What Is RCM in Medical Billing and Why It Determines Whether Your Practice Gets Paid
The Qualigenix Editorial Team consists of certified billing and coding experts with over 40 years of experience across 38+ medical specialties. Our content is rigorously researched against CMS, AMA, and payer-specific guidelines to ensure total compliance and accuracy. We apply the same elite standards to our resources as we do our client work, consistently delivering high claim accuracy and significant reductions in AR days.
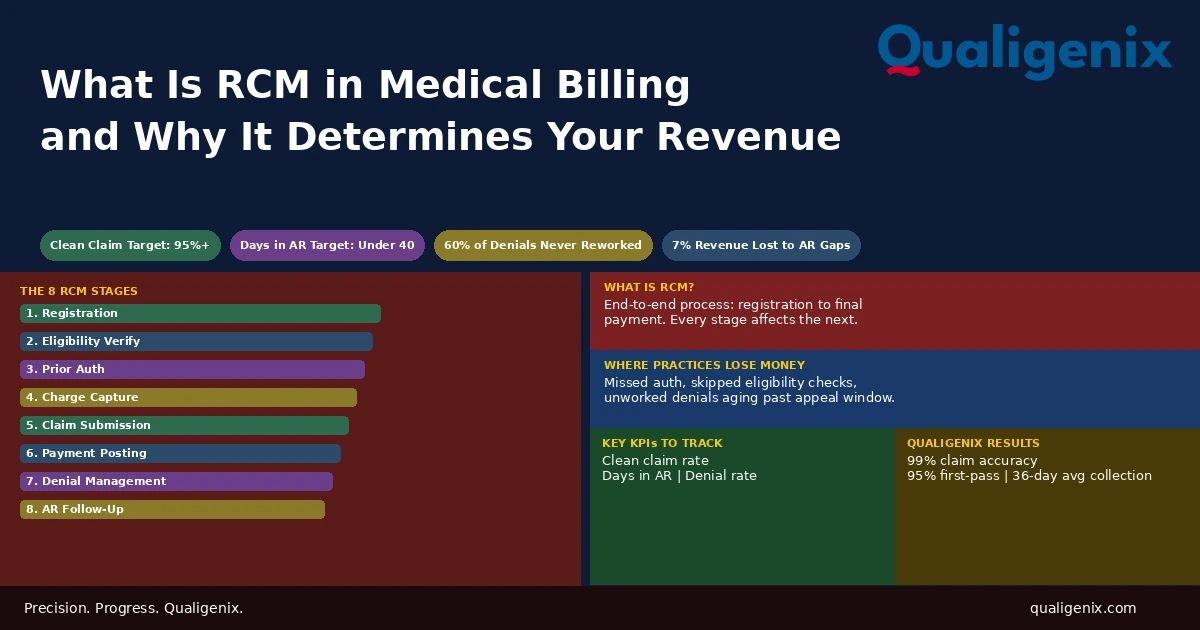
RCM in medical billing stands for Revenue Cycle Management. It’s the full process from the moment a patient schedules an appointment to the moment a practice collects final payment. Every stage in that cycle, from registration through denial management, is connected. One broken step reduces what every step after it can collect.
Most practices think about billing when a claim denies or a payment doesn’t arrive. That’s already too late. The decisions that determine whether a practice gets paid happen before a single code is entered. They happen at registration, at eligibility verification, at prior authorization. By the time a claim reaches a payer, the outcome is largely determined by what happened upstream.
That’s what RCM is. It’s not just billing. It’s the full system that connects patient intake to final payment collection, and every link in that chain is either holding or breaking your revenue.
This blog explains what RCM in medical billing actually covers, what each stage does, where practices consistently lose money, and what a functioning revenue cycle looks like in practice.
