What Is Revenue Cycle Management? Guide for Healthcare Providers
The Qualigenix Editorial Team consists of certified billing and coding experts with over 40 years of experience across 38+ medical specialties. Our content is rigorously researched against CMS, AMA, and payer-specific guidelines to ensure total compliance and accuracy. We apply the same elite standards to our resources as we do our client work, consistently delivering high claim accuracy and significant reductions in AR days.

Revenue cycle management (RCM) is the end-to-end financial process that connects patient care to payment. Weak RCM means delayed payments, high denial rates, and cash flow strain. In medical billing, it is the operational engine that turns clinical services into collected revenue. This guide covers the full 8-step process, the 5 KPIs every provider must track, how RCM works differently across settings, and how Qualigenix clients achieve a 99% claim accuracy rate, 95% first-pass acceptance, and a 30% reduction in AR days.
A patient walks into your office. You deliver excellent care. They leave satisfied. Then the billing starts — and somewhere between the encounter and the payment, revenue disappears.
A coding error triggers a denial. An eligibility gap causes a rejection. An aging claim sits unanswered in accounts receivable for 60 days. This is not rare. According to the Healthcare Financial Management Association, U.S. healthcare providers lose more than $125 billion annually to billing errors and inefficient revenue cycle processes.
Revenue cycle management fixes this. It is the system that ensures every service gets documented, coded, billed, and collected — accurately and on time. Whether you run a solo family practice or a multi-specialty group, your financial health depends on how well your revenue cycle performs.
This guide explains what RCM is, how it works in healthcare and medical billing, what the process looks like step by step, and what you should be measuring to know if yours is working.
Revenue cycle management (RCM) is the end-to-end administrative and financial process healthcare providers use to track patient care from initial registration through final payment. It includes insurance eligibility verification, medical coding, claim submission, denial management, payment posting, and patient collections — connecting every clinical encounter to the revenue it generates.
Why Revenue Cycle Management Matters More Than Ever in 2026
Healthcare reimbursement has never been more complex. Payer rules change constantly. Prior authorization requirements expand every year. Patient financial responsibility keeps rising as high-deductible health plans become the norm. And the administrative burden on billing teams grows without a corresponding increase in staff or technology.
The result is predictable. The average medical practice has a denial rate between 5 and 10%, according to MGMA. Medicare Advantage plans deny nearly one in five claims at first submission. And 65% of denied claims are never reworked — they get written off as bad debt.
Every percentage point of denial rate improvement translates directly to recovered revenue. A practice billing $2 million annually with a 10% denial rate and a 65% write-off rate loses roughly $130,000 per year to claims that were never corrected. That is not a billing problem. That is a revenue cycle management problem.
Strong RCM is not a back-office nicety. It is a core business function — as essential to a practice’s survival as the clinical care it delivers.
Revenue Cycle Management Benchmarks: Where Does Your Practice Stand?
| RCM Metric | Underperforming | Industry Benchmark | High-Performing | Qualigenix |
|---|---|---|---|---|
| Clean Claim Rate | Below 85% | 90–94% | 95%+ | 95% |
| Denial Rate | Above 10% | 5–7% | Below 5% | <5% |
| Days in AR | Above 50 days | 35–50 days | 30–35 days | 36 days avg. |
| Net Collection Rate | Below 90% | 92–95% | 96%+ | Optimized per specialty |
| Cost to Collect | Above 5% of net revenue | 3–5% | Under 3% | 4–9% of collections (outsourced) |
| Claim Accuracy Rate | Below 88% | 90–95% | 96%+ | 99% |
| AR Over 90 Days | Above 25% of total AR | 15–20% | Under 15% | Aggressively worked |
| Denied Claims Never Reworked | 65% (industry avg.) | Below 20% | Under 10% | Systematic follow-up on all |
| Cost to Rework a Denied Claim | $118 | $25–$60 | Under $25 | Minimized via prevention |
| Medicare Advantage Denial Rate | Above 25% | ~20% at first submission | Below 10% | Managed with payer-specific rules |
| Annual Revenue Lost (US) | $125 billion+ | Recoverable with right RCM | ||
| Avg. Onboarding (outsourced RCM) | 4–6 weeks | 2–4 weeks | Under 2 weeks | As few as 6 days |
| Specialties Requiring Specialty Coding | All specialties | — | — | 38+ covered |
| AR Days Reduction Post-Outsourcing | — | 15–20% | 25–35% | 30% |
Sources: MGMA Cost and Revenue Survey 2025; HFMA Revenue Cycle Benchmark Report 2025; CMS National Health Expenditure Data 2025; Qualigenix internal performance data 2026.
