DME for Medicare: Complete 2026 Billing & Compliance Guide
The Qualigenix Editorial Team consists of certified billing and coding experts with over 40 years of experience across 38+ medical specialties. Our content is rigorously researched against CMS, AMA, and payer-specific guidelines to ensure total compliance and accuracy. We apply the same elite standards to our resources as we do our client work, consistently delivering high claim accuracy and significant reductions in AR days.
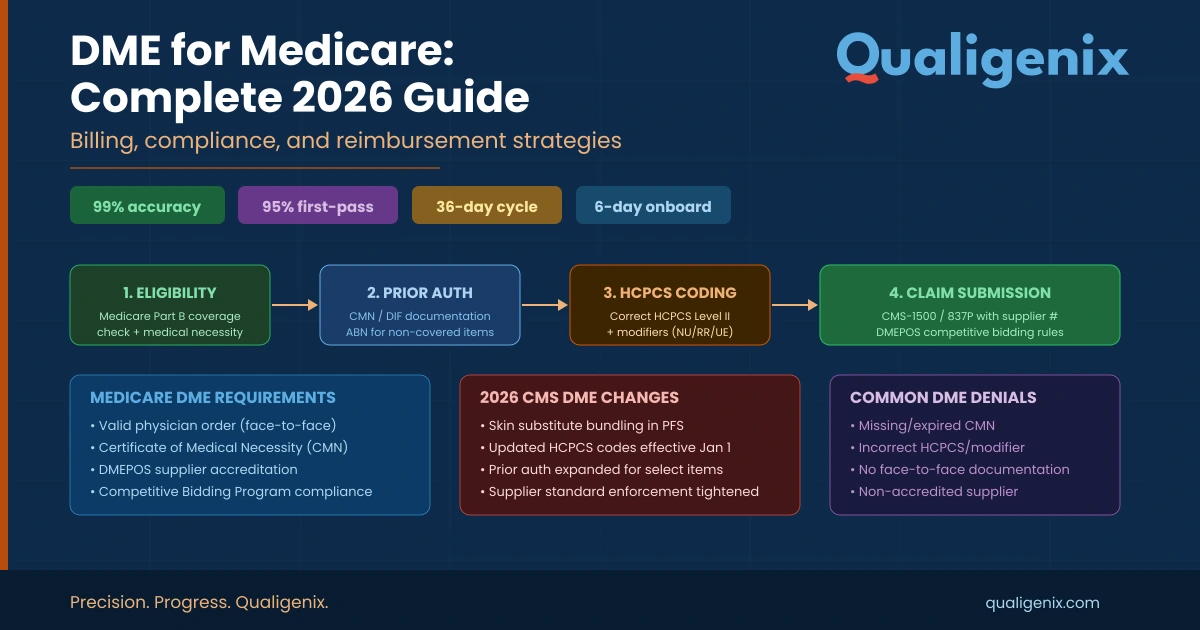
| Summary DME for Medicare refers to Durable Medical Equipment billed under Medicare Part B, using HCPCS Level II codes submitted to DME Medicare Administrative Contractors (MACs). In 2026, two major compliance changes affect all DME suppliers and referring providers: the April 13, 2026 Required List expansion adding 83 new HCPCS codes requiring Face-to-Face (F2F) documentation and a Written Order Prior to Delivery (WOPD), and 7 new Prior Authorization codes including orthoses and pneumatic compression devices. Practices that fail to update intake workflows before April 13, 2026 face a 30-60 day cash flow gap from denied claims. |
What Is DME for Medicare and Why Does Billing Get So Complex?
| DME for Medicare refers to Durable Medical Equipment, Prosthetics, Orthotics, and Supplies (DMEPOS) covered under Medicare Part B for beneficiaries who meet medical necessity criteria. DME must be prescribed by a Medicare-enrolled treating practitioner, ordered with a compliant Standard Written Order (SWO), and billed using HCPCS Level II codes to the appropriate DME Medicare Administrative Contractor (MAC) for the beneficiary’s home state. Medicare covers 80% of the approved amount after the Part B deductible is met, with the beneficiary responsible for the remaining 20%. |
Durable Medical Equipment covers an enormous range of products that help patients manage long-term health conditions at home — from CPAP machines and oxygen concentrators to wheelchairs, orthotic braces, insulin pumps, and nebulizers. Medicare alone spends over $6 billion annually on DMEPOS claims, according to CMS data. That scale, combined with historically high rates of fraud and improper billing, has made DME for Medicare one of the most heavily audited provider categories in the entire fee-for-service system.
