What Is an EOB in Medical Billing? How to Read, Post, and Use Explanation of Benefits Statements
The Qualigenix Editorial Team consists of certified billing and coding experts with over 40 years of experience across 38+ medical specialties. Our content is rigorously researched against CMS, AMA, and payer-specific guidelines to ensure total compliance and accuracy. We apply the same elite standards to our resources as we do our client work, consistently delivering high claim accuracy and significant reductions in AR days.

An EOB (Explanation of Benefits) is a document sent by an insurance payer after processing a medical claim. It details what services were billed, what the payer covered, what adjustments were made, and what the patient owes. An EOB is not a bill—it’s a claim processing summary that billing teams use for payment posting, denial identification, appeal documentation, and patient billing. Understanding how to read and act on EOBs is fundamental to revenue cycle accuracy. This guide covers every section of an EOB, how it differs from an ERA and a medical bill, the most common EOB issues, and how Qualigenix’s payment posting and denial management services turn EOBs into clean, accurate AR.
If you work in medical billing, you encounter EOBs every day. But if you’re new to the field-or if you’ve ever wondered what is an EOB in medical billing and why it matters to your revenue cycle-this guide will give you the complete picture.
An Explanation of Benefits is one of the most important documents in healthcare billing. It’s the payer’s official response to every claim you submit, and it contains the information your team needs to post payments correctly, identify denials, bill patients accurately, and initiate appeals when warranted. Yet many billing teams treat EOBs as routine paperwork instead of the revenue intelligence they actually are.
Misreading an EOB leads to misposted payments. Ignoring EOB adjustment codes means leaving recoverable revenue on the table. Failing to reconcile EOBs with patient statements creates billing disputes and erodes patient trust. This guide walks through every section of an EOB, how to read each field, the critical difference between an EOB and an ERA, and how Qualigenix’s payment posting services and denial management services ensure every EOB is processed accurately.
What Is an EOB in Medical Billing?
| Direct Answer: An EOB (Explanation of Benefits) is a statement issued by an insurance payer after a medical claim is processed. It summarizes the services billed, the amount the payer allowed and paid, any adjustments or denials with reason codes, and the patient’s remaining financial responsibility (deductible, copay, coinsurance). An EOB is not a bill-it is a claim adjudication summary sent to both the provider and the patient under federal notification requirements. |
Think of an EOB as the “report card” for every claim your practice submits. It tells you whether the payer accepted the claim, how much they paid, why they adjusted or denied specific line items, and what the patient owes. For billing teams, EOBs are the primary source document for payment posting, denial follow-up, and patient statement generation.
Federal regulations require insurers to send EOBs to patients for every processed claim, ensuring transparency in how benefits are applied. Providers receive the same information-typically in electronic format as an ERA 835-to enable efficient payment reconciliation.
EOB in Medical Billing: Key Stats at a Glance
| Metric | Value / Source |
| Claims denied on first submission (industry avg.) | 11.8% (industry data 2025) |
| Medicare Advantage first-submission denial rate | ~18% (CMS data) |
| Missing/inaccurate data as top denial cause | 50% of denials (Experian Health 2025) |
| Authorization issues causing denials | 35% (Experian Health 2025) |
| Active CARC codes used on EOBs/ERAs | 358 (ANSI X12) |
| Active RARC codes for supplemental detail | 1,185 (ANSI X12) |
| Claim adjustment group codes on EOBs | 5 (CO, PR, OA, PI, CR) |
| Federal requirement for EOB issuance | HIPAA / ACA Section 2715 |
| ERA 835 electronic format standard | ANSI X12 835 (HIPAA-mandated) |
What Information Does an EOB Contain?
While formatting varies by payer, every Explanation of Benefits includes the same core data fields. Understanding each section is the foundation of accurate payment posting.
Patient and subscriber information: Patient name, member/subscriber ID, group number, and plan information. Always verify this matches your records before posting.
Provider information: Billing provider, rendering provider, and facility name. Confirm the claim was attributed to the correct provider in your system.
Service details: Date(s) of service, CPT/HCPCS procedure codes, ICD-10 diagnosis codes, modifiers, units, and place of service. These should match exactly what was submitted on the claim.
Billed charges: The total amount your practice charged for each service line. This is your starting point before adjustments.
