What Is Medical Coding? Complete Guide 2026
The Qualigenix Editorial Team consists of certified billing and coding experts with over 40 years of experience across 38+ medical specialties. Our content is rigorously researched against CMS, AMA, and payer-specific guidelines to ensure total compliance and accuracy. We apply the same elite standards to our resources as we do our client work, consistently delivering high claim accuracy and significant reductions in AR days.
What Is Medical Coding? Complete Guide 2026
Last Updated: April 2026 | Includes FY 2026 ICD-10-CM Updates (487 New Codes), CPT 2026 Changes (418 Total), AI-Assisted Coding Trends & Accuracy Best Practices
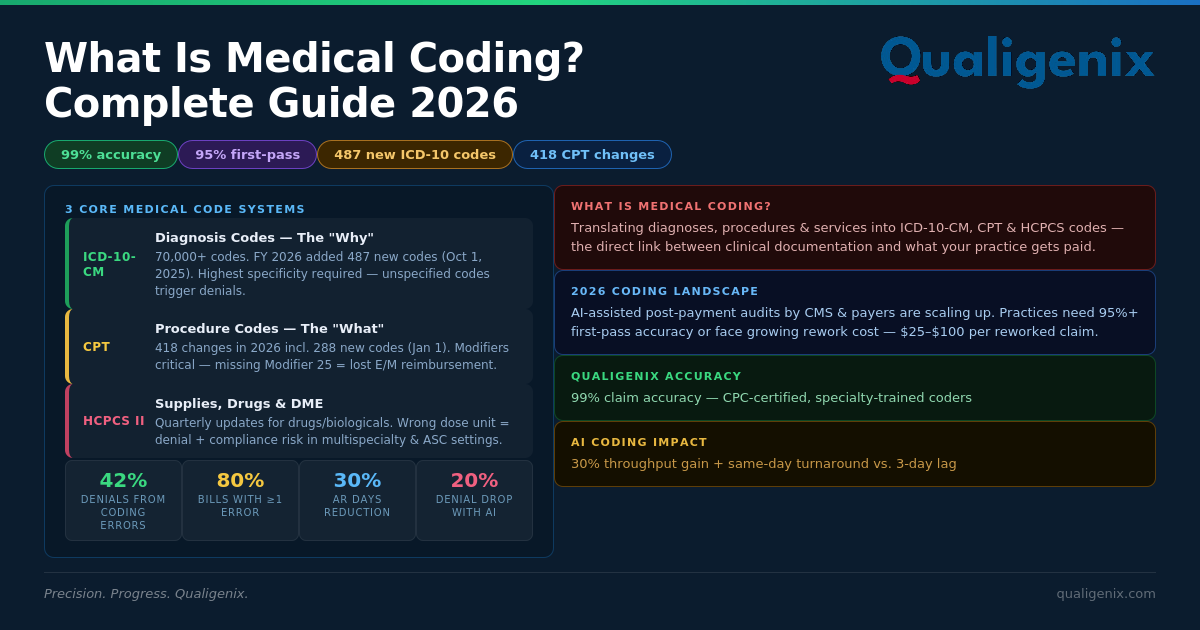
⚡ TL;DR — Key Takeaway: Medical coding is the process of converting clinical diagnoses, procedures, and services into standardized alphanumeric codes — ICD-10-CM, CPT, and HCPCS — that insurance payers use to adjudicate and reimburse claims. Coding errors are responsible for approximately 42% of all claim denials, and up to 80% of medical bills contain at least one error. In 2026, FY updates added 487 new ICD-10 codes and 418 CPT changes, making coding accuracy more consequential — and harder to maintain — than ever.
Every patient encounter generates a clinical story. A physician sees a 58-year-old with hypertension and stage 3 chronic kidney disease, orders labs, and adjusts their medication protocol. That clinical story — every diagnosis, every service, every supply used — must be translated into a precise string of alphanumeric codes before a single dollar of reimbursement flows from the insurer to the practice. That translation is medical coding.
Get the code right and the claim pays. Get it wrong — wrong specificity, wrong modifier, wrong code pair — and the claim denies. Approximately 42% of all claim denials trace back to coding errors (Sully.ai, 2026). Up to 80% of medical bills contain at least one error. For a practice submitting 500 claims per month at an average value of $300, moving from 75% first-pass accuracy to 95% first-pass accuracy represents $30,000 per month in claims your team no longer has to rework.
