Medical Billing vs Coding: Key Differences Explained
The Qualigenix Editorial Team consists of certified billing and coding experts with over 40 years of experience across 38+ medical specialties. Our content is rigorously researched against CMS, AMA, and payer-specific guidelines to ensure total compliance and accuracy. We apply the same elite standards to our resources as we do our client work, consistently delivering high claim accuracy and significant reductions in AR days.
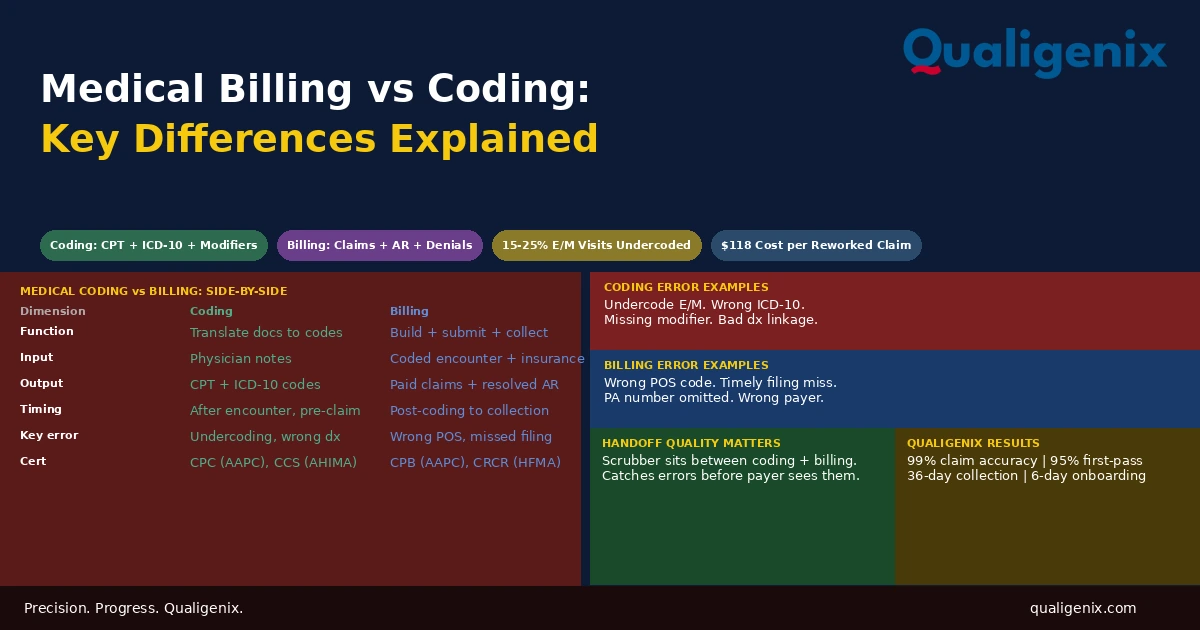
Medical coding and medical billing are two distinct functions that depend on each other to produce a paid claim. Coding translates clinical documentation into standardized codes that describe what the physician did and why. Billing uses those codes to build a claim, submit it to the insurer, track payment, and manage anything that doesn’t pay correctly. Coding comes first. Billing comes second. An error in coding becomes a billing problem. A billing system that doesn’t catch coding errors becomes an error delivery mechanism. Practices that treat both as a single interchangeable function have no way to diagnose where their revenue losses are actually coming from.
When a claim denies, the question a practice needs to answer is: was this a coding problem or a billing problem? The answer determines what needs to be fixed. A wrong CPT code is a coding problem. It originates in the documentation review step and must be fixed there. A claim submitted to the wrong payer is a billing problem. It originates in the submission workflow and must be fixed there. A wrong CPT code submitted to the wrong payer is both — and fixing only one of them doesn’t fix the claim.
Most practices that struggle with chronic denials, low clean claim rates, or unexplained revenue gaps can’t answer that question accurately because they don’t have a clear picture of what coding does, what billing does, and where the handoff between them occurs. The two functions are often performed by the same person, managed under the same label, or outsourced to partners who don’t clearly distinguish between them in their reporting.
