Outsource Medical Coding: How to Choose the Right Partner
The Qualigenix Editorial Team consists of certified billing and coding experts with over 40 years of experience across 38+ medical specialties. Our content is rigorously researched against CMS, AMA, and payer-specific guidelines to ensure total compliance and accuracy. We apply the same elite standards to our resources as we do our client work, consistently delivering high claim accuracy and significant reductions in AR days.
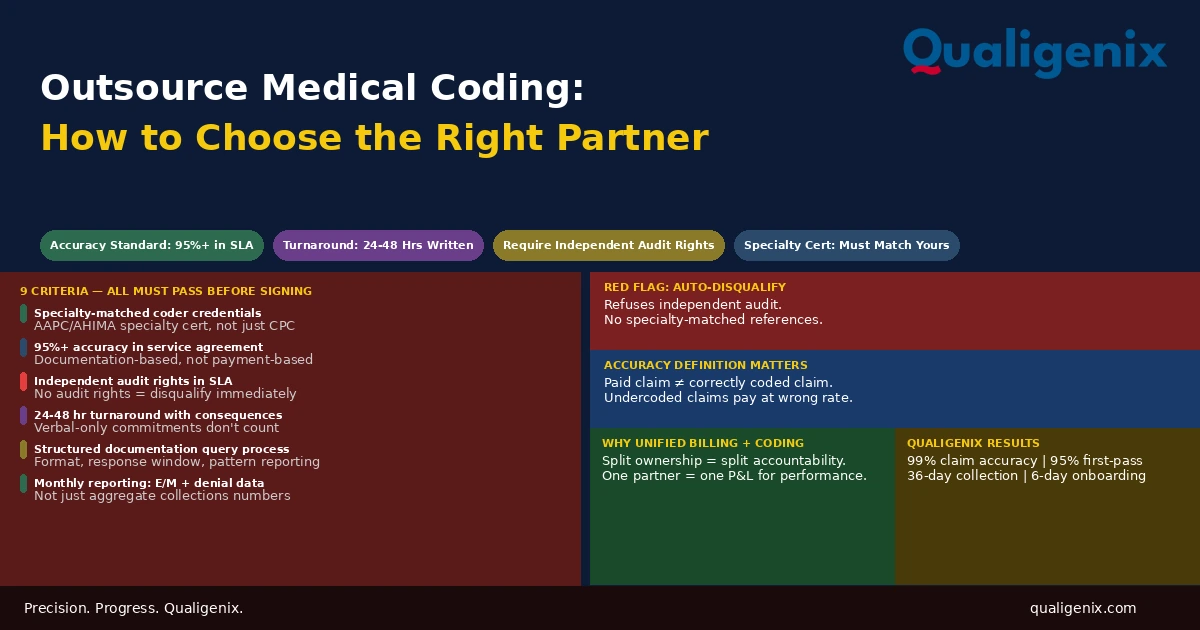
Selecting an outsourced medical coding partner is not a procurement decision. It is a multi-year revenue cycle commitment whose quality compounds in both directions correctly coded claims pay at the right rate, day after day, year after year; systematically undercoded or miscoded claims reduce collections by amounts that accumulate well beyond what a lower vendor fee saves. The evaluation criteria that matter are specific: specialty-matched coder credentials, a contractually defined and independently auditable accuracy rate, a turnaround commitment with teeth, a structured documentation query process, and monthly reporting that lets the practice verify performance rather than trust it. Partners who can’t meet all of these criteria should not receive a long-term coding contract regardless of what their demo looks like.
The pitch for outsourced medical coding is always some version of the same promise: lower cost, better accuracy, faster turnaround. Most vendors can make this pitch. The credible ones can prove it. The distinction between them matters enormously because the difference between a coding partner who delivers 95% accuracy and one who delivers 88% accuracy on a practice generating $4 million in annual charges is not a minor service quality gap. It is a revenue difference that accumulates to hundreds of thousands of dollars over the life of the contract.
The evaluation process that most practices apply to outsourced coding vendors is insufficient to distinguish between these two outcomes. A polished demo of a billing dashboard, a sales rep with good specialty knowledge, and a price point 10% below the nearest competitor do not predict coding accuracy. They predict a good sales process. The only thing that predicts coding accuracy is documented accuracy performance, specialty-matched credentials, a robust quality control process, and the contractual willingness to be independently audited.
This blog covers what a rigorous coding partner evaluation looks like: what to require in credentials, what to define contractually, what to measure from day one, and what red flags disqualify a vendor before the conversation reaches pricing.