In 2026, the stakes are higher than they’ve ever been. The FY 2026 ICD-10-CM update added 487 new diagnosis codes effective October 1, 2025. CPT 2026 introduced 418 total changes including 288 new codes effective January 1, 2026. CMS and commercial payers are using AI-assisted post-payment audits to identify coding errors at scale. This guide covers everything your practice needs to know about medical coding in 2026 — and how Qualigenix medical coding services deliver 99% claim accuracy.
What Is Medical Coding?
Medical coding is the standardized process of translating healthcare diagnoses, procedures, medical services, and equipment into universal alphanumeric codes — ICD-10-CM for diagnoses, CPT for procedures and services, and HCPCS for supplies and drugs — that insurance payers use to process and reimburse claims. Accurate medical coding is the direct link between what a clinician documents and what the practice gets paid.
Think of medical coding as the universal language of healthcare billing. A physician might document “non-ST-elevation myocardial infarction with subsequent care, initial encounter” — but the payer doesn’t read prose, it reads code I21.4. Every diagnosis, every procedure, every injection, every device, every level of clinical complexity has a corresponding code. The medical coder’s job is to find the precise code that accurately represents what the documentation says, apply the correct modifiers, and ensure the diagnosis code supports the procedure code on the same claim.
Medical coding sits directly upstream of claim submission in the revenue cycle. If coding is wrong, the claim is wrong — and a wrong claim either gets denied immediately or creates audit exposure later during a post-payment review. This is why coding accuracy is the single highest-leverage metric in any RCM strategy. It’s cheaper to code it right the first time than to fix it after denial, appeal it through the payer’s review process, and risk write-off if the appeal window closes.
Medical Coding: Key Statistics and Benchmarks 2026
| Metric | Value / Benchmark |
|---|---|
| Claim denials caused by coding errors | ~42% of all denials (Sully.ai, 2026) |
| Medical bills containing at least one error | Up to 80% (industry research, 2026) |
| Total ICD-10-CM codes in use (US) | 70,000+ diagnosis codes |
| FY 2026 ICD-10-CM new codes | 487 new codes, 38 revisions, 28 deletions (effective Oct 1, 2025) |
| CPT 2026 total code changes | 418 changes including 288 new codes (effective Jan 1, 2026) |
| HCPCS Level II update frequency | Quarterly (drugs/biologicals); semi-annually (DMEPOS) |
| AI coding impact on denial reduction | ~20% denial reduction when ML combined with heuristic rules (Stanford Health Care) |
| Coding throughput improvement with AI | 30% increase in coding throughput (Medicodio case study) |
| AI + denial improvement — orthopedic example | 95% reduction in coding errors; 3-day lag to same-day turnaround (Medicodio) |
| Industry first-pass acceptance benchmark | 95% or higher (below this = revenue leakage from rework) |
| In-house coding accuracy (generalist) | 75–85% without specialty training or systematic QA |
| Qualigenix claim accuracy rate | 99% — CPC-certified, specialty-trained coders |
| Qualigenix first-pass acceptance rate | 95% — across all specialties and payer types |
| Qualigenix AR days reduction | 30% average — accurate coding = fewer denials = faster payment |
What Are the Three Main Medical Coding Systems?
Every claim submitted to a US insurance payer requires codes from at least two of the three primary code systems. Understanding what each system covers — and who maintains it — is foundational to understanding why coding errors are so common and so consequential.
ICD-10-CM — International Classification of Diseases, 10th Revision
Maintained by: CDC’s National Center for Health Statistics (NCHS). Effective date for 2026 updates: October 1, 2025.
ICD-10-CM codes answer the “why” of every clinical encounter — why was this patient seen, what conditions were diagnosed, what chronic diseases are being managed. Each code is an alphanumeric string of 3–7 characters, with greater length indicating greater specificity. A code like E11.9 means Type 2 diabetes mellitus without complications. E11.649 means Type 2 diabetes mellitus with hypoglycemia without coma — a far more specific and clinically meaningful statement.