RCM in medical billing stands for Revenue Cycle Management. It is the complete process healthcare practices use to manage every financial interaction with a patient, from pre-visit insurance verification and prior authorization through charge capture, claim submission, payment posting, denial management, and AR follow-up. A practice’s RCM performance determines its clean claim rate, days in AR, and ultimately how much of what it earns it actually collects.
RCM in Medical Billing: Key Benchmarks and Numbers
| Metric | Benchmark / Data Point | Source |
|---|---|---|
| Industry benchmark clean claim rate | 95% or higher | MGMA Revenue Cycle Survey |
| Target days in AR for healthy practices | Under 40 days | Healthcare billing benchmarks |
| High-performing practice days in AR | 30 to 35 days | MGMA performance data |
| Industry average denial rate on first submission | 10% to 15% of claims | CAQH operational benchmarks |
| Target denial rate for well-run RCM | Under 5% | Revenue cycle industry standards |
| Denied claims never reworked by practices | Approximately 60% | Change Healthcare denial data |
| Cost to rework a single denied claim | $25 to $118 per claim | MGMA administrative cost data |
| Revenue in AR past 90 days typically collected | Only about 20% | Healthcare AR aging benchmarks |
| Revenue lost to uncollected AR annually | Up to 7% of net revenue | MGMA revenue cycle survey |
| Qualigenix claim accuracy rate | 99% | Qualigenix performance data |
| Qualigenix first-pass acceptance rate | 95% | Qualigenix performance data |
| Qualigenix average collection cycle | 36 days | Qualigenix performance data |
| Qualigenix AR days reduction | 30% | Qualigenix performance data |
| Qualigenix client onboarding time | 6 days | Qualigenix operations data |
What RCM in Medical Billing Actually Covers
Revenue Cycle Management is the end-to-end process that moves a patient encounter from intake to paid claim. The term gets used loosely. Some people use it to mean medical billing. Others use it to mean just the AR and collections side. In a complete definition, RCM covers eight distinct functional areas, and all eight must work together for the cycle to close cleanly.
Think of it as a chain. A patient calls to schedule. They show up for their visit. They receive care. Their services get coded. A claim gets built and submitted. The payer responds with payment or denial. The payment gets posted. Any balance gets followed up. If that chain runs without breaks, the practice gets paid accurately and quickly. If any link fails, everything downstream from it is compromised.
The practical answer to “what is RCM in medical billing” is this: it’s the system that determines how much of what a practice earns it actually collects. Billing is one part of that system. RCM is the whole thing.
Most practices don’t have a complete RCM system. They have billing software, a front desk that collects copays, and a biller who works denials when they have time. That’s not RCM. That’s billing with gaps. The gaps are where the revenue goes.
Stage 1: Patient Registration and Demographics
RCM starts before any clinical care is delivered. It starts when a patient calls to schedule, when they check in at the front desk, or when their information is entered into a practice management system. The accuracy of that intake data determines whether every downstream billing step works correctly.
A patient’s name, date of birth, and insurance ID entered incorrectly at registration will produce a claim that fails payer edits. The claim denies. Staff must find the error, correct it, and resubmit. If timely filing windows are tight, the delay may cost the practice the payment entirely. None of this has anything to do with the care delivered or the accuracy of the coding. It starts and ends with a data entry mistake at intake.
Front desk staff who collect demographics are performing an RCM function. Practices that don’t train them to treat intake as a billing-critical task are setting their billing team up to fix problems that never needed to happen.