Revenue Cycle Management in Healthcare: How It Works Across Settings
RCM looks different depending on the care setting. A solo physician practice, a multi-specialty group, a hospital system, and a telehealth provider all face different billing environments, payer mixes, and workflow challenges. What stays constant is the goal: every service delivered to every patient must generate the correct payment, collected as quickly as possible.
RCM in Hospital Systems
Hospital RCM operates at significant scale and complexity. A large health system may submit tens of thousands of claims per day across inpatient, outpatient, emergency, and ancillary service lines. Each service line has different coding requirements — inpatient claims use DRG-based coding under IPPS, while outpatient claims use APC-based coding under OPPS.
Hospitals also manage dual billing — facility claims (UB-04) and professional claims (CMS-1500) for the same encounter. A surgeon operating at a hospital generates both a professional fee claim under their individual NPI and a facility fee claim under the hospital’s NPI. Both need separate coding, submission, and reconciliation.
Hospital RCM teams are typically large, specialized departments. Patient access, coding, billing, follow-up, and analytics often operate as distinct functions. The claim volume requires enterprise-grade technology — automated eligibility verification, real-time claims monitoring dashboards, and sophisticated denial analytics.
RCM in Physician Group Practices
For physician groups — whether a 3-provider family medicine practice or a 50-provider multi-specialty group — RCM is simpler in structure but equally critical in execution. Group practices submit professional claims only (CMS-1500), focused on a defined specialty or set of specialties.
The challenge for group practices is bandwidth. With smaller billing teams, every error costs proportionally more in staff time. A denied claim that takes two hours to research, correct, and resubmit represents a significant chunk of a small team’s daily capacity. This is why denial prevention delivers outsized returns at the group practice level — stopping the problem before it starts costs far less than fixing it after.
RCM for Telehealth Providers
Telehealth RCM added complexity after the COVID-19 public health emergency. The temporary billing flexibilities during the PHE have partly become permanent — but payer-by-payer rules vary significantly.
Telehealth billing requires correct Place of Service code selection — POS 02 for telehealth provided other than in the patient’s home, POS 10 for telehealth in the patient’s home — and the appropriate GT or 95 modifiers depending on the payer. Incorrect POS coding on telehealth claims is one of the leading causes of telehealth-specific denials.
What is revenue cycle management in healthcare vs. in a medical office?
RCM in healthcare refers to the financial process across all care settings — hospitals, outpatient clinics, telehealth platforms, and long-term care facilities. In a medical office or physician practice, RCM focuses specifically on professional billing — coding encounters, submitting CMS-1500 claims, managing payer follow-up, and collecting patient balances. The goals are the same. The scale, tools, and team structures differ.
Revenue Cycle Management in Medical Billing: The Billing Team’s Role
If healthcare RCM is the full system, revenue cycle management in medical billing is the operational engine inside it. Medical billing is where the financial transactions actually happen — where clinical documentation becomes coded claims, coded claims become submitted bills, and submitted bills become collected payments.
The medical billing team sits at the intersection of clinical documentation and financial outcomes. Their work directly determines how much revenue the practice collects and how quickly it arrives.
Front-End vs. Back-End Medical Billing
Medical billing divides into front-end and back-end functions. Both must work well for the revenue cycle to perform.
Front-end medical billing covers everything before and during the patient encounter: patient registration, insurance eligibility verification, prior authorization, co-pay collection at the point of service, and demographic verification. Front-end errors cause the majority of back-end denials. A wrong insurance ID entered at registration creates a denial 7 to 14 days later when the claim is adjudicated.
Back-end medical billing covers everything after the encounter: charge capture, coding, claim submission, clearinghouse processing, payment posting, denial management, appeals, and patient billing. Back-end work responds to what the front end sends downstream. A high-performing back-end team can catch and correct some front-end errors — but prevention always costs less than correction.
The Role of Medical Coders in RCM
Medical coders are the bridge between clinical documentation and financial claims. They review physician notes, operative reports, and diagnostic results and translate them into standardized codes — CPT codes for procedures and services, ICD-10-CM codes for diagnoses, and HCPCS Level II codes for supplies and certain services.
Coding accuracy is the single biggest driver of clean claim rate. A claim with wrong or missing diagnosis codes gets denied for medical necessity. A claim with an incorrect CPT code gets denied for incorrect billing. A claim missing a required modifier gets rejected before adjudication begins.
Specialty-specific coding knowledge matters enormously. The coding rules for interventional radiology, behavioral health, wound care, and orthopedic surgery are all different — different bundling rules, different modifier requirements, different documentation standards. A generalist coder working in an unfamiliar specialty produces systematic errors that compound into meaningful revenue loss over time.
What is the difference between medical billing and revenue cycle management?
