Medical Necessity Documentation Mistakes to Avoid
The Qualigenix Editorial Team comprises certified medical billing professionals, CPC-credentialed coders, prior authorization specialists, and revenue cycle consultants with more than 40 years of combined hands-on experience serving solo physicians, group practices, hospitals, and ASCs across 38+ specialties in the United States. Every guide, article, and resource published on the Qualigenix blog is researched against current CMS guidelines, Federal Register notices, AMA policy updates, and payer-specific billing rules — and reviewed for compliance accuracy before publication. Our content reflects the same standards we apply to our client work: 99% claim accuracy, 95% first-pass acceptance, and a 30% average reduction in AR days.
A claim can look perfect in your billing system, then fall apart the moment a payer asks for records. One missing detail in your note, one vague diagnosis, or one copy-pasted template can turn into a denial, an appeal, or an audit request that ties up your cash flow for weeks.
This is happening more often because payers are checking whether the service was truly needed, not just whether the code was valid. In fact, CMS (Centers for Medicare & Medicaid Services) estimated the Medicare Fee-for-Service improper payment rate at 7.66%, or $31.70 billion in fiscal year 2024, due to insufficient documentation.
Let’s see the most common medical necessity documentation mistakes that trigger denials, and how to fix documentation gaps before the claim submission.
What Is Medical Necessity Documentation?
Medical necessity documentation is the clinical proof in the medical record. It shows that a service was required, appropriate, and supported by the patient’s condition at that time. It is not a single checkbox. It is the full story that connects symptoms, exam findings, assessment, diagnosis, plan, and why the chosen service was the right service right now. Good documentation includes:
- The patient’s symptoms and how severe they are
- Relevant history and risk factors
- Objective findings, such as exam results, vitals, or test results
- Your assessment and treatment justification
- Your plan, follow-up, and expected outcome
- Any prior authorization support details when required
How Payers Evaluate Medical Necessity
Payers do not judge medical necessity based on your intent. They judge it based on what they can see in the record. In review, insurers often compare:
- ICD-10 (International Classification of Diseases) diagnosis support, meaning whether the diagnosis in the chart matches the diagnosis billed
- CPT (Current Procedural Terminology) justification, which implies whether the service billed fits the documented clinical need
- Clinical notes and progress notes, meaning whether the record proves the service was reasonable and necessary
- Their coverage policies, including LCD (Local Coverage Determination) and NCD (National Coverage Determination) rules, when applicable
If your note is vague, missing key details, or does not connect symptoms to services, payers can label it “not medically necessary” and deny payment.
Why Medical Necessity in Medical Billing Drives Payment Decisions
Medical necessity in medical billing is the bridge between clinical care and reimbursement. If your documentation does not clearly support the diagnosis and the service, the payer can deny, downcode, delay for records, or recoup later. It also influences:
- Reimbursement compliance and audit exposure
- Payer audit risk and the chance of recoupments later
- Denial volume and the time your team spends on appeals
Even strong coding can fail when the story does not match the code.
The Link Between Documentation and Claim Denials
Denials happen when the payer cannot match the following three clinical elements in the chart:
- Patient’s Clinical Condition: The diagnosis, differential diagnoses, presenting symptoms, objective findings, relevant comorbidities, and how these factors affect disease severity or treatment complexity
- Service Provided: The specific procedure, diagnostic test, visit complexity level, therapeutic intervention, or medical decision-making you billed
- Medical Necessity Rationale: The third factor is why this particular service was clinically indicated at this time, for this patient. You need to include risk stratification, failed conservative measures, symptom progression, functional impairment, or potential complications being prevented
When documentation does not clearly link all three clinical elements with proper detail, claims often get denied for lack of medical necessity. Payers only review what is written in the medical record. If clinical reasoning, treatment decisions, or supporting details are missing, they assume the service was not justified, even when care was appropriate.