What Strong Registration Looks Like
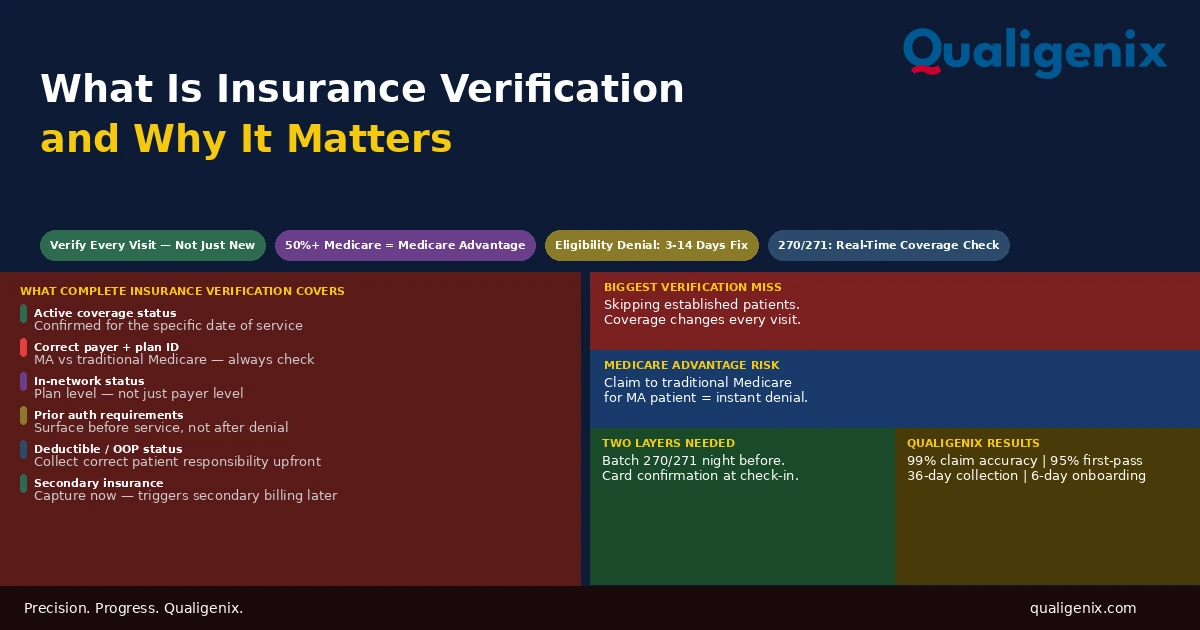
A well-run registration process collects the patient’s legal name exactly as it appears on their insurance card, their insurance member ID and group number, their date of birth, their guarantor information, and any secondary insurance. It also captures a copy of the insurance card front and back. For Medicare patients, it collects the Medicare Beneficiary Identifier (MBI). For Medicaid patients, it verifies the state program and plan.
Practices with electronic intake forms that feed directly into the practice management system reduce manual entry errors. Practices that still rely on paper intake and manual data transcription introduce error at every step of that transfer.
Stage 2: Insurance Eligibility Verification
Once registration is complete, the next RCM step is confirming that the patient’s insurance coverage is active and that your practice is in network with their plan. This is eligibility verification, and it must happen before the visit, not after.
A patient who shows up assuming their insurance is current may have had a coverage lapse. Their employer may have changed plans. They may have enrolled in a Medicare Advantage plan that replaces their traditional Medicare. None of these changes will show up at the front desk unless someone checks. If no one checks, the practice delivers care, submits a claim to the wrong payer or an inactive plan, and receives a denial that requires rework or, more likely, gets written off.
Warning: Eligibility verification done only at initial intake misses coverage changes between visits. For patients with chronic conditions who return regularly, coverage can change at any point during a plan year. Every visit requires a fresh eligibility check. Practices that verify once and assume coverage is stable will eventually bill the wrong payer and absorb the denial cost.
Eligibility verification uses HIPAA 270/271 electronic transactions. A 270 query goes to the payer. A 271 response comes back with the patient’s coverage details: active status, plan type, deductible met-to-date, copay amounts, and any coordination of benefits with a secondary plan. Done in real time, this check takes under three seconds. Done by phone, it takes 10 to 20 minutes and returns less complete information.
Stage 3: Prior Authorization
Some services require payer approval before they can be performed. This is prior authorization, and it is one of the most common sources of back-end denials in medical billing. The service gets performed. The claim gets submitted. The denial comes back weeks later: prior authorization required and not obtained. At that point, the appeal window is narrow, the documentation burden is high, and the outcome is uncertain.