This blog explains what medical coding is, what medical billing is, where each begins and ends, how they interact, and what goes wrong in revenue cycles where the distinction between them isn’t clearly understood or actively managed.
Medical coding is the process of translating physician documentation into standardized codes: CPT codes for procedures, ICD-10 codes for diagnoses, and HCPCS codes for supplies and equipment. Medical billing is the process of using those codes to build an insurance claim, submit it to the payer, track it through adjudication, post the payment, and manage denials and patient balances. Coding produces the language. Billing uses the language to collect payment. Both must be accurate for a claim to be paid correctly and on time.
Medical Billing vs Coding: The Side-by-Side Comparison
| Dimension | Medical Coding | Medical Billing |
|---|---|---|
| Primary function | Translate clinical documentation into codes | Use codes to build claims and collect payment |
| Input | Physician notes, operative reports, test results | Coded encounter, patient demographics, insurance data |
| Output | CPT codes, ICD-10 codes, modifiers | Submitted claims, posted payments, worked denials |
| Code sets used | CPT, ICD-10-CM, ICD-10-PCS, HCPCS Level II | Claim forms (CMS-1500, UB-04), payer-specific rules |
| Knowledge required | Clinical anatomy, coding guidelines, documentation standards | Payer rules, claim forms, AR management, denial process |
| When it happens | After the clinical encounter, before claim submission | From claim submission through final payment collection |
| Common errors | Undercoding, wrong diagnosis linkage, missing modifiers | Wrong POS code, timely filing miss, PA number omitted |
| Revenue impact of errors | Underpayment, medical necessity denial, compliance risk | Delayed payment, denial, write-off, recoupment |
| Certifications | CPC (AAPC), CCS (AHIMA) | CPB (AAPC), CRCR (HFMA) |
| Regulatory framework | AMA CPT guidelines, CMS ICD-10 guidelines, OIG compliance | Payer contracts, CMS billing rules, timely filing policies |
What Medical Coding Is and What It Actually Requires
Medical coding is the clinical translation layer of the revenue cycle. Its function is to convert the narrative of a physician’s documentation — what the patient presented with, what the physician examined, what was ordered, what was performed, and what was decided — into a standardized set of codes that a payer’s adjudication system can evaluate against coverage criteria and fee schedules.
The code sets coders work with are distinct and purpose-specific. CPT codes describe what the physician did. ICD-10-CM codes describe what the patient had. HCPCS Level II codes describe supplies, equipment, and certain non-physician services. Modifiers provide context about how a service was performed that changes how the payer should adjudicate it. All of these must work together on a claim: the CPT code must be supported by a diagnosis code that establishes medical necessity, the modifier must be applied correctly to represent the actual circumstances of the service, and the code combination must not trigger a bundling edit that causes the payer to deny one or both codes.
Medical coding is constrained by two things simultaneously: what the documentation supports and what the guidelines allow. A coder cannot assign a code for a service not documented in the clinical note, regardless of whether the physician performed it. And a coder cannot assign a code that isn’t defined in the current code set, regardless of how accurately it would describe the service. The documentation must support the code, and the code must exist and be correctly applied. Both conditions must be true for the coded encounter to be accurate and defensible.
This is why documentation quality is the foundation of coding accuracy. A physician who documents an encounter with enough specificity — the exact diagnoses managed, the data reviewed, the decisions made, the procedures performed with laterality and extent — gives the coder the raw material to assign the most accurate and highest-supported code. A physician who documents minimally forces the coder to either code conservatively to what’s safely supported or return a query that delays charge entry. In both cases, revenue is affected by a documentation decision that happened before coding began.
What Medical Billing Is and What It Actually Requires
Medical billing begins where coding ends. The coder produces a coded encounter: a patient, a date of service, a set of CPT codes, a set of ICD-10 codes, and any modifiers. The biller takes that coded encounter and converts it into an insurance claim that the payer can process.
Building that claim requires information beyond what the coder produces. The patient’s insurance member ID, the rendering provider’s NPI, the billing entity’s NPI and Tax ID, the place-of-service code, the billed charge for each service, and the prior authorization number if the service required one — all of these must be present and accurate on the claim. The biller assembles these pieces, runs the assembled claim through a scrubber to catch errors before submission, and transmits the clean claim electronically through a clearinghouse to the payer.