Common Medical Necessity Documentation Mistakes to Avoid

There are many factors that trigger claim denial, but they are entirely preventable with the right clinical details. Here are the common mistakes which affect your claim submission:
-
Diagnosis Does Not Support the Procedure
The most common error is the mismatch between ICD-10 diagnosis support & CPT codes. Your CPT may be technically correct, but the diagnosis in the claim and record does not justify it. Let’s say you are going to submit a brain MRI claim, but you mention R10.9 code (Abdominal pain) instead of R94.02 (Abnormal brain scan).
Payers use LCD and NCD policies that list which diagnoses support which procedures. When your ICD-10 isn’t on their approved list or when it’s too nonspecific, automated edits flag it as “CO-11: Diagnosis inconsistent with procedure”.
How To Avoid It: Choose the most specific ICD-10 code that accurately reflects clinical findings. Document objective exam findings, symptom severity, functional limitations, and why conservative measures failed or aren’t appropriate. Make sure your assessment and plan clearly connect the diagnosis to why this particular service is medically necessary now
-
Missing or Weak Clinical Notes
Payers deny when the record does not show why the service was reasonable and necessary. Incomplete documentation can also cause denial of payment. Your notes should be complete, legible, and include the reason for the encounter, relevant history, findings, test results, assessment, and plan of care. Quick checklist you can add to your workflow:
- Clear chief complaint and relevant history.
- Objective findings and assessment, not just symptoms.
- A plan that explains what you did and why it was needed.
-
Copy Paste or Template Driven Records
Every visit note looks identical because you’re copying previous documentation or auto-filling templates without patient-specific updates. Payers see this pattern and immediately suspect billing fraud.
A patient sees you for six physical therapy visits over three weeks. All six progress notes contain:
- Identical exam findings: Patient tolerated treatment well, ROM improving
- Same treatment plan: Continue current therapy regimen
- Copy-pasted goals: Increase strength and mobility
- No objective measurements showing actual progress
When an auditor reviews these records, they see zero clinical evolution across multiple visits. That’s a red flag. Either the patient isn’t progressing (making continued treatment medically unnecessary) or you’re not documenting what’s actually happening (making the record fraudulent).
-
Lack of Treatment History or Progress Tracking
Documentation doesn’t show what treatments you’ve already tried, how the patient responded, or why continued care remains medically necessary. Records should substantiate not only the service performed but also the required level of care. Suppose you bill for the 8th physical therapy session for lower back pain, but your progress notes never document:
- What conservative treatments were tried first (home exercises, NSAIDs, activity modification)
- Objective progress measures across sessions (pain scales, functional assessments, range of motion)
- Clinical justification for why therapy should continue beyond typical episode limits
- Response to treatment or modifications made when progress plateaued
The payer reviews the request and sees no medical reasoning for ongoing treatment. Their medical director denies visits 7-12 as “not medically necessary” because records don’t show the patient is benefiting or that continued therapy will produce functional improvement.
-
No Link Between Symptoms and Services
Disconnected documentation is another cause of the denial. When your note doesn’t clearly connect symptoms and services, payers can’t see why the procedure was medically necessary. Your note documents:
- Chief Complaint: Right knee pain for 2 weeks
- Exam Findings: Left shoulder shows decreased ROM
- Service Billed: 97110 (therapeutic exercise) targeting the lumbar spine
There’s no explanation for why you’re treating the lumbar spine when the patient complained of knee pain and your exam focused on the shoulder. Even if your clinical reasoning was sound, the disconnected documentation makes it look like you billed for unrelated services.
For fixing this, you can write one or two clear “because” statements in the assessment or plan. For example: “Because the patient has X limitation and failed Y, I am ordering Z to rule out A and guide treatment.”