Prior authorization is a front-end RCM function. It belongs in the workflow before the appointment, not on the denial management worklist afterward. Practices that don’t track which services their payers require authorization for, and don’t have a process to obtain and document that authorization in advance, will generate preventable denials at a predictable and recurring rate.
Authorization requirements change frequently. Payers add new services to their authorization lists, modify existing requirements, and sometimes remove them. An authorization tracking system that was accurate six months ago may be missing current requirements. The only way to stay current is to audit authorization requirements against payer policies on a regular schedule, not to rely on historical knowledge.
Stage 4: Charge Capture and Medical Coding
After care is delivered, charge capture and coding translate the clinical encounter into billable data. Charge capture is the act of recording every service, procedure, and supply that was provided. Coding assigns the correct CPT procedure codes, ICD-10 diagnosis codes, and any required modifiers to those services.
Both must be accurate. A service that isn’t captured can’t be billed. A service that’s captured but coded incorrectly produces a claim that either denies or reimburses at the wrong rate. Undercoding means the practice collects less than it’s entitled to. Overcoding creates compliance risk and potential audit exposure.
Charge capture and coding are where clinical reality becomes billing data. The quality of this translation determines the accuracy of every claim that follows. Practices that treat coding as a back-office administrative task rather than a clinical-billing bridge will see it in their denial rates.
High-volume practices with many providers face additional charge capture risk. When providers see 15 to 20 patients per shift and enter charges from memory hours later, charges get missed and codes get simplified. A charge capture workflow that requires same-day or next-day entry, combined with regular code distribution audits, catches these patterns before they compound into significant revenue loss.
Stage 5: Claim Submission and Scrubbing
Once charges are coded, claims are built and submitted to payers. Before submission, a clean claim goes through a scrubber: software that checks the claim against payer edits for common errors including missing modifiers, invalid code combinations, incorrect place-of-service codes, and missing required fields.
Claims that pass the scrubber go out clean. Claims that fail are flagged for correction before submission. The goal of claim scrubbing is to catch errors internally before a payer rejects the claim, which adds days or weeks to the payment timeline and requires staff time to correct and resubmit.
The industry benchmark clean claim rate is 95% or higher. Practices below 90% are spending significant staff time on rework. Each rework event costs between $25 and $118 depending on the complexity of the correction and the payer’s requirements. At scale, a poor clean claim rate is one of the most expensive operational problems a billing department can have, and one of the most fixable once the root causes are identified.
Timely Filing Windows
Every payer sets a timely filing deadline: the window from the date of service within which a claim must be submitted. Medicare’s timely filing limit is 12 months. Many commercial payers set shorter windows of 90 days to 180 days. Claims submitted after the deadline are denied on the basis of timely filing, and those denials typically can’t be appealed except in very narrow circumstances.
Timely filing denials are almost always avoidable. They result from charge lag (delays between service delivery and charge entry), claim scrubbing backlogs, or missing information that holds a claim in a pending status for too long. A clean claim submitted quickly is one of the easiest RCM wins a practice can achieve.
Stage 6: Payment Posting
When a payer processes a claim and issues payment, a remittance advice (ERA or EOB) arrives showing what was paid, what was adjusted, and what was denied. Payment posting is the process of recording that information accurately in the practice management system.
Accurate payment posting matters for two reasons. First, it gives you a real picture of your AR. If payments are posted incorrectly or in lump sums without proper allocation to individual claims, your AR reports become unreliable. You can’t manage what you can’t measure accurately. Second, payment posting is where underpayments get identified. If a payer pays $85 on a service your contract says should reimburse $110, that discrepancy needs to be caught and challenged at this stage, not written off as a contractual adjustment.
Many practices post payments too slowly, in batches days after the ERA arrives, or inconsistently across different payers. Slow or inaccurate posting inflates days in AR artificially and masks underpayment patterns that are recoverable with a timely challenge.