Allowed amount: The maximum the payer will consider for reimbursement based on the contracted fee schedule or Medicare rate. The difference between billed charges and allowed amount is typically a contractual adjustment (CO-45).
Payer payment: The dollar amount the insurance company actually paid to the provider. This should match the deposit on your bank statement or remittance.
Adjustment codes (CARC + RARC): Claim Adjustment Reason Codes and Remittance Advice Remark Codes explain why the payer adjusted or denied each line item. These codes—paired with group codes CO, PR, OA, PI, or CR—tell you who is financially responsible for each adjustment. See our claim adjustment guide for detailed code breakdowns.
Patient responsibility: The amount the patient owes, broken down by deductible (PR-1), coinsurance (PR-2), and copay (PR-3). This amount gets posted to the patient’s balance and drives patient statement generation.
Denial reasons: If any service line was denied, the EOB shows the specific CARC and RARC codes explaining why. Denials flagged here are your team’s trigger to correct and resubmit or initiate an appeal.
What Is the Difference Between an EOB, ERA, and Medical Bill?
These three documents are frequently confused. They serve different purposes and go to different recipients:
| Factor | EOB (Explanation of Benefits) | ERA (Electronic Remittance Advice) | Medical Bill / Patient Statement |
| What it is | Paper/digital claim processing summary | Electronic data file (ANSI X12 835) | Invoice sent to the patient |
| Who receives it | Patient AND provider | Provider only (via clearinghouse) | Patient only |
| Format | Human-readable summary | Machine-readable for auto- posting | Patient-friendly with amount due |
| Purpose | Transparency on claim outcome | Automated payment posting into PM/EHR | Collects patient’s financial responsibility |
| Contains CARC/RARC | Yes (in text/code format) | Yes (structured data fields) | No (shows balance due only) |
| Is it a bill? | No | No | Yes |
| HIPAA mandate | Required for patient notification | Required for electronic transactions | Not HIPAA-mandated (billing practice) |
For billing teams, the ERA 835 is the workhorse—it feeds directly into your practice management system for auto-posting. The EOB is the human-readable version used for audits, appeals, and patient communication. The medical bill is the final step: it tells the patient what they owe based on what the EOB/ERA determined.
How Do You Read an Explanation of Benefits Statement Step by Step?
Here’s the systematic approach Qualigenix billing teams follow when processing every EOB:
Step 1 — Verify patient and claim identity: Match the patient name, member ID, claim number, and dates of service to your billing system. Confirm you’re posting to the correct account and the correct payer sequence (primary vs. secondary).
Step 2 — Check billed charges against submitted claim: Ensure the CPT/HCPCS codes, modifiers, units, and place of service on the EOB match what you originally submitted. Discrepancies here indicate a claim was altered during processing.
Step 3 — Review the allowed amount: Compare the payer’s allowed amount to your contracted rate. If the allowed amount is lower than expected, it may indicate a fee schedule error, a bundling adjustment, or an out-of-network reduction. CO-45 is the standard contractual adjustment code.
Step 4 — Read group codes before CARC codes: The group code (CO, PR, OA, PI, CR) determines financial responsibility before you even look at the reason. CO = provider write-off. PR = patient balance. OA/PI = review for appeal potential. CR = reverse and repost.
Step 5 — Read CARC + RARC as a pair: The CARC tells you the category of adjustment. The RARC tells you the specific detail. For broad codes like CO-16, the RARC is where the actionable fix lives.
Step 6 — Identify denials and classify as valid or recoverable: Valid adjustments (CO-45 matching your contract) get posted as write-offs. Recoverable denials (CO-16, CO-4, CO-22) get corrected and resubmitted within the payer’s filing deadline.
Step 7 — Post accurately and reconcile: Post payer payment to insurance line. Post CO adjustments to contractual bucket. Post PR amounts to patient balance. Finalize only after all payer sequences have processed. Our payment posting services handle this with group-code-level precision.
Is an EOB the Same as a Medical Bill?
No. An EOB is a claim processing summary sent by the insurance company to explain how a claim was adjudicated. It shows what the payer covered, what was adjusted, and what the patient may owe—but it is not a request for payment. The medical bill is a separate invoice sent by the provider to the patient for the amount identified as patient responsibility on the EOB.