Medical billing is a component of revenue cycle management — specifically the claim submission and collections process. RCM is the broader system that includes patient registration, eligibility verification, clinical documentation, coding, billing, denial management, payment posting, and analytics. Billing without strong front-end RCM produces unnecessary denials. RCM without strong billing execution produces slow collections.
The 8-Step Revenue Cycle Management Process
Every successful revenue cycle follows the same eight steps. Each step feeds into the next. A failure at any point creates downstream problems that cost money and time to resolve.
Step 1: Patient Registration and Scheduling
The revenue cycle starts before the patient arrives. Accurate demographic collection — full legal name, date of birth, address, and primary and secondary insurance information — is the foundation every subsequent step builds on. A single transposed digit in a policy number can cause a claim rejection days later that takes hours to diagnose and fix.
Best practice is to collect and verify registration data at the time of scheduling, not at check-in. This gives the billing team time to catch errors and verify coverage before the appointment — not after the service is already delivered.
Step 2: Insurance Eligibility Verification
Eligibility verification confirms that the patient’s insurance is active, what services are covered, what the co-pay and deductible amounts are, and whether the planned service requires prior authorization. Verify for every patient before every appointment — not just new patients.
Coverage lapses, plan changes, and benefits exhaustion happen regularly. Catching them before the appointment prevents both the denial and the difficult conversation with the patient about an unexpected bill.
Our insurance eligibility verification services check every patient before every appointment — automatically, in real time, with no additional burden on your front desk.
Step 3: Clinical Documentation and Coding
After the encounter, the physician’s documentation gets translated into billable codes. Coding accuracy determines claim fate. CPT codes must correctly describe the service. ICD-10-CM diagnosis codes must support medical necessity for the CPT codes billed. The two must link correctly — the diagnosis must justify the procedure.
Common coding errors include upcoding, undercoding, unbundling, and missing modifiers. Our medical coding services cover 38+ specialties with specialty-trained coders who know the payer-specific rules for each code set.
Step 4: Charge Capture and Entry
Charge capture records every billable service from the encounter into the billing system. Services documented but not captured generate no claim and no revenue. Unlike a denied claim, a missed charge produces no error message — it simply disappears.
Common gaps include procedures documented but not entered as charges, supplies used but not billed, and E&M services coded at a lower level than documentation supports. Regular charge capture audits — comparing clinical documentation to billed charges — identify and close these gaps.
Step 5: Claim Submission and Scrubbing
Before a claim leaves your system, scrub it against payer-specific editing rules. Claim scrubbing checks for correct patient demographics, valid code combinations, required modifiers, diagnosis-to-procedure linkage, and payer-specific billing requirements.
A claim that passes scrubbing goes out clean. A clean claim reaches the payer, gets adjudicated, and generates payment — typically within 14 to 30 days for electronic claims. A claim that skips scrubbing and goes out with errors gets rejected or denied. Rework costs $25 to $118 per claim and delays payment by weeks or months.
Our claim submission services include pre-submission scrubbing against both clearinghouse edits and payer-specific rules — the combination that delivers our 95% first-pass acceptance rate.
How long does it take for a clean claim to be paid?
Electronic clean claims are adjudicated within 14 to 30 days by commercial payers. Medicare pays clean electronic claims within 14 days. Medicaid timelines vary by state — typically 21 to 30 days. Claims with errors take 45 to 90 days or longer after rework and resubmission.
Step 6: Payment Posting and Reconciliation
When the payer sends payment, the billing team posts it against the original claim. Payment posting records what the payer paid, what adjustments were made, and what remains as patient responsibility. This step is also a quality control checkpoint.
Accurate payment posting catches underpayments — instances where a payer paid less than the contracted rate. Payers process millions of claims and occasionally apply the wrong fee schedule or miss a modifier. Without careful reconciliation, underpayments go undetected and unchallenged.
Our payment posting services reconcile every EOB and ERA against contracted rates — flagging underpayments and initiating follow-up before the appeal window closes.
Step 7: Denial Management and Appeals
Denial management identifies denied claims, determines root causes, corrects errors, and resubmits within payer timely filing deadlines. It also performs root cause analysis to prevent the same denial type from recurring.
Most practices react to individual denials but never aggregate them. Aggregation is where the value is. If 40% of your denials share a single reason code from one payer, that pattern points exactly to where you need to fix your front-end process. Without that analysis, you rework the same denials month after month without solving the underlying problem.
Our denial management services combine rapid rework with systematic root cause analysis — reducing both current denials and future denial rates in a continuous improvement loop.
Step 8: Patient Billing and Collections
After insurance adjudication, the remaining patient balance — co-pays, deductibles, co-insurance, and non-covered services — must be billed and collected. High-deductible health plans have shifted more financial responsibility onto patients, making this step increasingly important.