Unlike most medical specialties that use CPT codes for billing, DME for Medicare relies primarily on HCPCS Level II codes — alphanumeric codes developed by CMS to describe specific equipment items, supplies, and services not covered by CPT. Getting these codes right, paired with correct modifiers, complete clinical documentation, and a valid Standard Written Order in the supplier’s possession before delivery, is the baseline requirement for any clean claim.
In 2026, the compliance stakes have gone up significantly. CMS published CMS-6097-N in the January 13, 2026 Federal Register, expanding the DMEPOS Required List by 83 items effective April 13, 2026. A separate prior authorization expansion added 7 new HCPCS codes requiring pre-approval before claims can be submitted. If your practice refers patients for DME or your organization supplies DME to Medicare beneficiaries, this guide covers everything you need to protect your revenue and stay compliant.
2026 DME for Medicare — Key Stats at a Glance
| Metric | Value / Detail |
| Annual Medicare DMEPOS Spend | Over $6 billion (CMS) |
| Required List Expansion (Effective April 13, 2026) | +83 new HCPCS codes requiring F2F + WOPD |
| Prior Authorization List Expansion (Effective April 13, 2026) | +7 new HCPCS codes (5 orthoses + 2 pneumatic compression) |
| Current DMEPOS Master List Size | 512+ items |
| Required Prior Authorization List (Pre-2026) | 67 items |
| F2F Encounter Window | Within 6 months before order date |
| Cash Flow Gap if Workflow Not Updated by April 13 | 30-60 days (denied claims) |
| Qualigenix Claim Accuracy Rate | 99% |
| Qualigenix First-Pass Acceptance Rate | 95% |
| Qualigenix AR Days Reduction | 30% |
| Qualigenix Average Onboarding | 6 days |
| Medicare Part B DME Patient Responsibility | 20% after deductible |
How Does Medicare Part B Cover DME?
Medicare Part B is the coverage vehicle for DME for Medicare. To qualify for coverage, the equipment must meet four criteria established by CMS: it must be durable (withstand repeated use), primarily serve a medical purpose, not be useful to a person in the absence of illness or injury, and be appropriate for use in the home. Meeting these criteria is necessary but not sufficient — the equipment must also meet medical necessity documentation standards and be ordered by a Medicare-enrolled treating practitioner.
Coverage rules follow the beneficiary’s home state, not the location of the ordering practice. DME claims are submitted to the DME MAC assigned to that beneficiary’s state. The four DME MACs — Noridian, CGS Administrators, National Government Services (NGS), and Palmetto GBA — each handle a specific geographic jurisdiction. Submitting a claim to the wrong MAC is a common and entirely preventable denial cause.
Medicare covers the item at 80% of the approved DMEPOS fee schedule amount, with the beneficiary responsible for the remaining 20% after the Part B annual deductible is satisfied. For equipment classified under ‘capped rental’ rules — including hospital beds, CPAP devices, and certain mobility equipment — billing follows a structured rental-to-purchase pathway with specific anniversary date tracking requirements.
What Makes DME ‘Durable’ Under Medicare Rules?
Medicare defines durability as the ability to withstand repeated use for a significant period. Single-use items, disposable supplies, and equipment with a lifespan under 3 years typically do not qualify as DME for Medicare Part B coverage. Supplies used with qualifying DME — such as A4253 blood glucose test strips or A4239 insulin infusion supplies — may be separately billable as DMEPOS supplies, but follow distinct coverage and quantity limitation rules.
What Is a Standard Written Order (SWO) and Why Is It Critical?
A Standard Written Order is the document that authorizes a DME supplier to provide an item to a Medicare beneficiary. Under CMS rules, the SWO must be in the supplier’s possession before the item is delivered — not after. For items on the Required List, the SWO must also be accompanied by a compliant Face-to-Face encounter note from within the previous 6 months.