What Are the Most Common EOB Issues That Affect Revenue?
These are the EOB-related problems Qualigenix identifies most frequently across practices:
1. Misposted Adjustments
Posting a CO adjustment to the patient balance: This bills the patient for an amount they don’t owe, violating your payer contract. It’s one of the most common payment posting errors and creates patient complaints, refund requests, and compliance risk. Always post CO to contractual write-off—never to patient AR.
2. Ignoring Actionable Denial Codes
Treating every denial as a write-off: When billing teams see a denied line item on the EOB and write it off without reviewing the CARC/RARC codes, they’re leaving recoverable revenue on the table. CO-16 (missing information), CO-4 (modifier error), and CO-22 (wrong payer) are all correctable—if your team acts within the filing window.
3. Failing to Reconcile EOB with Bank Deposit
Posting the EOB amount without matching the actual deposit: The payment shown on the EOB should match the bank deposit or EFT. If it doesn’t, there may be a recoupment, offset, or payment split your team missed. Always reconcile EOB payment amounts with actual deposits before closing the posting.
4. Not Using EOBs for Secondary Billing
Billing the secondary payer without the primary EOB attached: Secondary payers require the primary payer’s EOB to calculate their payment. Submitting a secondary claim without it triggers a denial or a Secondary Claim Development Questionnaire that delays payment by weeks. This is especially common in Medicare secondary payer situations.
5. Delayed Patient Statement Generation
Waiting too long to bill the patient after receiving the EOB: Once the EOB identifies patient responsibility, promptly generate and send the patient statement. Delays reduce collection rates—patients are most likely to pay within the first 30 days of receiving a bill. Qualigenix’s patient statement services automate this process.
How Long Should You Keep EOBs on File?
Retain EOBs for a minimum of 6–7 years, consistent with federal and state medical record retention requirements and payer audit timelines. Medicare requires providers to maintain billing records for at least 7 years. For patients with chronic conditions or ongoing treatment, longer retention is advisable. Store both paper and electronic copies in a secure, HIPAA-compliant system.
Can Patients Use EOBs to Dispute a Medical Bill?
Yes. Patients can compare their EOB with the provider’s bill to verify that the charged amount matches the patient responsibility shown on the EOB. If the bill is higher than the EOB’s “you may owe” amount, it may indicate a billing error, a prior balance carryover, or charges from a different date of service. The EOB is the patient’s primary tool for catching billing discrepancies.
How Does Qualigenix Ensure Accurate EOB Processing and Payment Posting?
EOB processing is where billing accuracy lives or dies. A single misposted adjustment ripples through patient statements, AR reports, and financial reconciliation. That’s why practices across 38+ specialties partner with Qualigenix for precision payment posting.
Group-code-level posting accuracy: Every EOB is posted with strict adherence to group codes—CO to contractual write-off, PR to patient balance, OA/PI flagged for review. No CO dollars ever touch patient AR. Our payment posting services maintain this standard across every payer and every claim.
CARC/RARC-driven denial identification: Our team reads every adjustment code pair, classifies each as valid or recoverable, and routes actionable denials to our denial management services for correction and resubmission within payer deadlines.
ERA 835 auto-posting with manual review: We leverage electronic remittance auto-posting for efficiency but apply manual review checkpoints to catch discrepancies that auto-posting misses—fee schedule mismatches, unexpected bundling, and payer-initiated reductions.
EOB-to-deposit reconciliation: Every posted payment is matched against actual bank deposits before the posting is finalized. Discrepancies trigger immediate investigation.
99% claim accuracy and 95% first-pass rate: Accurate EOB processing is the downstream result of clean claims going in. Our 99% claim accuracy rate means fewer adjustments and denials on the EOB in the first place. Combined with a 36-day average collection cycle and 30% AR reduction, our clients see measurable revenue improvement.