-
Poor Telehealth Documentation
Telehealth claims fail when you do not document enough to show the service met requirements and supported the plan of care. CMS telehealth guidance also emphasizes documenting in the medical record how telehealth helps achieve the goals outlined in the patient’s plan. A practical telehealth note should clearly state the visit type, modality used, and why telehealth was appropriate for that patient and condition. To fix it, you can do:
- Document modality and limitations
- Document what you assessed
- Add clear follow-up and escalation guidance
-
Missing Prior Authorization Support
Prior authorization approval does not protect you if the clinical documentation in the chart does not match what was authorized or what you billed. Medicare guidance also makes clear that insufficient documentation can invalidate the claim and create overpayment recovery risk after payment. Fix it by aligning three items before the visit or procedure:
- The prior authorization request narrative.
- The chart note and attached clinicals.
- The final billed CPT and diagnosis codes.
For example, if the authorization was based on failed conservative therapy, your record should show what was tried, for how long, and why it did not work.
How Medical Necessity Documentation Errors Impact Revenue
Medical necessity documentation errors directly affect revenue. Many healthcare providers now see average denial rates around 11%, with some clinics reaching 17%. These denials delay payments, increase rework, and reduce overall reimbursement.
Immediate Payment Loss
Denied claims mean zero revenue until you fix them. Take an example, you process 1,000 claims monthly, each averaging $200 in reimbursement. If the denial rate is 10%, then 100 denied claims per month. If you corrected 50% of the denied claim, then $10000 lose per month, which is equal to $1,20,000 lose.
Administrative Burden
Each denied claim costs $25 to $181 just to fix. Your staff spends hours rectifying the documentation, resubmitting claims, and managing appeals instead of processing new revenue. That administrative burden compounds monthly losses.
Cash Flow Disruption
Denied claims not only impact direct revenue loss but also disrupt the cash flow, as appeals take 30 to 90 days to resolve. Those payment delays create gaps that make covering payroll and expenses difficult.
Audits Demand Repayment
Weak clinical documentation standards trigger payer audits. When auditors find problems, they review hundreds of claims and demand repayment for previously approved services. One mistake can cost you years of revenue.
How Qualigenix Helps With Medical Necessity Documentation

Medical necessity documentation improves fastest when you treat it as a process, not an individual habit. Here, Qualigenix helps you reduce denials by tightening the link between clinical documentation and payer rules, so your records prove what your claims are billing. This improves reimbursement compliance and lowers avoidable audit exposure. Here’s how we help:
Pre-submission validation
Most denials start with small gaps, such as missed diagnosis-to-procedure links, incomplete clinical notes, or vague treatment justification. Qualigenix handles pre-claim validation, manages prior authorization support, and applies accurate code matching so claims go out clean and get paid faster.
Diagnosis-to-procedure matching
Medical billing has unique documentation demands. Qualigenix supports hospitals, physician practices, and specialty clinics with specialized workflows tailored to different service types. The platform handles strict payer rules, applies correct CPT justification and ICD-10 diagnosis support standards, and aligns clinical records with billing data to reduce claim denial prevention failures.
End-to-End Support
Our team tracks denials, manages appeals, and validates documentation through one coordinated system. This keeps accounts receivable from piling up, improves cash flow, and gives clinics more time to focus on patient care rather than fighting claim rejections.
Medical Necessity Documentation Approach
Qualigenix uses a 30-60-90 day onboarding approach and provides service level agreements tied to measurable results, such as fewer denials and reduced AR days. This creates a steady workflow where documentation issues are caught early and corrected before they become repeat denials.
Protect Your Revenue With Stronger Documentation Today!
Medical necessity documentation is not paperwork. It is your proof that the care was reasonable, necessary, and supported by the record. When you strengthen ICD to CPT alignment, improve progress notes, and close documentation gaps before submission, you reduce denials and protect yourself from takebacks later. Medicare also makes it clear that insufficient documentation can lead to denials and even overpayment recovery after payment. If you want faster reimbursement and fewer medical necessity denials, build a documentation-first workflow. Partner with Qualigenix to strengthen your clinical notes, reduce payer audit risk, and clean claims with confidence.
FAQs
1. What does medical necessity documentation mean?
Medical necessity documentation proves a treatment is essential, clinically appropriate, and meets standard care guidelines. Payers expect evidence that the service directly addresses the patient’s specific diagnosis or symptoms.