Clear, readable statements improve payment rates. Multiple payment options — online, by phone, by mail, and payment plans for larger balances — remove barriers to payment. Collecting co-pays and known deductible amounts at the time of service is the single most effective patient collection strategy — it eliminates the need to bill separately and avoids the lower collection rates that apply to post-service patient billing.
RCM KPIs: The 5 Metrics Every Practice Must Track
You cannot manage what you do not measure. These five KPIs give you a complete picture of your revenue cycle’s health — where money flows in, where it leaks out, and how efficiently your team is working.
1. Clean Claim Rate
Clean claim rate measures the percentage of claims paid on the first submission without correction. Formula: (Claims paid on first submission / Total claims submitted) × 100. Target: 95% or higher.
A rate below 90% means at least 10% of your claims bounce back for correction. Each costs $25 to $118 to rework and delays payment by weeks. The root causes — coding errors, patient data problems, missing modifiers, payer rule gaps — are almost always systematic and fixable.
2. Days in Accounts Receivable
Days in AR measures how long it takes, on average, to collect payment after a service is delivered. Formula: (Total AR Balance / Average Daily Charges). Target: 30 to 35 days. Practices above 50 days experience significant cash flow strain.
High AR days usually trace to high denial rates slowing payment, inadequate follow-up on unpaid claims, slow patient collections, or staffing gaps in the billing department.
3. Denial Rate
Denial rate measures the percentage of submitted claims payers deny. Formula: (Denied claims / Total claims submitted) × 100. Target: below 5%. Industry average: 5 to 10%. Many small practices without dedicated billing staff run denial rates of 10 to 15% or higher.
Track denial rates by payer and by denial reason code. The combination tells you which payers deny most frequently and exactly why — the data you need to target process improvements where they will have the greatest impact.
4. Net Collection Rate
Net collection rate measures how much of your collectible revenue you actually collect. Formula: (Payments collected / (Charges – Contractual adjustments)) × 100. Target: 95% or higher. A rate below 90% indicates significant revenue leakage.
Net collection rate is the most honest measure of revenue cycle effectiveness. A high gross collection rate can mask problems if contractual adjustments are misapplied. Net collection rate cuts through and shows you the real number.
5. Cost to Collect
Cost to collect measures how much you spend per dollar of revenue collected. Formula: (Total billing costs / Net collections) × 100. Target: under 3% of net revenue. Practices with high denial rates and manual billing processes often run cost-to-collect ratios of 5% or higher.
For outsourced billing, the cost to collect is the outsourcing fee — typically 4 to 9% of collections. This is often lower than in-house costs when you factor in salary, benefits, training, software, and the hidden cost of denied claims that no one is working.
What is a good denial rate for a medical practice?
A denial rate below 5% is the benchmark for high-performing practices. The industry average is 5 to 10%. Small practices without dedicated billing staff often run 10 to 15% or higher. Every percentage point above 5% represents preventable revenue loss and staff time spent on rework that better front-end processes and claim scrubbing could eliminate.
Top RCM Challenges and How to Overcome Them
Every practice faces revenue cycle challenges. The ones that fall behind treat these challenges as inevitable. The ones that pull ahead treat them as solvable process problems.
Challenge 1: High Denial Rates
High denial rates are the most visible and most expensive RCM problem. Every denied claim represents a service already delivered that has not been paid — and may never be paid if not reworked quickly.
The most common denial causes: incorrect or missing patient demographic information (15 to 20% of denials), coding errors including wrong CPT codes and missing modifiers (25 to 30%), missing or expired prior authorizations (10 to 15%), untimely filing (10%), and eligibility issues (10 to 15%).
Warning: Untimely filing denials are permanently unrecoverable. Once a payer’s filing deadline passes, the claim cannot be resubmitted or appealed. Most commercial payers allow 90 to 180 days from the date of service. Some allow up to one year. Know your payer-specific deadlines and track them. Every day of delay on a denied claim increases the risk of missing the window entirely.
Challenge 2: Staffing Gaps and Turnover
Medical billing is a specialized skill that takes time to develop. Experienced billers who know payer-specific rules, can work denials efficiently, and understand specialty-specific coding are difficult to find and expensive to keep. When a billing team member leaves, collections can stall for weeks while a replacement is found and trained.
Cross-train billing staff on multiple payer types and denial categories so no single person holds critical knowledge. Document all processes in writing. Consider outsourcing as a stability strategy — an outsourced partner provides team-based coverage with no single point of failure, regardless of vacation, sick leave, or turnover.
Challenge 3: Prior Authorization Burden
Prior authorization requirements have expanded dramatically over the past decade. The American Medical Association reports that physicians and their staff spend an average of 14.6 hours per week on prior authorization tasks. Incomplete or missing authorizations are one of the fastest-growing causes of denials — and these denials are among the hardest to appeal.