After submission, billing is a tracking and follow-up function. The biller monitors the claim’s status through adjudication, posts the payment or denial when the ERA arrives, and takes action on anything that doesn’t resolve correctly. Denials are routed for correction or appeal. Underpayments are identified and followed up with the payer. Secondary claims are generated when primary adjudication is complete and secondary coverage exists. Patient balances are billed when insurance processing is done.
The biller’s job is not finished when the claim is submitted. It is finished when the account is collected, written off to a contractual adjustment, or exhausted through appeal. A billing team that measures its performance by claims submitted rather than revenue collected is managing only the first half of its function. The second half is denial management, secondary billing, AR follow-up, patient collections is where most of the revenue difference between high-performing and low-performing billing operations is found.
The Three Code Sets Medical Coders Work With
Understanding the code sets coders use helps practices understand what their coding output should look like and why errors in each produce different kinds of billing problems.
CPT Codes: What Was Done
Current Procedural Terminology codes are published and maintained by the American Medical Association. They are updated annually with new codes, deleted codes, and revised code definitions. CPT codes are five-digit numeric codes organized into major categories: Evaluation and Management, Anesthesia, Surgery, Radiology, Pathology and Laboratory, and Medicine.
For most physician practices, E/M codes are the most frequently used CPT category. For surgical practices, surgical CPT codes represent the majority of revenue. For diagnostic specialties, pathology and laboratory codes dominate. The right CPT code depends on exactly what was documented as having been performed, and the code description must match the clinical service precisely. A CPT code assigned to a service the documentation doesn’t support is an overcoding error. A CPT code that understates the complexity or extent of the service performed is an undercoding error.
ICD-10 Codes: Why It Was Done
ICD-10-CM codes are the diagnosis classification system used for physician claims. They are alphanumeric codes of up to seven characters that identify specific diseases, conditions, symptoms, injuries, and reasons for encounters. The ICD-10 system has over 70,000 codes, providing a level of specificity that allows precise communication of a patient’s clinical situation.
The ICD-10 code on a claim establishes medical necessity. The payer asks, in effect: given this diagnosis, does this service make clinical sense? A patient with a confirmed shoulder tear receiving a shoulder MRI — the diagnosis supports the service. A patient with lower back pain receiving a knee MRI — the diagnosis doesn’t support the service, and the claim will deny for medical necessity unless the documentation and the code selection are revised to reflect the actual clinical situation.
ICD-10 specificity matters as much as ICD-10 accuracy. A code that is technically correct but overly general — using “diabetes mellitus, unspecified” when the documentation clearly documents type 2 diabetes with diabetic neuropathy — is both a documentation accuracy problem and a coding specificity problem. Payers may require the specific code for certain clinical decision-making purposes, and in quality reporting contexts, unspecified codes misrepresent the patient’s actual condition.
HCPCS Level II Codes: Supplies and Equipment
HCPCS Level II codes cover services and supplies not described by CPT codes: durable medical equipment, orthotics, prosthetics, drugs administered by a physician, and certain non-physician services. For practices that provide infusions, administer injectable medications, or dispense supplies and equipment, HCPCS codes are a significant part of the billing code set. Each drug administered by a physician has a J-code (a type of HCPCS code) that identifies the specific drug, its form, and the unit of billing.
Where Coding Errors Become Billing Problems
The handoff between coding and billing is the most consequential point in the revenue cycle. Every error in the coded encounter that is not caught before claim submission becomes a billing problem: a denial to work, a resubmission to manage, an appeal to pursue, or in the worst case a write-off to absorb.
Undercoding: The Revenue Loss That Doesn’t Show Up as a Denial
Undercoding is assigning a lower-level CPT code than the documentation supports. A physician who bills 99213 when the note documents moderate MDM complexity supporting 99214 is undercoding. The claim pays at the lower rate. There is no denial. There is no audit flag. There is simply less revenue than the practice was entitled to on every undercoded encounter, compounding across months and years.