2. Why is medical necessity required for insurance payment?
Medical necessity ensures services meet payer coverage rules and clinical guidelines. Insurers use it to confirm treatments are appropriate, reasonable, and eligible for reimbursement before approving insurance payments.
3. What happens when medical necessity is not documented?
Poor documentation leads to immediate claim denials. Providers then face time-consuming appeals or audits, which can result in heavy financial penalties and the forced repayment of previously processed insurance funds.
4. Is medical necessity required for all claims?
Most clinical claims require this justification. It matters most for high-cost surgeries, specialized imaging like MRIs, and long-term therapies where the risk of over-utilization is significantly higher for insurers.
5. How can clinics improve medical necessity documentation?
Use structured progress notes, match ICD ten diagnosis support to CPT justification, and run pre-bill checks to catch documentation gaps early. Medicare guidance also stresses that the burden of proof remains with the provider.
What’s Next
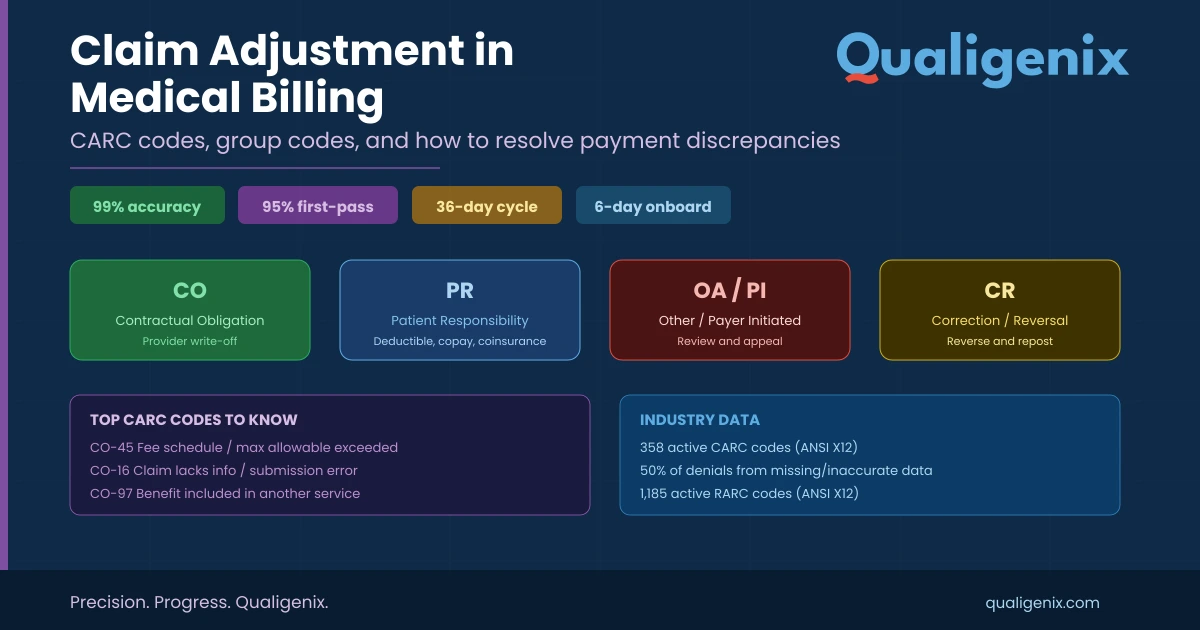
Claim Adjustment in Medical Billing: CARC Codes, Group Codes, and How to Resolve Payment Discrepancies
A claim adjustment occurs when a payer changes the reimbursement amount from what was originally billed. Every adjustment is...
Denial Management in Medical Billing: 7 Common Causes
A patient visits your clinic, receives care, and leaves reassured. The service is documented, the claim is submitted, and...
Effective Strategies for Charge Entry to Maximize Revenue
Most practices focus on coding or collections, but charge entry in medical billing is where revenue strength is truly...