Build authorization tracking into your scheduling workflow. Check authorization requirements when the appointment is booked, not the day before. Use payer portals and electronic authorization systems to reduce manual phone-based processes.
Challenge 4: Payer Contract Complexity
A typical medical group has 10 to 25 active payer contracts. Each one has different fee schedules, coverage rules, billing requirements, and timely filing deadlines. Keeping up with contract changes — and ensuring your billing team knows the rules for each payer — is a constant challenge.
Maintain a payer rule library updated whenever you receive contract amendments or payer policy bulletins. Schedule quarterly contract reviews to verify fee schedules are current. Identify underpayments by reconciling payments against contracted rates for every payer.
Challenge 5: Technology Gaps
Many practices run revenue cycle operations on outdated practice management systems that lack real-time eligibility verification, automated claim scrubbing, and denial management dashboards. Manual billing processes are slower, more error-prone, and more dependent on individual staff knowledge than automated ones.
Invest in a practice management system with integrated eligibility verification and claim scrubbing. If a full system upgrade is not feasible, add clearinghouse-level scrubbing as a middle layer between your billing system and the payer. Even simple spreadsheet-based denial tracking is better than no tracking at all.
In-House RCM vs. Outsourced Revenue Cycle Management
The decision to manage RCM in-house or outsource it to a specialist is one of the most important financial decisions a practice makes. Neither option is universally right — the best choice depends on your practice size, specialty, billing volume, and current performance.
| Factor | In-House RCM | Outsourced RCM |
|---|---|---|
| Monthly Cost | $4,500–$8,000+ (salary + benefits + software) | 4–9% of collections |
| Coverage During Staff Absence | None — collections stall | Continuous — team-based model |
| Specialty Coding Expertise | Limited to what in-house staff knows | Built-in across 38+ specialties |
| Denial Follow-Up | Often reactive and inconsistent | Systematic — tracked per claim |
| Payer Rule Updates | Managed manually, often delayed | Maintained proactively by billing team |
| Monthly Reporting and Analytics | Manual, often incomplete | Dashboard + KPI reports included |
| Scalability | Requires new hires as volume grows | Scales automatically with volume |
| Clean Claim Rate | 75–88% (typical small practice) | 95%+ with specialist partner |
| Best For | Large practices with dedicated RCM staff | Small to mid-size practices and high-denial specialties |
Should a small practice outsource revenue cycle management?
For most small practices, yes. Outsourcing eliminates salary, training, and software costs, replaces single-point-of-failure in-house teams with team-based coverage, and delivers specialist-level billing performance. The 4 to 9% outsourcing fee is typically offset by improved collections and lower denial rates within the first 90 days. Qualigenix clients average a 30% reduction in AR days after outsourcing.
RCM Best Practices: What High-Performing Practices Do Differently
High-performing practices do not have better luck. They have better processes. These are the specific practices that consistently separate top-performing revenue cycles from average ones.
Verify Eligibility Before Every Appointment
Insurance coverage changes constantly. Patients switch jobs, age off parents’ plans, exhaust mental health benefits, and change payers between visits. Verifying eligibility only at registration or only for new patients creates a gap that produces front-end denials for established patients. Verify every patient before every scheduled appointment — automatically, using real-time clearinghouse verification.
Use Claim Scrubbing at Every Submission Point
The most expensive claim errors are the ones that reach the payer. Pre-submission claim scrubbing at both the practice management system level and the clearinghouse level creates two quality checkpoints that catch most errors before they become denials.
Work Denials Within 48 Hours of Receipt
The longer a denial sits unworked, the higher the risk of missing a timely filing deadline. High-performing billing teams triage denials daily — categorizing by denial reason, assigning rework priority, and tracking progress to resolution. Denied claims older than 30 days without action represent a material write-off risk.
Pro Tip: Sort your denial queue by payer timely filing deadline, not by date received. The denial closest to its filing deadline should be worked first — regardless of when it arrived. A denial received today from a payer with a 90-day window is more urgent than a denial received last week from a payer with a 365-day window.
Track KPIs Monthly and Set Improvement Targets
Practices that review KPIs monthly catch problems when they are small. A denial rate that ticks up from 6% to 9% over three months signals a specific process breakdown that is identifiable and correctable quickly if you are looking for it. Practices that review annually catch the same problem after losing a full year of revenue.
Perform Root Cause Analysis on Denial Patterns
The goal of denial management is not to rework denials faster. The goal is to prevent them from occurring. Root cause analysis — aggregating denials by reason code, payer, and provider to identify patterns — makes prevention possible. A denial pattern accounting for 30% of your denials can often be resolved with a single process change.