The SWO must include: the beneficiary’s name or Medicare Beneficiary Identifier (MBI), a description of the item ordered, the treating practitioner’s name and NPI, date of the order, and the treating practitioner’s signature. Missing or incomplete SWOs are the single most common reason for DMEPOS claim denials, according to CMS CERT data.
The April 13, 2026 Required List Expansion: What Every Practice Must Know
This is the most significant DME compliance change of 2026 and the one posing the greatest cash flow risk to practices and suppliers who are not prepared. CMS published CMS-6097-N in the Federal Register on January 13, 2026, massively expanding the DMEPOS Required List — the subset of the Master List where F2F documentation and WOPD requirements are actively enforced as conditions of payment.
Eighty-three new HCPCS codes are being added to the Required List, effective April 13, 2026. For any claim with a date of service on or after that date for an item on this expanded list, Medicare will deny the claim outright if it lacks a compliant WOPD or a Face-to-Face encounter note from within the preceding 6 months. There is no grace period. The OIG and CERT program’s Comprehensive Error Rate Testing consistently identified these high-cost and high-volume categories as having elevated rates of improper payments — which is precisely why CMS is adding enforcement.
The expansion heavily targets orthotics (both off-the-shelf and custom-fabricated), mobility assistive equipment accessories, and new respiratory equipment categories including nebulizers and oxygen supplies. Custom-fabricated orthoses face heightened scrutiny, with additional documentation required to justify why a custom device was medically necessary versus a prefabricated alternative.
The 7 New Prior Authorization Codes (Also Effective April 13, 2026)
Separately from the Required List expansion, CMS is adding 7 new HCPCS codes to the Required Prior Authorization List. Prior authorization requests for these codes can be submitted to the applicable DME MAC beginning March 30, 2026 — two weeks before the effective date. The 7 new PA codes are:
- L0651, L1844, L1846, L1852, L1932: Five orthotic codes covering spinal, knee, and ankle-foot orthoses
- E0651, E0652: Two pneumatic compression device codes
For suppliers with pending brace orders for delivery on or after April 13, immediate review is required. Any order involving these codes must have a P/A request in progress before the effective date to prevent cash flow disruption.
Master List vs. Required List vs. Prior Authorization List: What Is the Difference?
| List Type | What It Is | Practical Effect | 2026 Update |
| DMEPOS Master List | All items under review by CMS for potential additional requirements | No automatic PA or documentation mandate; items may be elevated to Required List | 18 new HCPCS codes added (Jan 13, 2026) |
| Required List (F2F + WOPD) | Items requiring Face-to-Face exam within 6 months AND Written Order Prior to Delivery as conditions of payment | Claims denied without compliant F2F note + valid SWO in supplier’s possession before delivery | 83 new items added, effective April 13, 2026 |
| Required Prior Authorization List | Items requiring pre-approval from DME MAC before claim submission | Non-affirmation = claim denial. Must submit P/A request before furnishing item | 7 new codes added, effective April 13, 2026 |
HCPCS Codes for DME for Medicare: A Billing Reference
HCPCS Level II codes are the backbone of DME for Medicare billing. Unlike CPT codes, they describe the physical item delivered — not the service performed. The most commonly billed categories and representative codes include:
Respiratory Equipment
- E0601: CPAP device — requires sleep study confirming obstructive sleep apnea; modifiers NU (new) or RR (rental) required
- E1390: Oxygen concentrator, single delivery port — requires documented hypoxemia (O2 sat at or below 88%); KX modifier mandatory for Medicare
- E0431: Portable gaseous oxygen — documentation must show oxygen use beyond the home
Diabetes Equipment
- E0784: External insulin pump — often requires prior authorization; documentation must show uncontrolled diabetes despite multiple daily injections
- A4253: Blood glucose test strips — coverage limits vary by insulin use frequency; Medicare limits typically apply
- E0607: Home blood glucose monitor — covered when prescribed with clear documentation
Mobility Equipment
- E0143: Walker, folding — requires documentation of mobility impairment and physician certification
- K0001: Standard manual wheelchair — requires physician certification of medical necessity; mobility assessment often required
- K0005: Ultra-lightweight manual wheelchair — stricter medical necessity documentation; typically requires face-to-face assessment
Key Modifiers for DME Billing
- KX: Documentation is on file and meets LCD criteria — required for many Medicare DME items
- NU: New equipment — used when beneficiary is purchasing the item
- RR: Rental — used for monthly rental billing
- GA: Waiver of liability on file — used when supplier expects Medicare may deny
What Are the Top DME for Medicare Claim Denial Causes in 2026?