EOB Processing Checklist for Billing Teams
Use this checklist to audit your current EOB workflow:
- Patient/claim verified: EOB matched to correct patient, claim ID, dates of service, and payer sequence before posting
- Billed charges confirmed: CPT/HCPCS codes, modifiers, and units on EOB match the original submitted claim
- Allowed amount checked: Payer’s allowed amount compared against contracted fee schedule; discrepancies flagged for review
- Group code read first: CO, PR, OA, PI, or CR identified before reading the CARC number on every line item
- CARC + RARC paired: Both codes read together to determine root cause and required action for each adjustment
- CO posted to contractual: All CO adjustments posted to contractual adjustment bucket—never to patient AR
- PR posted to patient balance: Deductible, copay, and coinsurance amounts posted to patient responsibility and statement generated
- Denials routed for action: Recoverable denials (CO-16, CO-4, CO-22, PI codes) sent to denial management for correction/resubmission
- Payment reconciled with deposit: EOB payment amount matched against actual bank deposit or EFT before posting is finalized
- Secondary claim prepared: Primary EOB attached when submitting to secondary payer; patient balance finalized only after all payers process
Frequently Asked Questions About EOBs in Medical Billing
What does EOB stand for in medical billing?
EOB stands for Explanation of Benefits. It is a document sent by an insurance payer after processing a medical claim. The EOB summarizes what was billed, what the payer covered, what adjustments were made (with CARC/RARC codes), and what the patient owes. It is not a bill—it is a claim adjudication summary.
What is the difference between an EOB and an ERA?
An EOB is a human-readable claim processing summary sent to both the provider and the patient. An ERA (Electronic Remittance Advice) is the machine-readable electronic version (ANSI X12 835 format) sent only to the provider via clearinghouse. ERAs enable automated payment posting; EOBs are used for audits, appeals, and patient communication. Both contain the same claim data.
Is an EOB the same as a medical bill?
No. An EOB explains how the payer processed a claim and what the patient may owe. A medical bill is a separate invoice sent by the provider to the patient requesting payment for the amount identified as patient responsibility on the EOB. Always compare the two—if they don’t match, contact the provider or insurer.
Why did I receive an EOB if I don’t owe anything?
Insurance companies are required to send EOBs for every processed claim, even when the payer covered the full cost. The EOB confirms that no patient balance exists and serves as your record that the service was processed. It’s a transparency requirement, not a payment request.
How do billing teams use EOBs for denial management?
Billing teams review the CARC and RARC codes on the EOB to identify why a claim was denied or adjusted. Actionable denials—such as CO-16 (missing information), CO-4 (modifier error), or CO-22 (wrong payer)—are corrected and resubmitted within the payer’s filing deadline. The EOB is also the primary documentation for formal appeals.
How long should you keep EOBs?
Retain EOBs for at least 6–7 years, consistent with federal and state retention requirements. Medicare providers should keep records for 7 years. EOBs are needed for audits, appeals, and retroactive claim reviews. Store securely in HIPAA-compliant systems.
What should I do if my EOB and my medical bill don’t match?
Compare the “you may owe” amount on the EOB with the bill from your provider. If the bill is higher, it may include a prior balance, charges from another date of service, or a billing error. Contact the provider’s billing department first, then your insurance company if the discrepancy isn’t resolved.
How does Qualigenix handle EOB processing?
Qualigenix posts every EOB with group-code-level precision—CO to contractual write-off, PR to patient balance, and actionable denials routed for correction. We reconcile payments against bank deposits, use ERA auto-posting with manual checkpoints, and track adjustment patterns to prevent recurring issues. Our 99% claim accuracy rate and 36-day collection cycle reflect this approach.
Related Qualigenix Resources
Service Pages:
- Payment Posting Services
- Denial Management Services
- Medical EDI Services
- Patient Statement Services
- AR Follow-Up Services
- Insurance Eligibility Verification Services
Blog Guides:
- Claim Adjustment in Medical Billing Guide
- How to Appeal an Insurance Claim Denial Step by Step
- Denial Management in Medical Billing: 7 Common Causes
- Healthcare Billing Process Explained
- What Is a Clean Claim Rate? Benchmarks & Best Practices
- Medicare Secondary Payer: Rules & Billing Guide
Stop Losing Revenue to EOB Processing Errors — Book a Free Consultation
Every misposted EOB, every ignored denial code, and every unreconciled payment is revenue your practice is losing. Whether your team struggles with CARC interpretation, payment posting accuracy, or patient statement timing, Qualigenix has the expertise and infrastructure to fix it.