How Qualigenix Delivers Revenue Cycle Management Results
At Qualigenix, we build revenue cycle management programs around measurable outcomes. Every client relationship starts with a baseline audit of current denial rates, AR days, clean claim rate, and net collection rate. We set specific improvement targets and track performance against them monthly.
Our revenue cycle management services cover the complete billing cycle: eligibility verification, coding across 38+ specialties, clean claim submission, denial management, AR follow-up, payment posting, and patient billing. We integrate with your existing EHR and practice management system — no workflow disruption on the clinical side.
For practices that need full outsourcing, our medical billing outsourcing services provide team-based billing coverage with no single point of failure. Our clients average a 30% reduction in AR days within the first quarter and a 99% claim accuracy rate from day one.
We also offer standalone services for practices that need targeted help — denial management for practices with rising denial rates, AR follow-up for practices with aging receivables, and medical coding for practices that need specialty-specific coding support without full outsourcing.
Revenue Cycle Management Checklist
- ☐ Patient demographics verified for accuracy at every registration
- ☐ Insurance eligibility verified for every patient before every appointment
- ☐ Prior authorization tracked and obtained before every service requiring it
- ☐ Charge capture audited monthly against clinical documentation
- ☐ Claims scrubbed against payer-specific rules before every submission
- ☐ Clean claim rate tracked monthly (target: 95%+)
- ☐ Denied claims worked within 48 hours of receipt
- ☐ Denial reason codes aggregated monthly for root cause analysis
- ☐ Payments reconciled against contracted rates for every payer
- ☐ AR aging reviewed weekly — claims over 60 days escalated
- ☐ Patient balances billed within 14 days of insurance adjudication
- ☐ Monthly KPI report reviewed: denial rate, AR days, clean claim rate, net collection rate
Revenue Cycle Management Glossary
Revenue Cycle Management (RCM)
The end-to-end administrative and financial process healthcare providers use to track patient care from initial registration through final payment. It includes eligibility verification, clinical documentation, coding, claim submission, denial management, payment posting, and patient collections. Strong RCM connects every clinical encounter to the revenue it is entitled to generate.
Clean Claim Rate (First-Pass Rate)
The percentage of claims paid by a payer on the first submission without correction. Formula: (Claims paid on first submission / Total claims submitted) × 100. Target: 95% or higher. A rate below 90% signals systematic coding, data, or payer rule compliance problems generating preventable revenue delays.
Days in Accounts Receivable (AR Days)
The average number of days between service delivery and payment receipt. Formula: (Total AR Balance / Average Daily Charges). Target: 30 to 35 days for high-performing practices. AR days above 50 indicate cash flow strain, high denial rates, or inadequate follow-up on unpaid claims.
Denial Management
The systematic process of identifying denied claims, determining root causes, correcting errors, and resubmitting within payer timely filing deadlines. Effective denial management also includes aggregating denial reason codes to identify patterns and implement front-end process fixes that prevent the same denial types from recurring.
Net Collection Rate
The percentage of collectible revenue actually collected after contractual adjustments. Formula: (Payments / (Charges – Contractual Adjustments)) × 100. Target: 95% or higher. Rates below 90% indicate revenue leakage from written-off patient balances, unchallenged underpayments, or abandoned denied claims.
Prior Authorization
Advance approval required from a payer before delivering certain services, procedures, or medications. Failure to obtain required prior authorization is one of the most common — and most expensive — causes of claim denials. Prior authorization denials are often non-appealable, making prevention the only effective strategy.
Charge Capture
The process of recording all billable services from a patient encounter into the billing system. Missed charge capture generates no error message and no claim — the service simply goes unbilled. Regular charge capture audits comparing clinical documentation to billed charges are the primary tool for identifying and closing these gaps.
Frequently Asked Questions: Revenue Cycle Management
What is revenue cycle management?
Revenue cycle management is the end-to-end process healthcare providers use to track patient care from registration through final payment. It covers eligibility verification, coding, claim submission, denial management, payment posting, and patient collections — ensuring every service generates the revenue it is entitled to.
What is revenue cycle management in healthcare?
Revenue cycle management in healthcare refers to the complete financial lifecycle of a patient account across all care settings — hospitals, outpatient clinics, telehealth platforms, and physician practices. It spans clinical documentation, administrative workflows, and financial operations, connecting every patient encounter to the payment it generates.
What is revenue cycle management in medical billing?
Revenue cycle management in medical billing refers to the billing-side workflows that generate payer reimbursement — charge capture, CPT and ICD-10 coding, claim submission, denial management, payment posting, and patient collections. It is the operational engine that converts clinical documentation into collected revenue.
What are the 8 steps of the revenue cycle?
The 8 steps are: (1) Patient registration and scheduling, (2) Insurance eligibility verification, (3) Clinical documentation and coding, (4) Charge capture and entry, (5) Claim submission and scrubbing, (6) Payment posting and reconciliation, (7) Denial management and appeals, and (8) Patient billing and collections. Each step feeds the next — a failure at any point creates downstream revenue loss.