In 2026, specificity is not optional. CMS and commercial payers require the highest level of ICD-10 specificity the documentation supports. Using an unspecified code when the medical record contains specific information is a coding error that can trigger denial, reduced reimbursement, or clawback during a RADV audit. The FY 2026 update added 487 new codes, with the most significant changes in Chapter 19 (Injury and Poisoning) and Chapter 12 (Skin and Subcutaneous Tissue Disorders). Behavioral health, post-COVID syndromes, and opioid use disorder coding also received expanded specificity requirements (Medical Healthcare Solutions, 2026).
CPT — Current Procedural Terminology
Maintained by: American Medical Association (AMA). Effective date for 2026 updates: January 1, 2026.
CPT codes answer the “what” — what procedure was performed, what service was rendered, what level of clinical complexity was involved. They’re five-digit numeric codes divided into six sections: Evaluation and Management (E/M), Anesthesia, Surgery, Radiology, Pathology/Laboratory, and Medicine. CPT 2026 introduced 418 total changes — 288 new codes, plus revisions and deletions — with a sharp focus on digital health, telehealth, and care coordination services.
CPT codes require accurate application of modifiers — two-digit alphanumeric codes that provide additional context about how a service was performed. A missing or incorrect modifier is one of the most common coding errors in specialty billing. For example, Modifier 25 (significant, separately identifiable E/M on the same day as a procedure) is frequently missing when a physician performs both an office visit and a minor procedure in the same encounter — causing the visit to bundle into the procedure and resulting in lost reimbursement.
HCPCS Level II — Healthcare Common Procedure Coding System
Maintained by: Centers for Medicare & Medicaid Services (CMS). Update frequency: Quarterly for drugs/biologicals; semi-annually for DMEPOS.
HCPCS Level II codes cover what CPT doesn’t — durable medical equipment (DME), prosthetics, orthotics, supplies, drugs, biologicals, and certain professional services. They’re alphanumeric codes beginning with a letter (A–V) followed by four digits. In multispecialty and ASC settings, HCPCS coding errors are particularly costly because dosage units, drug-specific billing rules, and DMEPOS supplier requirements all interact with payer-specific reimbursement policies. A biologic medication coded at the wrong dose unit can result in both denial and compliance risk (Medical Healthcare Solutions, 2026).
What Are the Most Important Medical Coding Updates for 2026?
Coding updates are not optional administrative housekeeping. They are regulatory requirements that take effect on fixed dates, and using outdated codes after those dates results in automatic claim rejection. In 2026, the volume and complexity of updates demand systematic training and workflow changes — not a one-time staff email about new codes.
FY 2026 ICD-10-CM Updates (Effective October 1, 2025)
The FY 2026 ICD-10-CM update added 487 new codes, revised 38 existing codes, and deleted 28 others. The most significant volume changes occurred in Chapter 19 (Injury, Poisoning and Certain Other Consequences of External Causes) and Chapter 12 (Diseases of the Skin and Subcutaneous Tissue). Practices in pain management, dermatology, and trauma surgery face the highest volume of new codes requiring immediate workflow integration.
COVID-19 documentation now requires exact code pairings when respiratory manifestations are present — providers must differentiate between lower respiratory infections, unspecified respiratory infections, pneumonia, and bronchitis using specific additional codes. Post-COVID condition coding received clarification distinguishing active symptoms after resolution from new active infections. Behavioral health diagnosis coding expanded significantly for opioid use disorder, autoimmune disorders, and post-COVID syndromes. Severity-based classifications in chronic conditions like heart failure and diabetes now impact risk adjustment and HCC coding for Medicare Advantage plans directly.
⚠ HCC and Risk Adjustment Impact: For Medicare Advantage plans and value-based contracts, a 1–3% drop in HCC (Hierarchical Condition Category) capture accuracy from failing to apply 2026 ICD-10 specificity requirements translates to millions in lost risk-adjustment payments annually (RAAPID Inc., 2026). Generic diagnosis codes like “heart failure, unspecified” (I50.9) that no longer map to HCCs under 2026 guidelines eliminate RAF scoring and downstream payment.
CPT 2026 Updates (Effective January 1, 2026)
CPT 2026 introduced 418 total changes — 288 new codes, plus revisions and deletions — with notable emphasis on digital health, precision procedures, and care coordination. Telehealth received significant expansion with a new telemedicine subsection adding codes for synchronous E/M services across new and established patients via both audio-video and audio-only platforms. CPT 98016 replaced HCPCS G2012 for brief virtual check-ins — practices that haven’t updated their billing workflows are filing claims with deleted codes, triggering automatic rejection.