Understanding why DME claims get denied is as important as knowing the billing rules themselves. The 2026 CMS audit environment is more technology-driven and comprehensive than any prior year. Here are the top denial triggers your team must prevent:
- Missing or non-compliant SWO: If the Standard Written Order is incomplete, missing key patient or prescriber information, or not in the supplier’s possession before delivery, Medicare will reject the claim outright. For complex equipment like power mobility devices and ventilators, pre-delivery SWOs are strictly required.
- Incomplete medical necessity documentation: Medicare requires clear clinical evidence supporting the need for the equipment. Missing functional assessments, diagnosis codes, or supporting clinical notes are a leading cause of denials. Documentation must explicitly state why the item is medically necessary for this specific patient.
- Invalid or outdated HCPCS codes: Using obsolete or incorrect HCPCS codes is one of the most common reasons Medicare denies DME claims. With 83 new Required List codes and 18 new Master List codes effective in 2026, billing teams must ensure their code libraries are updated immediately.
- Missing F2F note for Required List items: For the 83 expanded Required List items effective April 13, 2026, any claim without a compliant Face-to-Face encounter note from within 6 months of the order date will be automatically denied.
- Wrong DME MAC jurisdiction: Claims submitted to the wrong MAC for the beneficiary’s home state will be rejected. Confirm MAC jurisdiction before every submission.
- Incorrect modifier usage: Missing the KX modifier when documentation supports coverage, or using the wrong rental vs. purchase modifier, are common avoidable denials.
- Capped rental billing errors: Items on the capped rental schedule have strict billing frequency rules and anniversary tracking requirements. Missing anniversary dates or billing after the rental-to-purchase conversion point creates overpayment liability.
How to Prepare Your Practice for the April 13, 2026 Required List Expansion
Waiting until April 13 to update your workflows is not an option. Practices that do will face a 30-60 day cash flow gap while denied claims are corrected and resubmitted. Here is the action plan your team needs now:
- Access CMS-6097-N: Download the Federal Register notice and identify which HCPCS codes in your order mix are moving to the Required List.
- Update your EMR alerts: Flag all Required List codes in your electronic medical records system so that any order for these items automatically triggers a documentation checklist.
- Verify F2F documentation protocols: Confirm that clinical notes for qualifying patients document the in-person exam, the clinical findings, and why the specific DME item is medically necessary. NPs, CNSs, and PAs can perform qualifying F2F encounters within their scope of practice.
- Audit SWO templates: Ensure all SWO templates include every required field — MBI or beneficiary name, item description, prescriber name and NPI, order date, and signature.
- Identify custom fabricated orthosis orders: For L1844 and L1846 codes, prepare documentation explaining why a custom device is necessary versus a prefabricated alternative.
- Submit P/A requests for new PA codes: Requests for the 7 new prior authorization codes (L0651, L1844, L1846, L1852, L1932, E0651, E0652) can be submitted starting March 30, 2026.
- Train all intake and billing staff: Front desk, clinical, and billing teams all have a role in DME compliance. One gap in the chain creates a denied claim.
How Qualigenix Protects Your DME for Medicare Revenue
DME for Medicare billing is among the most documentation-intensive and audit-exposed categories in healthcare revenue cycle management. Qualigenix provides specialized DME billing support that covers every layer of the claim lifecycle — from intake documentation audit to MAC submission to denial appeal.
Our 99% claim accuracy rate is the result of systematic pre-billing audits that verify SWOs, HCPCS codes, modifier selection, and clinical documentation before a single claim leaves your practice. When CMS expanded the Required List in January 2026, our team immediately updated our code databases and client intake workflows — so April 13 is not a disruption for our clients. It was already handled.