Stage 7: Denial Management
Despite best efforts, claims get denied. Denial management is the RCM process of working those denials: identifying the reason, correcting the error or building an appeal, resubmitting, and tracking the claim through to resolution.
The most important fact about denials is this: approximately 60% of denied claims are never reworked. They sit in a denial queue, age past the appeal deadline, and get written off as bad debt. That’s not a billing problem. That’s a workflow problem. A denial that isn’t worked within the payer’s appeal window is revenue that’s gone.
Warning: Denial management without root cause analysis is just rework. If the same denial reason keeps appearing across multiple claims, fixing individual claims doesn’t fix the problem. Root cause analysis identifies whether the denial is a registration error, a coding issue, a missing authorization, or a payer policy change, and corrects the upstream process so the denial stops recurring.
Categories of Denial Reasons
Denials fall into three broad categories. Administrative denials are caused by front-end errors: wrong member ID, invalid diagnosis code, missing prior authorization, or untimely filing. These are almost always fixable with a corrected claim. Clinical denials are based on the payer’s determination that the service wasn’t medically necessary. These require an appeal with clinical documentation. Contractual denials happen when a service isn’t covered under the patient’s plan. These require either a patient billing step or a write-off.
A healthy denial management workflow tracks denial reasons by category, by payer, and by provider. The pattern in that data tells you where to fix the upstream process. Practices that just work denials one by one and never analyze the pattern are treating symptoms instead of causes.
Stage 8: Accounts Receivable Follow-Up and Patient Collections
The final stage of RCM is following up on outstanding balances. After a payer adjudicates a claim, the patient may owe a portion: their deductible, copay, or coinsurance. That balance must be billed to the patient and collected. On the payer side, claims that are processed but unpaid past expected payment timelines need active follow-up to determine the cause and push the payment through.
AR is tracked in aging buckets: 0 to 30 days, 31 to 60 days, 61 to 90 days, and 90 days plus. A healthy practice keeps the large majority of its AR in the 0 to 30 day bucket. Balances that age past 90 days become statistically difficult to collect. Research consistently shows that only about 20% of AR past 90 days is ultimately collected. The older it gets, the less of it comes back.
Days in AR is the single most useful summary metric for RCM health. A days in AR under 40 indicates a well-functioning cycle. Days in AR above 50 indicates a systemic problem somewhere in the cycle. It may be a denial management backlog. It may be slow payment posting. It may be a patient collections process that doesn’t follow up consistently. Whatever the cause, high days in AR is the symptom that shows up in financial reports when RCM breaks down.
Where RCM and Provider Credentialing Connect
One RCM failure that many practices don’t think of as a billing problem is provider credentialing. A provider who isn’t credentialed and enrolled with a payer can’t bill that payer for services. Claims submitted under a non-enrolled provider deny automatically. There’s no appeal that fixes a credentialing gap. The only fix is completing enrollment before the provider sees patients under that payer.
Credentialing gaps hit hardest when a new provider joins a practice. Medicare enrollment takes 60 to 90 days on average. Commercial payer credentialing takes 90 to 120 days. If a practice starts a new provider seeing patients on day one without a credentialing plan in place, it’s generating uncompensated care for the length of that enrollment period.
Revalidation creates the same problem on a recurring basis. Medicare requires providers to revalidate their enrollment every five years. Missing a revalidation deadline can suspend billing privileges with little warning. A practice whose provider gets their Medicare billing deactivated mid-year will see a sudden, unexplained drop in collections that traces back not to billing errors, but to an expired enrollment.