Practices performing affected procedures must update charge masters and coding crosswalks. Relying on EHR “auto-updates” alone is insufficient — software updates don’t guarantee correct code application by clinical staff or coders who haven’t been trained on the clinical rationale behind the new codes (Medical Healthcare Solutions, 2026).
What Are the Most Common Medical Coding Errors That Cause Claim Denials?
Coding errors fall into two categories: errors of omission (missing information) and errors of commission (wrong information applied). Both cause denials, but they require different fixes. Understanding the error pattern in your practice — which the right billing partner surfaces through root-cause denial analysis — is the fastest path to improving first-pass acceptance rate.
- Unspecified ICD-10 codes where specificity is required: Using “heart failure, unspecified” (I50.9) when the documentation clearly states systolic heart failure (I50.2x) costs reimbursement and triggers payer review. In 2026, specificity isn’t just best practice — it’s required for HCC mapping and many commercial payer contracts.
- CPT-ICD-10 mismatch: The diagnosis code must clinically support the procedure code. An ICD-10 for a resolved condition billed with a surgical procedure for that condition triggers automatic medical necessity denial. This requires coders to understand clinical logic, not just code lookup.
- Missing or incorrect modifiers: Modifier omissions — particularly Modifier 25 (significant separate E/M), Modifier 51 (multiple procedures), and Modifier 59 (distinct procedural service) — cause either claim bundling (lost revenue) or medical necessity denials. Specialty surgery and multi-procedure encounters are most vulnerable.
- Unbundling: Billing separately for services that should be reported together under a global code violates National Correct Coding Initiative (NCCI) edits and triggers both denials and compliance risk. CMS NCCI edits are updated quarterly.
- Upcoding or downcoding: Upcoding (billing a higher complexity E/M than the documentation supports) creates audit liability. Downcoding (under-reporting complexity due to coder conservatism) is money left on the table. Both require specialty training and documentation review to correct.
- Coding from the charge sheet, not the clinical record: Using encounter forms or superbills without verifying the underlying clinical documentation leads to systematic errors when the pre-printed checkbox doesn’t match what was actually documented.
What Is the Revenue Impact of Coding Errors for a Typical Practice?
If your practice has a 15% denial rate and a 60% resubmission rate (industry average), you’re writing off or losing 6% of billed revenue to uncollected claims. For a $2M annual revenue practice, that’s $120,000 per year that systematically disappears — often without anyone identifying the root cause. Moving from 75% to 95% first-pass accuracy on 500 monthly claims at $300 average value recovers $30,000 per month in claims that no longer require rework.
How Is AI Changing Medical Coding in 2026?
AI-assisted coding tools entered mainstream healthcare in 2023–2024, and by 2026 they’ve fundamentally altered what’s possible in coding throughput and accuracy. Stanford Health Care’s research showed approximately 20% denial reduction when machine learning is combined with heuristic rule-based coding. Medicodio’s case study reported a 30% increase in coding throughput and a 95% reduction in coding errors in an orthopedic setting — with turnaround going from 3 days to same-day.
The practical implication: AI tools are not a replacement for human coders. For routine outpatient encounters, AI-assist tools accelerate throughput without sacrificing accuracy. For complex surgical cases, oncology billing, behavioral health documentation, or HCC risk adjustment coding, human expertise remains essential. Qualigenix uses AI-assisted tools as a productivity layer while maintaining CPC-certified human oversight for every coded claim — the combination that delivers 99% accuracy at scale.
What Certifications Do Medical Coders Need in 2026?
The most widely recognized medical coding certification in the US is the CPC (Certified Professional Coder) from AAPC, which covers outpatient and physician coding with specialty tracks available. For inpatient and hospital-based coding, the CCS (Certified Coding Specialist) from AHIMA is the standard. Specialty credentials include the COC (Certified Outpatient Coder), CCC (Certified Cardiology Coder), and CPMA (Certified Professional Medical Auditor). Each certification requires ongoing continuing education unit (CEU) requirements because the code set changes annually.