DME Billing Services: Specialized HCPCS coding, modifier application, and MAC-specific submission management. Visit qualigenix.com/specialities/dme-billing-services/
Prior Authorization Solutions: Our PA team manages prior authorization workflows for both legacy and newly required DMEPOS codes, including the 7 new April 2026 additions. Visit qualigenix.com/services/revenue-cycle-management-services/prior-authorization-solutions/
Denial Management Services: When DME claims are denied — for SWO issues, F2F documentation gaps, or MAC errors — our denial team resolves them fast. Visit qualigenix.com/services/revenue-cycle-management-services/denial-management-services/
Medical Coding Services: HCPCS code accuracy validated against 2026 CMS updates. Visit qualigenix.com/services/revenue-cycle-management-services/medical-coding-services/
Charge Entry Services: Clean charge entry that pairs correct HCPCS codes with compliant modifiers for every DME claim. Visit qualigenix.com/services/revenue-cycle-management-services/charge-entry-services
Frequently Asked Questions: DME for Medicare
What qualifies as DME for Medicare coverage?
To qualify as DME for Medicare, equipment must be durable (withstand repeated use), primarily serve a medical purpose, be of no use to a healthy person, and be appropriate for home use. Common qualifying items include hospital beds, wheelchairs, CPAP and BiPAP devices, oxygen equipment, walkers, and insulin pumps. The ordering practitioner must establish and document medical necessity for the specific item ordered.
How is DME billed to Medicare?
DME for Medicare is billed using HCPCS Level II codes, submitted electronically via EDI to the DME MAC serving the beneficiary’s home state. Claims must include the appropriate HCPCS code, required modifiers (KX, NU, RR, etc.), the treating provider’s NPI, and diagnosis codes that support medical necessity. The supplier must have a valid, complete SWO in their possession before submitting the claim.
What is the April 13, 2026 Required List expansion?
CMS published CMS-6097-N on January 13, 2026, expanding the DMEPOS Required List by 83 new HCPCS codes, effective April 13, 2026. For any claim with a service date on or after April 13 for these items, Medicare requires a Face-to-Face encounter note from within 6 months of the order date AND a Written Order Prior to Delivery (WOPD) as conditions of payment. Missing either results in automatic claim denial.
Can a nurse practitioner conduct the Face-to-Face encounter for DME?
Yes. A Nurse Practitioner (NP), Clinical Nurse Specialist (CNS), or Physician Assistant (PA) can perform the qualifying Face-to-Face encounter, provided they are treating the beneficiary for the condition requiring the DME item and the encounter is within their scope of practice. HCPCS code G0454 can be used by these practitioners to bill for required F2F DME encounters under Medicare rules.
What are the most common HCPCS code mistakes in DME billing?
The most common HCPCS errors include using codes that have been revised or deleted in the annual January update without checking the current CMS code set, applying the wrong modifier (e.g., NU vs. RR for purchase vs. rental), missing the KX modifier when documentation supports coverage, and using a general code when a more specific code is required. CMS’s PDAC (Pricing, Data Analysis and Coding) contractor is the authoritative resource for HCPCS code classification — their helpline is 877-735-1326.
What is capped rental for DME under Medicare?
Capped rental means Medicare pays a monthly rental fee for certain DME items for up to 13 months. After the rental period, ownership transfers to the beneficiary and Medicare pays for ongoing maintenance and servicing. Items subject to capped rental include hospital beds, CPAP devices, and certain mobility aids. Billing after the rental-to-purchase conversion creates overpayment exposure, and tracking anniversary dates is critical for clean claim compliance.
How does outsourcing DME billing to Qualigenix help practices?
Qualigenix handles the full DMEPOS billing cycle: SWO compliance review, HCPCS code validation, modifier selection, MAC jurisdiction confirmation, claim submission, and denial management. Our 95% first-pass acceptance rate for DME claims reflects systematic pre-billing audits that catch documentation gaps before submission. With the April 2026 Required List expansion, practices that partner with Qualigenix have already had their intake workflows updated — no cash flow disruption, no scramble.
Related Qualigenix Resources
Protect your DME and specialty billing revenue with these Qualigenix service pages and guides:
- DME Billing Services
- Prior Authorization Solutions
- Denial Management Services
- Medical Coding Services
- Charge Entry Services
- Claim Submission Services
- Insurance Eligibility Verification Services
- What is DME Revenue Cycle Management?