Internal links: Provider Credentialing Services | Payer Enrollment Services | Healthcare Credentialing 2026
The 5 KPIs That Tell You Whether Your RCM Is Working
RCM performance is measurable. These five metrics give a complete picture of revenue cycle health. If you don’t track all five, you’re managing your practice’s finances with partial information.
| KPI | What It Measures | Target | Warning Level |
|---|---|---|---|
| Clean Claim Rate | Claims paid on first submission without correction | 95% or higher | Below 90% |
| First-Pass Acceptance Rate | Claims accepted by payer on first pass | 95% or higher | Below 90% |
| Days in AR | Average days from service to payment | Under 40 days | Above 50 days |
| Denial Rate | Percentage of submitted claims denied | Under 5% | Above 10% |
| Net Collection Rate | Percentage of collectible revenue actually collected | 95% or higher | Below 90% |
How Qualigenix Manages the Full RCM Cycle
At Qualigenix, we manage the complete revenue cycle for practices across 38+ specialties. That means every stage from eligibility verification through denial management and AR follow-up, not just claim submission. We also handle the credentialing and enrollment infrastructure that makes billing work in the first place.
Our approach treats RCM as a connected system. When we identify a denial pattern, we trace it back to its source, whether that’s a registration workflow, a coding issue, a payer policy change, or a credentialing gap, and we fix the upstream cause. Our billing team doesn’t just work the denial queue. We reduce it.
We also handle CAQH profile management, Medicare revalidation tracking, and payer credentialing across commercial plans. When a provider joins a practice, we start the enrollment process immediately so the gap between day one and first billable date is as short as possible. Our average onboarding time for new clients is 6 days.
Our numbers reflect a system that works end-to-end: 99% claim accuracy rate, 95% first-pass acceptance rate, 30% reduction in AR days, and an average 36-day collection cycle. These aren’t targets. They’re our operational standard.
Related: Payer Enrollment Services | Provider Credentialing | Payment Posting in Medical Billing
RCM Health Checklist for Medical Practices
- Patient registration collects insurance ID, group number, and MBI for Medicare patients
- Insurance eligibility verified before every visit using real-time 270/271 transactions
- Prior authorization workflow in place with a current payer requirement list
- Charge entry deadline of 24 hours or less per provider
- Claims scrubbed before submission and clean claim rate tracked monthly
- Payment posting completed within 48 hours of ERA receipt
- Denial management workflow with appeal deadlines tracked by payer
- Root cause analysis run monthly on top denial reason codes
- AR aging reviewed weekly with follow-up on balances over 30 days
- All provider Medicare enrollments and revalidation dates tracked in PECOS
Frequently Asked Questions: What Is RCM in Medical Billing
What is RCM in medical billing?
RCM in medical billing stands for Revenue Cycle Management. It is the end-to-end process healthcare practices use to track patient care from registration and insurance verification through charge capture, claim submission, payment posting, denial management, and AR follow-up. Every stage is connected. A failure at any point reduces what every step after it can collect. RCM is the full system that determines how much of what a practice earns it actually gets paid.
What are the main stages of RCM in medical billing?
The eight main stages are patient registration, insurance eligibility verification, prior authorization, charge capture and coding, claim submission and scrubbing, payment posting, denial management, and AR follow-up with patient collections. All eight must function correctly for the revenue cycle to close without revenue leakage. Most practices with billing problems have a failure concentrated in one or two of these stages.
What is the difference between medical billing and RCM?
Medical billing is one component of RCM. It covers coding, claim submission, and payment collection. RCM is the broader system that includes everything before billing, like registration and authorization, and everything after, like denial management and AR follow-up. Treating billing as separate from the rest of the cycle is precisely how most revenue leaks begin.
Why do practices lose money in the revenue cycle?
Practices lose money when RCM stages are disconnected. A registration error causes a denial. A missed eligibility check leads to a coverage dispute. A denial that goes unworked past 30 days misses the appeal window. RCM problems are almost always systemic rather than isolated. One step fails and the failure compounds through every step downstream. The revenue loss is rarely traceable to a single mistake; it’s the sum of many small workflow gaps.
What is a clean claim rate and why does it matter for RCM?