How Does Qualigenix Deliver 99% Medical Coding Accuracy?
Qualigenix’s medical coding services combine specialty-trained CPC-certified coders with a multi-layer quality assurance process that catches errors before they reach the clearinghouse. Every coded claim undergoes pre-submission scrubbing against payer-specific edit rules, NCCI edit validation, and diagnosis-to-procedure clinical logic checks. The result: a 99% claim accuracy rate that sustains a 95% first-pass acceptance rate across all payer types and specialties.
The coding team is trained continuously on ICD-10-CM, CPT, and HCPCS annual updates — not just at the start of each code year but throughout the year as quarterly HCPCS updates, CMS guidance clarifications, and commercial payer policy changes occur. When CMS published the FY 2026 ICD-10-CM changes effective October 1, 2025, Qualigenix’s coders had already completed training and updated workflows before the effective date — not after the first wave of denials arrived.
Equally important is the feedback loop between coding and clinical documentation. When Qualigenix coders identify documentation that doesn’t support the specificity required for a code, they flag it to the provider through structured query processes — not simply downcode to the safest option. That feedback loop improves clinical documentation quality over time, which means better coding accuracy, fewer denials, and lower audit risk on an ongoing basis. The medical coding services integrate directly with the denial management workflow — so coding patterns that drive specific denial types get identified and corrected at the source, not just managed claim-by-claim.
How Does Medical Coding Affect Audit Risk in 2026?
In 2026, CMS and commercial payers are using AI-assisted post-payment audits to review coded claims at a scale that was previously impossible with human reviewers alone. Practices that fail to apply new code specificity requirements, misapply modifiers, or use discontinued codes are increasingly exposed to overpayment recovery demands, which can reach back years and include interest penalties.
The safest audit defense is documentation that supports every code submitted — not code selection that stretches what the documentation actually says. Qualigenix’s documentation feedback process and pre-submission QA process are specifically designed to ensure that every coded claim has defensible clinical documentation behind it, so that if an audit notice arrives, the practice’s records support the codes billed.
Medical Coding Accuracy Checklist: 10 Steps to Protect Your Revenue
- ☐ Update ICD-10-CM code sets immediately on Oct 1 each year: FY 2026 codes are effective October 1, 2025. Any claims with date of service on or after that date must use 2026 codes. Using deleted codes triggers automatic rejection.
- ☐ Update CPT code sets on Jan 1 each year: CPT 2026 (418 changes including 288 new codes) is effective January 1, 2026. Update your charge master and fee schedule simultaneously.
- ☐ Verify ICD-10 specificity against documentation: Never use an unspecified code when the medical record supports a specific code. Specificity is required for HCC mapping, value-based contracts, and audit compliance.
- ☐ Validate CPT-ICD-10 pairs before submission: Every procedure code must be supported by a diagnosis code that establishes medical necessity. Review NCCI edits and LCD/NCD coverage policies for your specialty.
- ☐ Apply modifiers correctly on every multi-service claim: Modifier 25, 51, 59, and specialty-specific modifiers are systematically under-applied. Each missing modifier means lost reimbursement or denial.
- ☐ Code from clinical documentation — not superbills: Encounter forms are guides, not substitutes for the actual medical record. Code what the documentation says, not what the pre-printed checkbox suggests.
- ☐ Run NCCI edit checks before submission: CMS NCCI edits are updated quarterly. Unbundling errors trigger both denial and compliance risk. Pre-submission review is your first defense.
- ☐ Monitor denial reason codes by CPT family: If the same CPT code keeps denying for the same reason, that’s a coding pattern — not an isolated incident. Root-cause analysis identifies and corrects systematic errors.
- ☐ Train coding staff on specialty-specific nuance: Cardiology modifiers, behavioral health time-based coding, oncology drug coding, and surgical global periods all require specialty knowledge that generic training doesn’t cover.
- ☐ Implement a documentation feedback loop: When clinical documentation doesn’t support the specificity required for a code, query the provider. Improved documentation today means better coding, better reimbursement, and lower audit risk tomorrow.
Frequently Asked Questions About Medical Coding
What is medical coding?