- Prior Authorization in Healthcare
- How to Reduce Medical Claim Denials
| Don’t Let the April 2026 DME Changes Cost You Revenue Eighty-three new HCPCS codes are joining the Required List on April 13, 2026. Practices that do not update their intake documentation workflows now will face denied claims, delayed payments, and a 30-60 day cash flow gap. Qualigenix has already updated our client systems. Your practice can be next. Book a Free Consultation today at qualigenix.com/contact-us/ |
What’s Next

Denial Management in 2026: The Top 10 Codes and the Appeal Playbook for Each
Denials cluster around a small set of codes, and each one has a different correct response. Some need a...
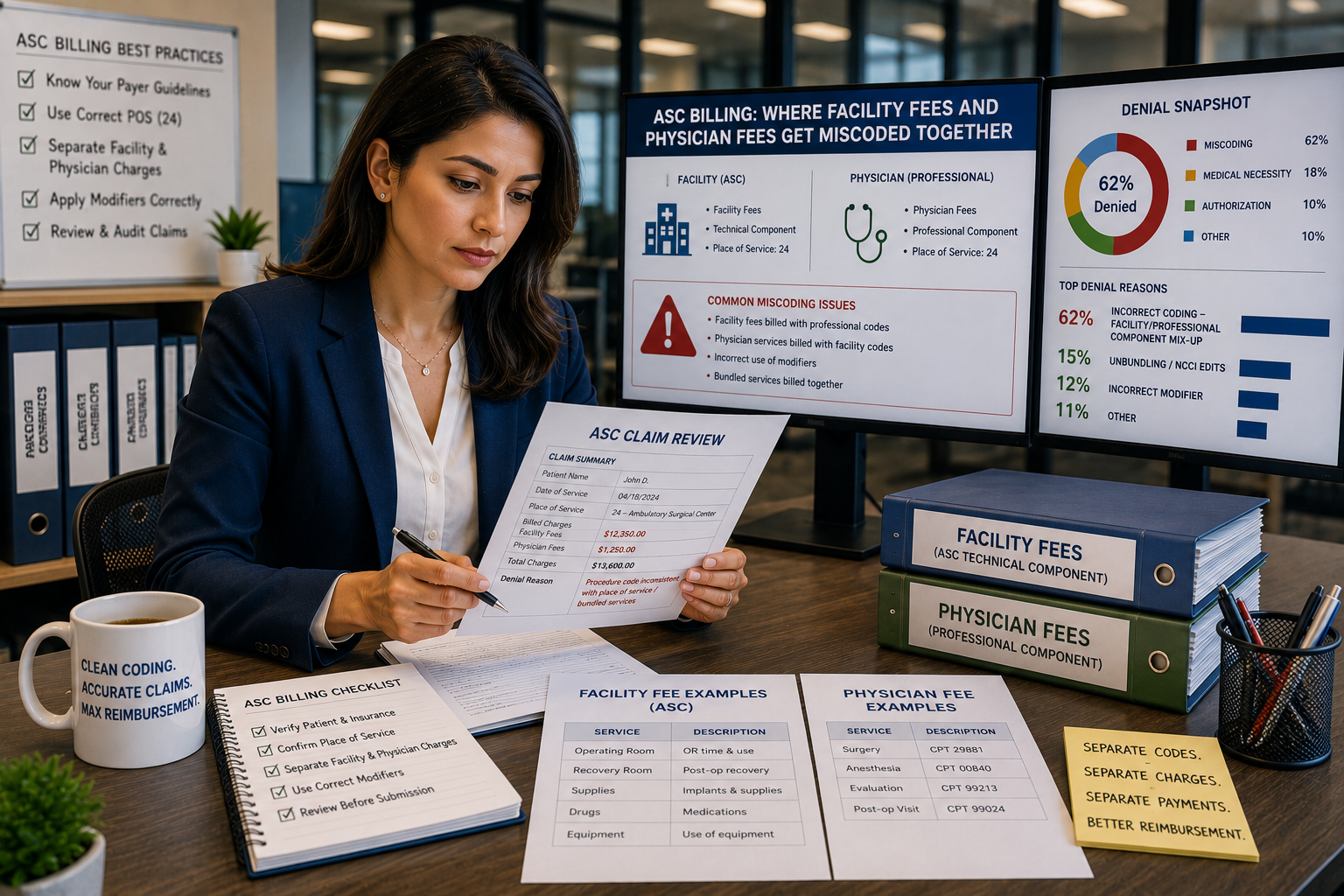
ASC Billing: Where Facility Fees and Physician Fees Get Miscoded Together
ASC facility and physician claims both go out on a CMS-1500 form with the same CPT code and place...