Our team delivers 99% claim accuracy, a 95% first-pass acceptance rate, and an average 36-day collection cycle. We onboard in as few as 6 days, starting with a comprehensive AR assessment that identifies where EOB processing gaps are costing your practice.
What’s Next
Denial Management in 2026: The Top 10 Codes and the Appeal Playbook for Each
Denials cluster around a small set of codes, and each one has a different correct response. Some need a...
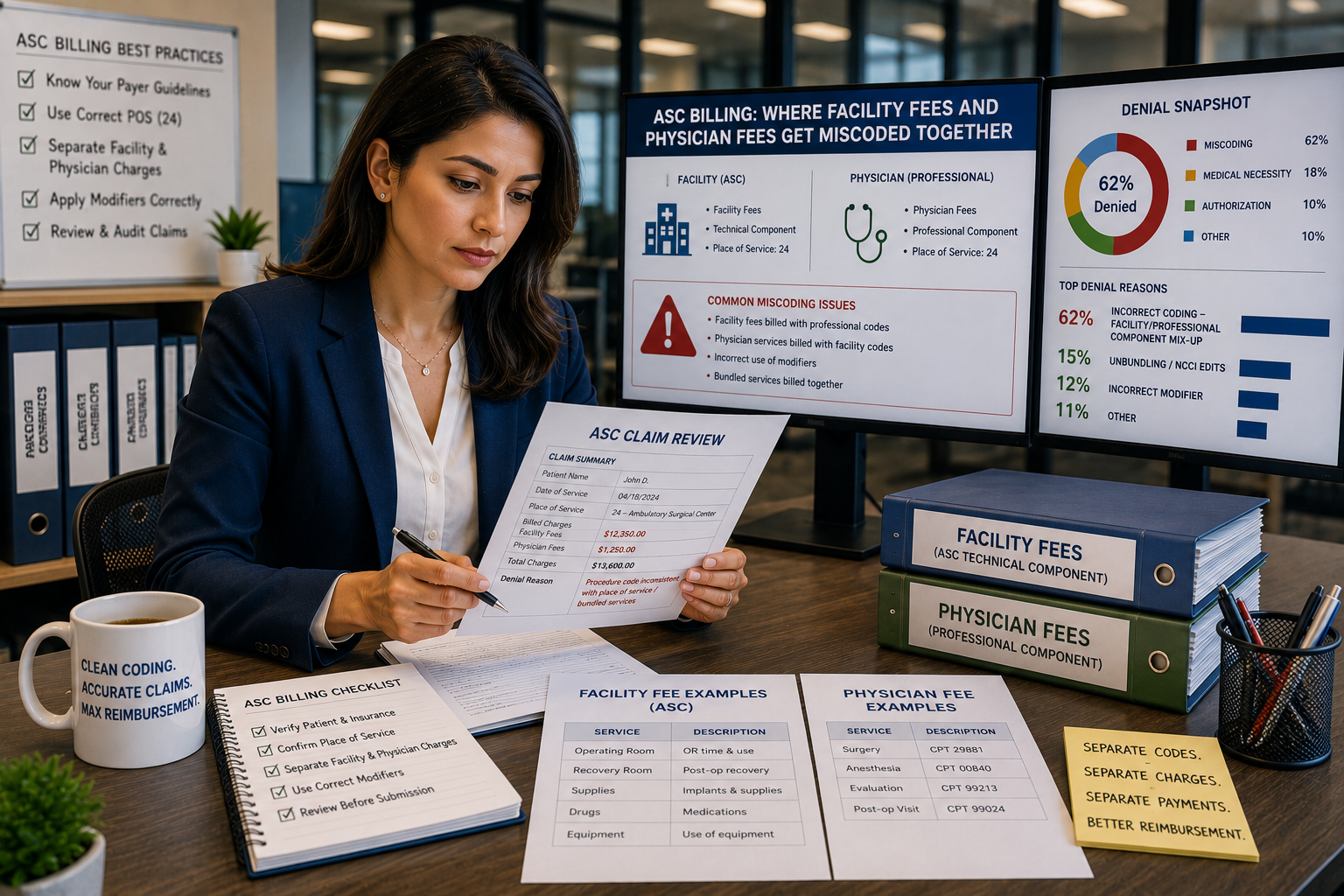
ASC Billing: Where Facility Fees and Physician Fees Get Miscoded Together
ASC facility and physician claims both go out on a CMS-1500 form with the same CPT code and place...