Choosing an outsourced medical coding partner requires evaluating six specific criteria: specialty-matched coder credentials for your encounter mix, a contractually defined coding accuracy rate of 95% or higher with independent audit rights, a turnaround commitment of 24 to 48 hours written into the service agreement, a structured documentation query process with defined physician response windows, monthly performance reporting including E/M code distribution and denial root cause data, and HIPAA compliance documentation with a signed BAA. Partners who cannot meet all six should not receive a long-term coding contract.
Outsourced Coding Partner Evaluation: Key Standards
| Evaluation Criterion | Minimum Standard | Disqualifying Response |
|---|---|---|
| Coding accuracy rate | 95% or higher, contractually defined | Claimed without measurement methodology |
| Independent audit right | Granted in service agreement | Refused or limited to vendor-conducted audits only |
| Coding turnaround commitment | 24 to 48 hours, written into SLA | Quoted verbally only or exceeds 48 hours |
| Specialty coder credentials | AAPC or AHIMA specialty cert for your encounter mix | General CPC only for complex specialty encounters |
| Documentation query process | Defined workflow with physician response standard | Ad hoc or informal — no defined process |
| Monthly reporting package | E/M distribution, denial root cause, turnaround data | Aggregate collections metrics only |
| HIPAA compliance | BAA signed before data transmission begins | Verbal assurance without documentation |
| Specialty-matched client references | Current clients at similar specialty and volume | References only from different specialties |
| Code update training process | Annual CPT/ICD-10 update training before January | No defined training schedule or documentation |
| Integrated billing option | Coding and billing managed by same partner | Coding only with no billing integration available |
Criterion 1: Specialty-Matched Coder Credentials
The first and most fundamental evaluation criterion is whether the coders who will be assigned to the practice’s encounters hold credentials that match the specialty complexity of those encounters. This is not a bureaucratic requirement. It is a quality prerequisite. Medical coding in specialty settings involves specialty-specific rules, procedure documentation patterns, and code set distinctions that general coding training does not fully cover.
The American Academy of Professional Coders (AAPC) and the American Health Information Management Association (AHIMA) both offer specialty-specific certifications in addition to their general coding credentials. AAPC specialty certifications include the Certified Cardiovascular and Thoracic Coder (CCTC), Certified Orthopedic Surgery Coder (COSC), Certified Oncology Coder (COC), Certified Rheumatology Coder (CRC), and many others. Each requires a specialty knowledge examination beyond the general CPC.
When evaluating a vendor, ask specifically: what certification does the coder assigned to my encounters hold, and is that certification in my specialty? The answer “our coders are all CPCs” is not sufficient for a specialty practice. A general CPC credential validates baseline coding competency. It does not validate the specific knowledge required to code complex orthopedic surgical procedures, oncology drug administration, or interventional cardiology encounters accurately. A vendor that cannot assign specialty-certified coders to specialty practices is structurally set up to produce lower accuracy on the most complex and highest-value encounters.
The credential question also applies to the depth of the coder pool the vendor can access. A vendor with one cardiology-certified coder can cover your cardiology practice until that coder goes on leave, takes a different assignment, or leaves the company. Ask about backup coverage: when your assigned specialty coder is unavailable, who covers the account and what are their credentials? A vendor with no backup specialty coverage is a staffing vulnerability that will manifest as turnaround delays and accuracy degradation when coverage gaps occur.
Criterion 2: Contractually Defined Accuracy with Independent Audit Rights
Every outsourced coding vendor claims high accuracy. The relevant question is not what they claim but how they define accuracy, how they measure it, and whether the measurement can be independently verified.
Defining Coding Accuracy
Coding accuracy should be defined in the service agreement as the percentage of coded encounters where all of the following are correct when reviewed against the clinical documentation: the CPT procedure code or E/M level, the ICD-10 diagnosis code or codes, all modifiers, and the diagnosis-to-procedure linkage. An accuracy definition that measures only CPT accuracy without measuring ICD-10 specificity or modifier correctness is a narrower standard than the practice needs.
The minimum standard is 95%. This means that in any audit sample of 100 coded encounters, no more than five should contain errors in any of the components above. A vendor who proposes an 90% accuracy floor is proposing a standard that allows 10 errors per 100 encounters a level that will produce a measurable denial pattern and a measurable undercoding revenue loss over time.
Independent Audit Rights
The accuracy guarantee is only meaningful if the practice can verify it independently. A vendor who defines accuracy, measures it themselves, and reports the result to the practice without allowing independent verification is reporting a number without accountability. Independent audit rights the right to pull a random sample of coded encounters at any time and have them reviewed by a qualified coder not affiliated with the vendor are the mechanism that makes an accuracy guarantee credible.