Research consistently shows that 15% to 25% of outpatient E/M visits are billed below the level the documentation supports. For a physician seeing 20 patients per day, that’s three to five undercoded visits every day. At $35 to $50 per visit in Medicare reimbursement difference between adjacent E/M codes, the annual revenue impact per physician ranges from $10,000 to $50,000 depending on specialty and payer mix. No denial queue surfaces this. No billing report flags it. Only a code distribution audit comparing the physician’s E/M code mix against specialty benchmarks reveals the pattern.
Missing Modifiers: The Bundling Denial
When a modifier is required but missing, the payer bundles services that should have been paid separately or denies one of the codes because the submission looks like a billing error. Modifier 25 on same-day E/M and procedure combinations is the most common example. Without it, the E/M bundles into the procedure and the E/M charge denies. The procedure was coded correctly. The E/M was coded correctly. The missing modifier was a coding output gap that became a billing denial.
Wrong Diagnosis Linkage: The Medical Necessity Denial
Each CPT code on a claim must be linked to an ICD-10 code that justifies its medical necessity. When a procedure is linked to a diagnosis that doesn’t support it — either because the coder selected the wrong diagnosis code, used an unspecified code when a specific one was required, or the diagnosis legitimately doesn’t match the service — the payer denies the procedure for medical necessity. The denial looks like a billing denial when the claim reaches the AR queue, but the root cause is in the coding step.
Where Billing Errors Have Nothing to Do With Coding
Not every billing problem originates in coding. Several categories of billing failures have nothing to do with the accuracy of the coded encounter and require the biller’s own process controls to prevent.
Place-of-Service Code Errors
The place-of-service code on the CMS-1500 tells the payer where the service was delivered and determines which fee schedule rate applies. POS 11 for an office-based service triggers the non-facility rate. POS 21 for an inpatient hospital service triggers the lower facility rate. A biller who applies the wrong POS code billing POS 11 for a hospital encounter, or POS 21 for an office visit creates a reimbursement error that has nothing to do with how the service was coded. It is a claim construction error in the billing step.
Timely Filing Violations
Medicare requires claims within 12 months of the date of service. Most commercial payers require 90 to 180 days. A claim submitted after the timely filing deadline denies and cannot be appealed based on late filing. Timely filing violations have no coding component. They result entirely from billing workflow failures: charge lag, pending claim backlogs, claims that sit in a hold status without anyone following up. The code was right. The claim was built correctly. It just wasn’t submitted on time.
Authorization Number Omissions
When a service required prior authorization and authorization was obtained, the authorization number must appear on the claim. A claim submitted without the PA number denies even though the authorization was legitimate and active. This is a billing workflow failure, not a coding error. The code on the claim was correct. The claim was built correctly. The PA number field was empty because no one linked the approved authorization to the billing record for that encounter.
Provider Enrollment Gaps
A claim submitted under a provider not enrolled with the payer denies automatically. This has nothing to do with coding. The service was coded correctly. The claim was built correctly. The provider’s NPI was not recognized by the payer’s adjudication system as an enrolled participating provider. The denial originates in the credentialing and enrollment function, which precedes both coding and billing.
Related: Provider Credentialing Services | Payer Enrollment Services
How Coding and Billing Interact in the Revenue Cycle
The revenue cycle is the full sequence of processes from patient registration through final payment collection. Coding and billing each occupy specific positions in that sequence, and their interaction determines the quality of the claim at the point where it matters most: when the payer adjudicates it.
The sequence looks like this: patient registration captures demographics and insurance. Eligibility verification confirms coverage before the visit. The physician delivers care and documents the encounter. The coder reviews documentation and assigns codes. The biller builds the claim from the coded encounter, scrubs it, and submits. The payer adjudicates. The biller posts the result and follows up on anything unpaid. Each function feeds the next.
The handoff between coding and billing is where the integrated quality of the claim is determined. A claim scrubber that sits between coding output and claim submission catches errors that the coder missed before they reach the payer. This is the intersection where a claim can still be corrected without cost. Once the claim is submitted with an error, correction requires denial management or resubmission, each of which costs time and money.