Medical coding is the process of translating clinical diagnoses, procedures, and services from healthcare documentation into standardized alphanumeric codes — ICD-10-CM for diagnoses, CPT for procedures and services, and HCPCS Level II for supplies and drugs — that insurance payers use to adjudicate and reimburse claims. Coding accuracy is the direct link between clinical documentation and payment.
Medical coding happens after every clinical encounter — office visit, surgery, diagnostic test, procedure, or telehealth session — and before the claim leaves the billing system. Every code applied must match the clinical documentation and must logically support every other code on the same claim.
What is the difference between ICD-10, CPT, and HCPCS codes?
ICD-10-CM codes (maintained by CDC/NCHS) identify diagnoses — the ‘why’ of care. CPT codes (maintained by the AMA) identify outpatient procedures and services — the ‘what’ of care. HCPCS Level II codes (maintained by CMS) identify supplies, drugs, biologicals, and DME not covered by CPT. All three systems must align correctly on every claim for payer adjudication to succeed.
On a typical outpatient claim, you’ll have one or more ICD-10-CM codes identifying the patient’s diagnoses, one or more CPT codes identifying what was done, and sometimes HCPCS codes if supplies, drugs, or equipment were used. The payer reviews whether the diagnosis codes medically justify the procedure codes — a mismatch triggers denial regardless of everything else being correct.
What are the 2026 medical coding changes practices need to know?
FY 2026 ICD-10-CM updates (effective October 1, 2025) added 487 new codes, 38 revisions, and 28 deletions, with major changes in Chapter 19 (Injury/Poisoning) and Chapter 12 (Skin Disorders), plus expanded behavioral health, post-COVID, and chronic disease specificity. CPT 2026 (effective January 1, 2026) introduced 418 changes including 288 new codes, with significant additions for digital health, telehealth, and care coordination.
Practices that rely on EHR “auto-updates” alone risk applying codes correctly in their system while their coders and clinical staff misapply the underlying coding rules. Systematic training is required each year — not just a system software update.
How many medical billing and coding errors exist?
Up to 80% of medical bills contain at least one error, and approximately 42% of all claim denials are caused by coding errors specifically (Sully.ai, 2026). For a $2M annual revenue practice, a 15% denial rate with a 60% resubmission rate means approximately $120,000 per year lost to uncollected claims.
What is the difference between medical coding and medical billing?
Medical coding translates clinical documentation into standardized codes (ICD-10-CM, CPT, HCPCS) that represent diagnoses and services. Medical billing uses those codes to create and submit claims to insurance payers and manage the collection process. Coding happens first; billing follows. Both must be accurate for the claim to pay.
In many practices, one person does both coding and billing — which creates a workload problem because both are full-time specialties done well. Separating the functions, or outsourcing both to a specialist like Qualigenix, ensures each step gets dedicated expert attention.
How does Qualigenix ensure coding accuracy?
Qualigenix maintains 99% claim accuracy through CPC-certified specialty-trained coders, multi-layer pre-submission claim scrubbing, continuous ICD-10 and CPT update training, payer-specific coding rule libraries, NCCI edit validation, and a structured documentation feedback loop. This results in a 95% first-pass acceptance rate across all specialties.
The documentation feedback loop is particularly important. When a coder identifies documentation that doesn’t support the required code specificity, they flag it to the provider with a structured query — improving clinical documentation quality over time rather than simply coding to the lowest defensible option.
Related Qualigenix Resources
Service Pages:
- Medical Coding Services — 99% accuracy, CPC-certified specialty coders
- CPT and ICD-10 Coding Services
- HCPCS Coding Services
- Medical Coding Consulting
- Denial Management Services
- Claim Submission Services
Blog Guides:
- Medical Billing vs. Medical Coding: The Difference
- Clean Claim Rate: Benchmarks & Best Practices
- Medical Necessity Documentation Mistakes to Avoid
- Charge Capture Errors & How to Fix Them
- Denial Management Process: 5 Essential Steps
- How to Reduce Medical Claim Denials: Your 2026 Guide
- Healthcare Billing Process Explained: End-to-End Workflow
- What Is Revenue Cycle Management? A Beginner’s Guide
Stop Losing Revenue to Coding Errors. Start Today.
Qualigenix’s CPC-certified specialty coders deliver 99% claim accuracy and 95% first-pass acceptance across 38+ specialties. With 6-day onboarding and an immediate coding audit, you’ll know exactly where your revenue is leaking — and we’ll fix it.