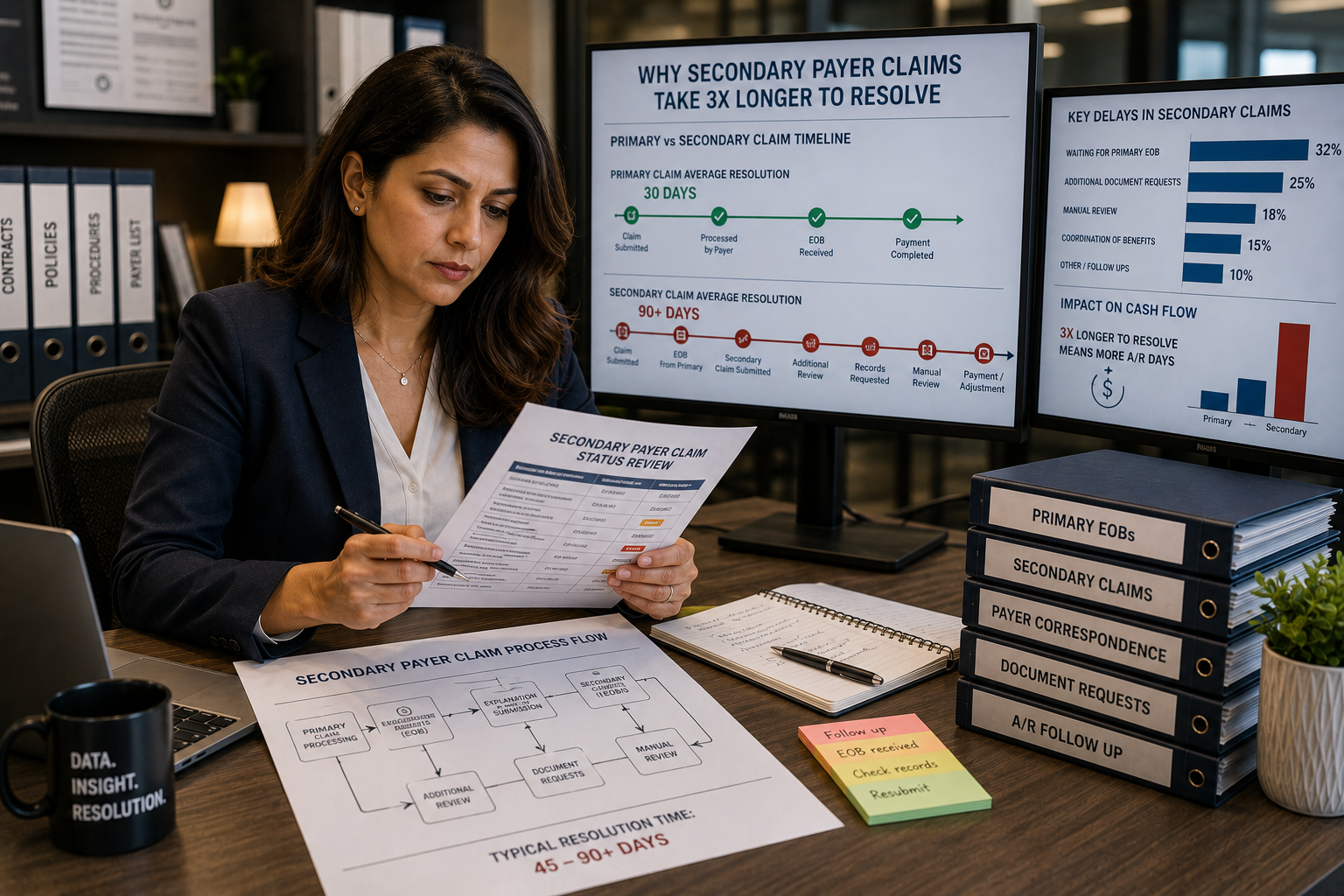
Coordination of benefits errors: why secondary payer claims take 3x longer to resolve
Secondary payer claims stall because coordination of benefits errors, wrong payer order, outdated COB records, and missing primary...