Related: What Is RCM in Medical Billing | What Is Claim Submission in Medical Billing
Why Practices Struggle to Diagnose Revenue Problems Without This Distinction
When a practice looks at its denial queue and sees a denial rate above the benchmark, the first management question is: where is this coming from? Without a clear understanding of what coding produces and what billing produces, the answer is always ambiguous. The denial could be a coding problem, a billing problem, a credentialing problem, or a registration problem. Each requires a different fix. Applying a billing fix to a coding problem leaves the coding problem in place and produces the same denial on the next claim.
The practices that diagnose and fix revenue cycle problems most effectively are the ones that can look at a denial and trace it to its origin. Medical necessity denial on claim 1234: is the ICD-10 code wrong (coding problem) or is the diagnosis correct but doesn’t meet the payer’s coverage criteria for this service (coverage determination that may require a PA or a different service)? Bundling denial on claim 5678: is modifier 25 missing (coding output gap) or was modifier 25 present but rejected by a scrubber rule that’s misconfigured (billing system configuration problem)? Wrong NPI denial on claim 9012: is the NPI incorrect on the claim (billing data entry error) or is the NPI correct but the provider isn’t enrolled with this payer (credentialing problem)?
Each diagnosis leads to a different fix. Getting to the right diagnosis requires understanding which function was responsible for the step that produced the error.
Skills and Expertise: What Each Role Requires
The skills required for medical coding and medical billing are distinct. This is one reason the two roles, when combined in a single person at higher volumes, often result in one function being performed less well than the other not because the person is inadequate, but because the knowledge domains don’t overlap as much as the combined title implies.
Medical coding requires strong clinical knowledge. A coder working in orthopedics needs to understand anatomical terminology, surgical approaches, the difference between diagnostic and interventional procedures, and how the documentation of each maps to the CPT code set. A coder working in oncology needs to understand chemotherapy administration protocols, the distinction between evaluation and treatment services, and how pathology coding works. Coding expertise is specialty-specific and deep.
Medical billing requires strong administrative and payer process knowledge. A biller needs to know which payers require what forms, what claim fields each payer validates at submission, how each payer’s denial code taxonomy maps to action steps, what the timely filing window is for each payer in the practice’s payer mix, and how to navigate each payer’s appeal process. Billing expertise is payer-specific and process-oriented.
The overlap between these skill sets is meaningful, a good coder understands how their coding output affects billing, and a good biller understands what coding produces but they are not the same job. At high volume, separating them produces better outcomes in both functions because each can be performed by someone whose expertise is concentrated in the right domain.
Certifications: What They Indicate About Each Role
Medical coding certifications from the American Academy of Professional Coders (AAPC) and the American Health Information Management Association (AHIMA) are the most widely recognized credentials in the field. The AAPC’s Certified Professional Coder (CPC) credential and AHIMA’s Certified Coding Specialist (CCS) both require passing a proctored examination demonstrating proficiency in CPT, ICD-10, HCPCS, and coding guidelines. Many coders hold specialty-specific credentials in addition to the base certification, such as the AAPC’s specialty certifications in orthopedics, cardiology, or oncology coding.
Medical billing certifications from AAPC (Certified Professional Biller, CPB) and HFMA (Certified Revenue Cycle Representative, CRCR) demonstrate knowledge of billing workflows, denial management, payer contracting, and revenue cycle performance metrics. These credentials focus on the operational and administrative dimensions of the billing function rather than the clinical knowledge base that defines coding expertise.
Neither role legally requires certification. But certified professionals have demonstrated their competency through an independent standard, which gives practices a reference point for evaluating the quality of the coding or billing they are receiving from in-house staff or an outsourced partner.
How Qualigenix Manages Both Coding and Billing
At Qualigenix, we manage medical coding and medical billing as integrated but distinct functions in the revenue cycle for practices across 38+ specialties. Our coders are specialty-trained and apply current AMA E/M guidelines, specialty-specific CPT coding standards, and ICD-10 specificity requirements to every coded encounter. Our billers apply payer-specific claim construction rules, manage the full AR cycle from submission through collection, and route denials based on their root cause coding, billing, credentialing, or coverage to the appropriate resolution pathway.