Our team delivers 99% claim accuracy, a 95% first-pass acceptance rate, and an average 36-day collection cycle. We onboard in as few as 6 days.
Precision. Progress. Qualigenix.
What’s Next

Denial Management in 2026: The Top 10 Codes and the Appeal Playbook for Each
Denials cluster around a small set of codes, and each one has a different correct response. Some need a...
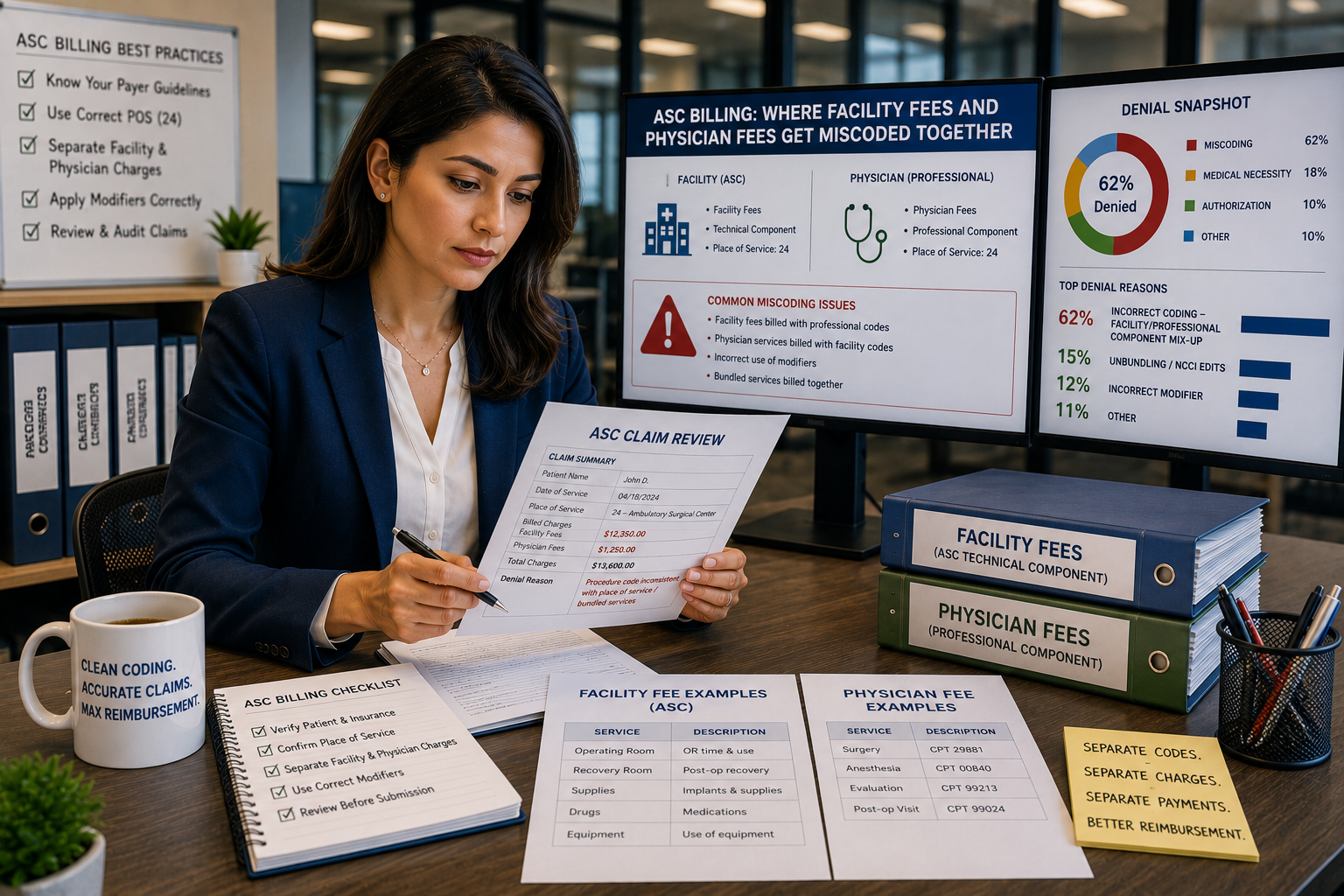
ASC Billing: Where Facility Fees and Physician Fees Get Miscoded Together
ASC facility and physician claims both go out on a CMS-1500 form with the same CPT code and place...