What RCM KPIs should I track?
Track these five: Clean Claim Rate (target 95%+), Days in AR (target 30–35 days), Denial Rate (target under 5%), Net Collection Rate (target 95%+), and Cost to Collect (target under 3% of net revenue). Together they show how efficiently your revenue cycle converts services into collected cash.
What is a clean claim rate and why does it matter?
Clean claim rate is the percentage of claims paid on first submission. The benchmark is 95%+. A rate below 90% means at least 10% of your claims get denied and reworked — costing $25 to $118 each and delaying payment by weeks. Improving clean claim rate is the highest-ROI improvement most practices can make to their billing process.
What causes high denial rates in medical billing?
The top causes are: wrong patient insurance information (15–20% of denials), coding errors including wrong CPT codes and missing modifiers (25–30%), missing prior authorizations (10–15%), eligibility issues (10–15%), and untimely filing (10%). Most denial causes are preventable with pre-submission scrubbing, real-time eligibility verification, and authorization tracking.
Should a small practice outsource revenue cycle management?
For most small practices, yes. Outsourcing removes salary, training, and software costs, eliminates single-point-of-failure risk, and delivers specialist-level billing performance. The 4 to 9% fee is typically offset by improved collections within the first quarter. Qualigenix clients average a 30% reduction in AR days after outsourcing.
How is RCM different in a hospital vs. a physician practice?
Hospital RCM involves DRG-based inpatient coding, APC-based outpatient coding, dual facility and professional billing, and large-scale payer contract management. Physician practice RCM focuses on professional billing — CMS-1500 claims, specialty-specific CPT coding, and smaller team workflows. Both require systematic denial management and AR follow-up to perform well.
What is the difference between front-end and back-end RCM?
Front-end RCM covers pre-encounter activities — registration, eligibility verification, prior authorization, and co-pay collection. Back-end RCM covers post-encounter activities — coding, claim submission, payment posting, denial management, and AR follow-up. Front-end errors cause most back-end denials. Prevention always costs less than correction.
How long does it take to see results after improving RCM?
Clean claim rate improvements are typically visible within the first billing cycle — 30 days. AR reductions become measurable within 60 to 90 days as aging claims are worked down and new claims flow through a cleaner process. Qualigenix clients regularly report a 30% reduction in AR days within the first quarter after onboarding.
How does Qualigenix help with revenue cycle management?
Qualigenix provides end-to-end RCM across 38+ specialties — eligibility verification, specialty coding, clean claim submission, denial management, AR follow-up, and payment posting. Clients achieve a 99% claim accuracy rate, 95% first-pass acceptance, 30% reduction in AR days, and a 36-day average collection cycle. Onboarding takes as few as 6 days.
Related Resources
Qualigenix Service Pages:
- Revenue Cycle Management Services
- Medical Billing Outsourcing Services
- Denial Management Services
- AR Follow-Up Services
- Medical Coding Services
- Insurance Eligibility Verification
- Claim Submission Services
Related Blog Guides:
- Revenue Cycle Management Best Practices
- Medical Billing Outsourcing vs. In-House
- Denial Management Process: Essential Steps
- What Is a Clean Claim Rate? Benchmarks and Best Practices
- Accounts Receivable in Medical Billing: Complete Guide
- The Healthcare Billing Process Explained
- Outsourcing Revenue Cycle Management: How It Works
Your Revenue Cycle Should Work as Hard as You Do
Qualigenix takes over the entire billing operation — eligibility, coding, claim submission, denial management, and AR follow-up — so your team can focus on patient care, not paperwork.
Our clients achieve 99% claim accuracy, a 95% first-pass acceptance rate, a 30% reduction in AR days, and an average 36-day collection cycle. We onboard in as few as 6 days.
Precision. Progress. Qualigenix.