We run monthly E/M code distribution reports that identify undercoding patterns before they compound into annual revenue losses. We configure claim scrubber rules that catch modifier errors and diagnosis linkage gaps between the coding output and the billing submission. We maintain a coding-to-billing feedback loop that gives coders specific, timely information when their output produces a denial category, allowing them to correct the pattern at its source rather than working the same denial type indefinitely.
Our results reflect both functions operating correctly together: 99% claim accuracy rate, 95% first-pass acceptance rate, 36-day average collection cycle, and 30% reduction in AR days. We onboard new clients in as few as 6 days.
Related: Outpatient Coding Accuracy at Scale | What Is Physician Billing | Charge Capture for High-Volume Specialties
Medical Billing and Coding Readiness Checklist
- E/M code distribution reviewed monthly per physician against specialty benchmarks
- Quarterly chart audits confirm coding accurately reflects documented complexity
- ICD-10 codes at maximum specificity — no unspecified codes where specific codes are documented
- Diagnosis-to-procedure linkage verified — each CPT linked to a supporting ICD-10 code
- Modifier 25 applied for same-day E/M and procedure combinations
- Claim scrubber rules current and updated quarterly with payer edit changes
- Place-of-service codes verified accurate for each service delivery location
- Charge entry completed within 24 hours of each encounter
- Authorization numbers recorded and included on applicable claims
- Timely filing deadlines tracked by payer with pending claims reviewed weekly
- Denial root cause identified for every denial: coding, billing, credentialing, or coverage
- Coding-to-billing feedback loop in place with prompt turnaround on coder queries
Frequently Asked Questions: Medical Billing vs Coding
What is the difference between medical billing and medical coding?
Medical coding translates clinical documentation into standardized CPT, ICD-10, and HCPCS codes. Medical billing uses those codes to build insurance claims, submit them to payers, post payments, and manage denials and patient balances. Coding produces the language a payer’s adjudication system reads. Billing uses that language to collect payment. A coding error becomes a billing problem when the claim submits. A billing error can undermine an accurately coded claim just as completely. Both must work correctly for the revenue cycle to produce accurate, timely collections.
What does a medical coder do?
A medical coder reviews physician documentation and assigns CPT codes for procedures, ICD-10 codes for diagnoses, and modifiers that provide context about how services were delivered. The coder’s output is the coded encounter that becomes the foundation of the insurance claim. Coding accuracy determines whether the claim is paid at the correct rate, whether medical necessity is established, and whether the code combinations pass payer edit rules. Documentation quality determines what the coder can accurately and defensibly assign.
What does a medical biller do?
A medical biller builds insurance claims from coded encounters, scrubs them for errors, submits them electronically to payers, tracks them through adjudication, posts payments, and manages denials, secondary billing, and patient balance follow-up. The biller’s job begins when coding ends and finishes when the account is collected or written off. A billing team that measures performance by claims submitted rather than revenue collected is managing only the first half of its function.
Can one person do both medical billing and coding?
In small practices one person often performs both, which is manageable at low volume but creates quality risks as patient volume increases. The skills required are distinct: coding requires deep clinical and code-set knowledge while billing requires payer-specific process expertise and AR management skills. At higher volumes, separating the functions allows each to be performed by a specialist, improving accuracy in both. The combination role becomes the bottleneck that limits how well either function can be performed as the practice grows.
What are CPT codes and who assigns them?
CPT codes are five-digit AMA-published codes describing medical, surgical, and diagnostic services. They are assigned by medical coders based on physician documentation. CPT codes are updated annually. They tell the payer what was done and are the basis for fee schedule reimbursement. A CPT code that doesn’t match what was documented is a coding error. A CPT code that understates the complexity of the service performed is undercoding that costs revenue on every affected encounter without producing a denial.
What are ICD-10 codes and why are they required on claims?