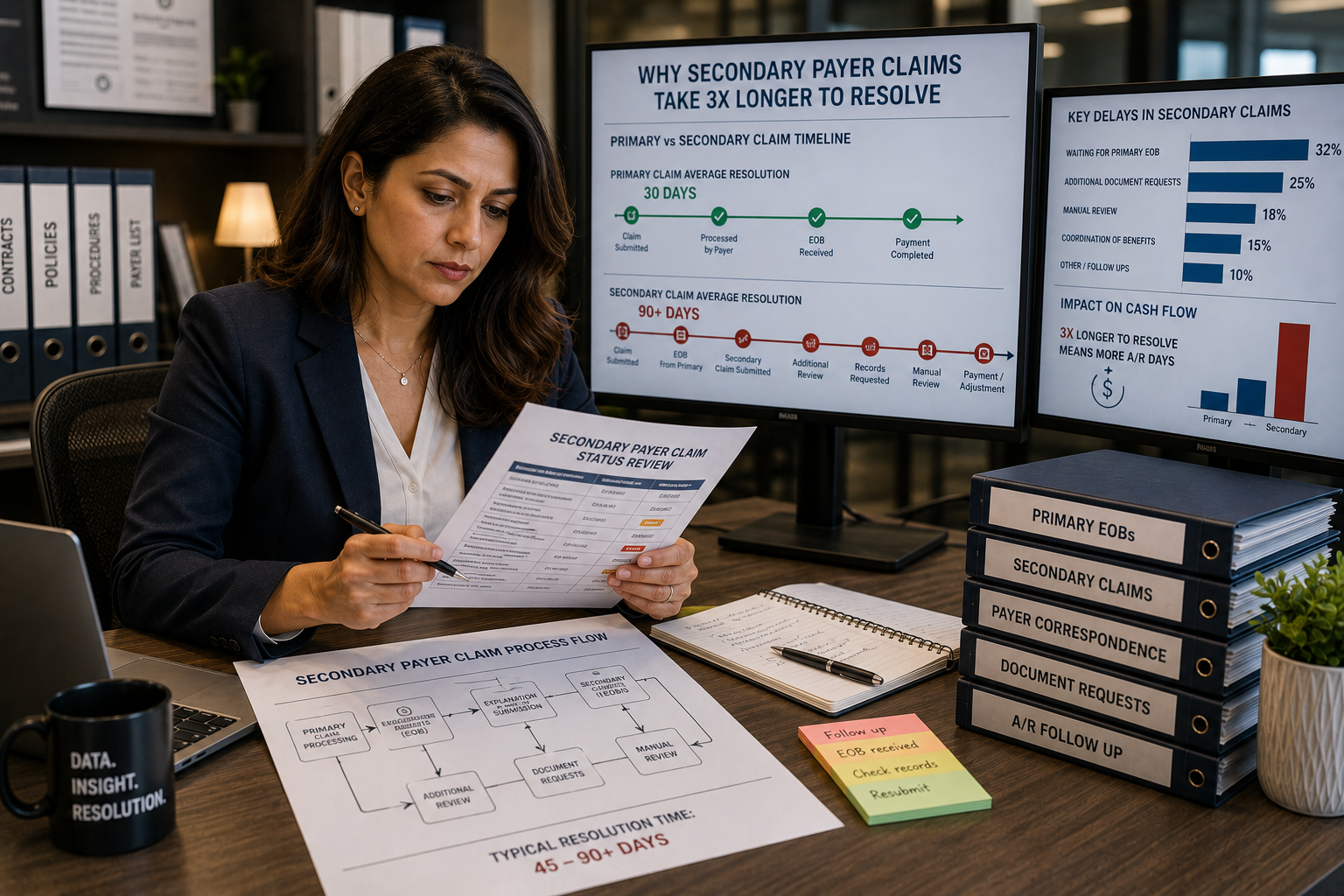
Coordination of benefits errors: why secondary payer claims take 3x longer to resolve
Secondary payer claims stall because coordination of benefits errors, wrong payer order, outdated COB records, and missing primary...