What’s Next
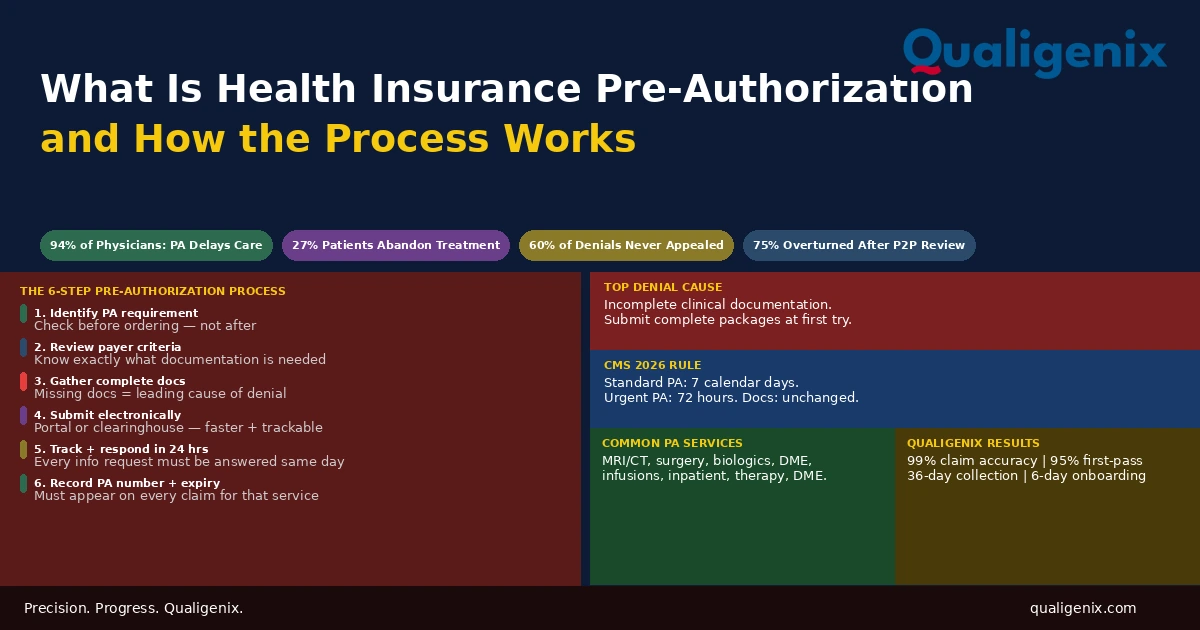
What Is Health Insurance Pre-Authorization and How It Works
Health insurance pre-authorization is the approval step that sits between a physician’s clinical decision and a patient’s access to...
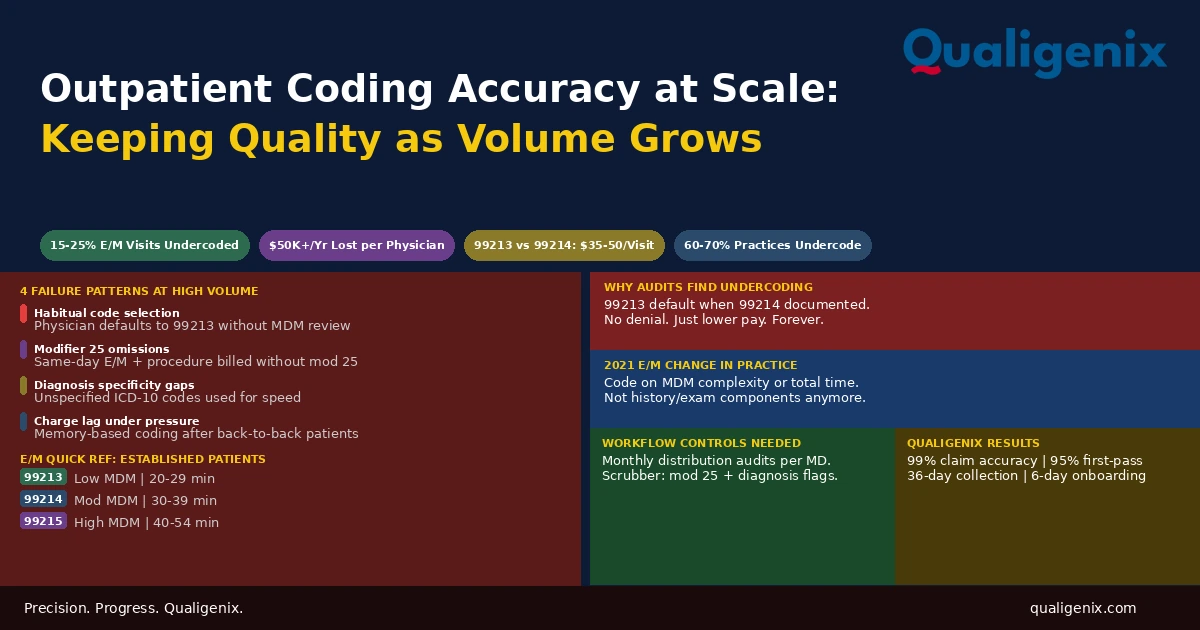
Outpatient Coding for High-Volume Practices: Keeping Accuracy at Scale
Outpatient coding accuracy is manageable when a physician sees 10 patients a day. It degrades predictably when they see...
Medicare Physician Fee Schedule 2026: What Every Practice Must Know
The 2026 Medicare Physician Fee Schedule (CMS-1832-F) introduces two separate conversion factors for the first time: $33.57 for qualifying...