ICD-10 codes identify the patient’s diagnoses and conditions, and they are required on every claim to establish medical necessity for the services billed. Without a supporting ICD-10 code, or with a code that doesn’t match the service billed, the payer denies the claim for medical necessity. ICD-10 specificity matters as much as accuracy: an unspecified code where a specific one is documented represents a missed opportunity for accurate billing and creates quality reporting gaps that compound over time.
What is the revenue cycle and where do billing and coding fit?
The revenue cycle runs from patient registration through final payment collection. Coding occurs after the clinical encounter but before claim submission. Billing spans from claim submission through AR management and patient collections. Registration and eligibility verification precede coding. Payment posting and denial management follow billing. Coding and billing together form the core of the claim generation and collection functions. Quality failures at either stage produce revenue losses, but they require different fixes depending on where the failure originates.
Related Resources from Qualigenix
Coding Gets Claims Right. Billing Gets Them Paid. We Do Both.
Qualigenix manages medical coding and billing as integrated, distinct functions for practices across 38+ specialties. Specialty-trained coders. Payer-specific billers. One partner. No handoff gaps.
Our team delivers 99% claim accuracy, a 95% first-pass acceptance rate, an average 36-day collection cycle, and a 30% reduction in AR days. We onboard in as few as 6 days.
Precision. Progress. Qualigenix.
What’s Next

Medical Coding Errors That Cost Practices the Most (And How to Catch Them Before They Submit)
Medical Coding Errors That Cost Practices the Most (And How to Catch Them Before They Submit) Written by the...
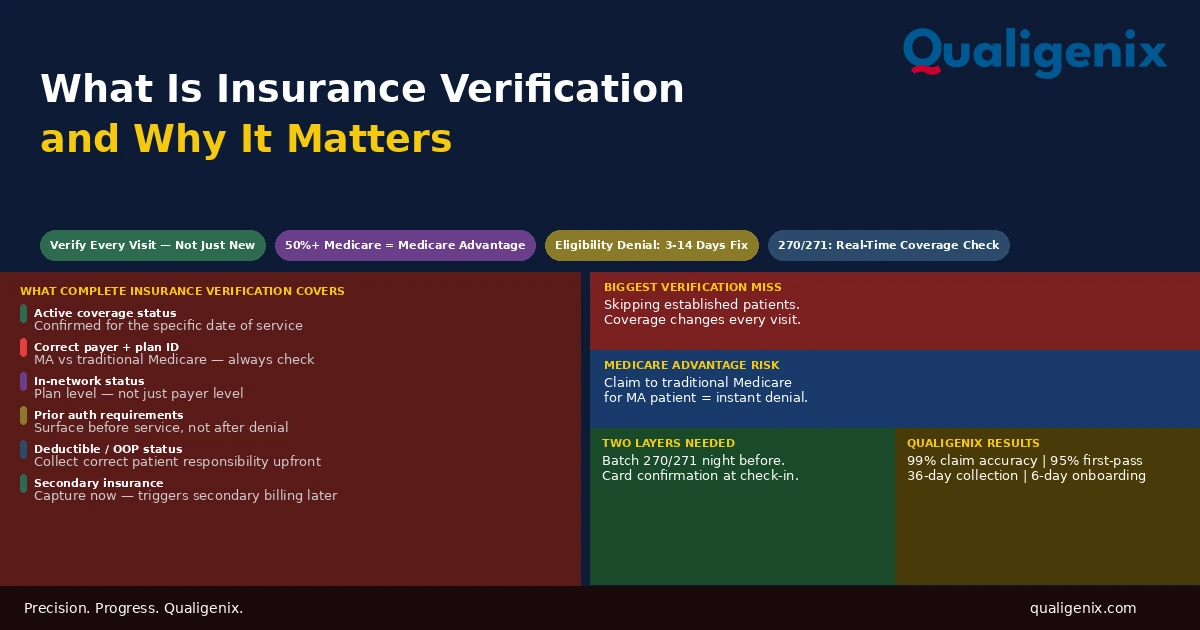
What Is Insurance Verification and Why It Matters
Insurance verification is the front-end process that determines whether a claim will be paid before the patient ever enters...

Insurance Denial Appeals: What Practices Miss
Most insurance denial appeals that fail don’t fail because the clinical case was weak. They fail because the...