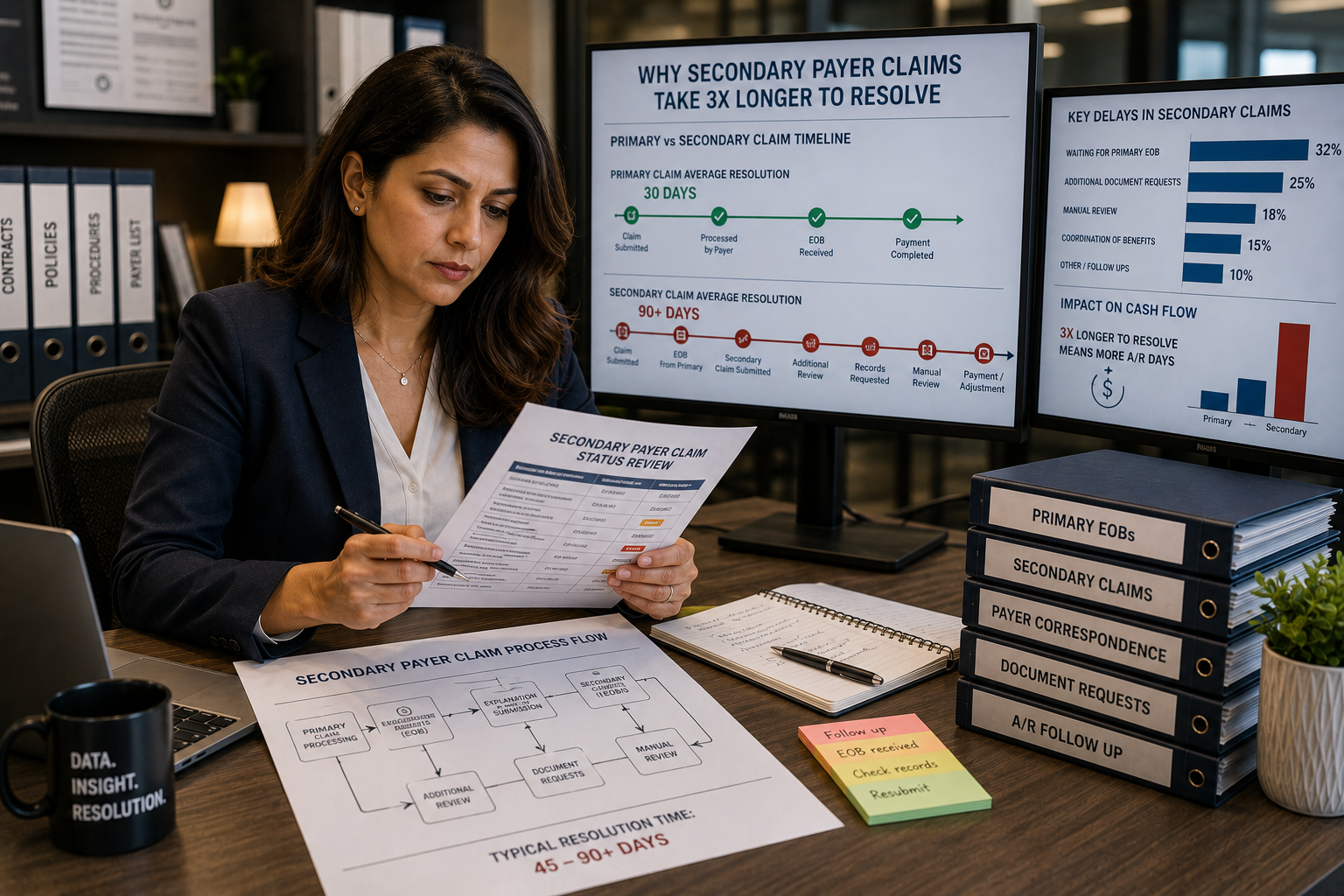
Coordination of benefits errors: why secondary payer claims take 3x longer to resolve
Secondary payer claims stall because coordination of benefits errors, wrong payer order, outdated COB records, and missing primary...