A clean claim rate is the percentage of claims paid on first submission without correction or appeal. The industry benchmark is 95% or higher. Practices below 90% are spending excessive staff time correcting and resubmitting claims that should have gone out right the first time. Each rework event costs $25 to $118. Clean claim rate is one of the most direct measures of overall RCM health.
What is accounts receivable in medical billing?
Accounts receivable is the total outstanding amount owed to a practice for services delivered but not yet collected. It’s tracked in aging buckets: 0-30, 31-60, 61-90, and 90-plus days. Healthy practices keep the bulk of AR in the 0-30 bucket. Balances past 90 days are at serious risk: only about 20% of AR in that bucket is typically recovered. Days in AR is the single most useful summary indicator of RCM performance.
What is denial management in RCM?
Denial management is the process of identifying why a claim was denied, correcting the error or filing an appeal, resubmitting the claim, and tracking it through to payment. Effective denial management also includes monthly root cause analysis to prevent recurring denial patterns. About 60% of denied claims are never reworked by practices. Each unworked denial is revenue permanently written off that a functional denial management workflow would have recovered.
What is prior authorization in the revenue cycle?
Prior authorization is payer approval obtained before a procedure is performed. Missing required authorizations results in automatic denials on the back end, regardless of medical necessity. It’s a front-end RCM function and one of the most common and most preventable denial causes. A practice without a current authorization requirement list and a workflow to obtain and document authorizations in advance will generate these denials on a recurring, predictable basis.
How does provider credentialing connect to RCM?
Credentialing directly affects RCM because a provider who isn’t enrolled with a payer cannot bill that payer. Claims submitted by non-enrolled providers deny automatically. Credentialing gaps, lapsed revalidations, and missing payer enrollments are RCM failures that happen before a single claim is ever submitted. They’re invisible until the denial arrives, and by then the lost revenue may span weeks or months of patient visits.
Should a practice outsource RCM or keep it in-house?
The honest answer depends on whether in-house staff have the capacity, tools, and training to manage all eight RCM stages correctly and consistently. Most practices that outsource RCM do so because the combined cost of staff, software, training, and compliance monitoring exceeds the cost of a billing partner. The performance argument for outsourcing is stronger than the cost argument: specialized RCM teams consistently outperform in-house billing on clean claim rate, denial rate, and days in AR.
What KPIs should practices track to measure RCM performance?
The five core RCM KPIs are clean claim rate (target 95% or higher), first-pass acceptance rate (target 95% or higher), days in AR (target under 40), denial rate (target under 5%), and net collection rate (target 95% or higher). Tracking all five gives a complete picture of revenue cycle health. If you only track one, make it days in AR. It reflects the combined effect of every upstream stage and tells you where to start investigating.
Related Resources from Qualigenix
- Payer Enrollment Services
- Provider Credentialing Services
- Payment Posting in Medical Billing
- CAQH Profile Management
- Healthcare Credentialing 2026
- Re-credentialing Services
- Telehealth Provider Credentialing
- Contact
Your RCM Should Be Collecting More Than It Is
Qualigenix manages the full revenue cycle for practices across 38+ specialties. From eligibility verification and prior authorization through denial management and AR follow-up, we close the gaps that cost practices money every day.
Our team delivers 99% claim accuracy, a 95% first-pass acceptance rate, an average 36-day collection cycle, and a 30% reduction in AR days. We onboard in as few as 6 days.
Precision. Progress. Qualigenix.
What’s Next

Medical Coding Errors That Cost Practices the Most (And How to Catch Them Before They Submit)
Medical Coding Errors That Cost Practices the Most (And How to Catch Them Before They Submit) Written by the...
What Is Insurance Verification and Why It Matters
Insurance verification is the front-end process that determines whether a claim will be paid before the patient ever enters...

Insurance Denial Appeals: What Practices Miss
Most insurance denial appeals that fail don’t fail because the clinical case was weak. They fail because the...