Negotiating independent audit rights into the service agreement before signing is not a sign of distrust. It is a sign of operational maturity. A coding vendor who is genuinely achieving 95% or higher accuracy on the practice’s encounter types will welcome independent audit because it validates the performance they are claiming. A vendor who resists independent audit is protecting a number they know cannot withstand outside scrutiny.
Warning: Some outsourced coding vendors define “accuracy” as the percentage of claims that were paid by payers, not the percentage of claims that were coded correctly. These are not the same measure. A claim coded at 99213 when the documentation supports 99214 will be paid by the payer at the 99213 rate. The payment was not rejected. The accuracy, by that vendor’s definition, was 100%. The actual coding accuracy was below standard, and the practice lost the revenue difference on every such claim. Confirm that the accuracy definition in any service agreement is documentation-based, not payment-based.
Criterion 3: Turnaround Time Commitment in the Service Agreement
Coding turnaround time is the elapsed duration from when complete clinical documentation is available for coding to when the coded encounter is returned and ready for claim submission. Every day of delay advances the claim toward the timely filing window without submitting it and introduces memory-based coding risk if the coder is working from documentation that is no longer fresh relative to the encounter.
The standard for outsourced coding is 24 to 48 hours from documentation receipt. High-volume practices should expect same-day or next-business-day turnaround. This commitment must be written into the service level agreement, not mentioned verbally during the sales process and forgotten after signing.
The service agreement should also define what “documentation receipt” means: the timestamp at which the complete documentation package is available in the vendor’s coding system. If the practice’s documentation workflow creates delays in transmitting notes — physicians completing notes two days after the encounter, a batch transfer process that runs weekly rather than daily — the 24-to-48-hour clock doesn’t start until complete documentation is in hand. Separating the vendor’s turnaround responsibility from the practice’s documentation completion responsibility is important for accurate performance measurement.
Also define what happens when the turnaround commitment is consistently missed. A service agreement that states a 48-hour turnaround standard but has no consequence for missing it consistently is not an enforceable standard. It is an aspiration. Performance penalties for systematic turnaround failures service credits, right to terminate without penalty, required remediation plans create accountability that informal commitments do not.
Criterion 4: Structured Documentation Query Process
When clinical documentation is insufficient to support an accurate code assignment, the coder has two choices: code conservatively to what is documented, or query the physician for clarification. In a well-run outsourced coding engagement, the query process is the mechanism through which coding accuracy is maintained and documentation quality is improved over time.
A structured query process includes four components that distinguish it from ad hoc coder-to-physician communication:
A defined submission format. Queries should be submitted through a structured form or portal that identifies the specific encounter, the coding question, and the documentation gap that prompted it. An informal message or a phone call is not a query process. It is an informal conversation that creates no audit trail and produces no pattern data.
A required physician response window. Physicians must respond to queries within a defined period 24 to 48 hours is standard or the encounter is coded conservatively to what is documented and flagged for physician review. A query process without a response window standard is a process that creates delays without accountability.
A consequence for non-response. When a physician does not respond within the window, the coder codes to what is documented and the encounter is finalized. The query is recorded as unresolved. The practice leadership receives a report of unresolved queries that identifies documentation gaps by physician and by encounter type.
A pattern reporting function. Monthly reporting of query volume, query resolution rate, and query categories by physician gives practice leadership visibility into which physicians generate the most documentation gaps and what those gaps consistently are. This data drives documentation improvement over time if it reaches the physicians in a usable format with specific feedback on what documentation elements would have avoided the query.
Criterion 5: Monthly Reporting Package That Verifies Performance
An outsourced coding partner’s monthly reporting should give the practice independent visibility into whether coding quality is actually performing at the contracted standard. Reporting that only shows claims submitted and collections received is billing reporting, not coding quality reporting. The practice needs to see the coding-specific metrics that indicate whether the partner is delivering what they promised.
The monthly coding reporting package should include at minimum:
| Report | What It Shows | Why It Matters |
|---|---|---|
| E/M code distribution per physician vs. benchmark | Whether code levels track specialty peers | Surfaces undercoding that has no denial signal |
| Coding turnaround average and range | Whether turnaround commitment is being met | Identifies charge lag risk before it becomes a filing issue |
| Query volume and resolution rate per physician | Documentation gap patterns by provider | Identifies physicians who need documentation feedback |
| Coding-related denial root cause breakdown | Denial categories attributable to coding vs. billing | Confirms coding quality is not producing systematic denials |
| Accuracy audit results (if quarterly audit conducted) | Independent or internal audit findings | Verifies that contracted accuracy rate is being achieved |
| New and deleted code compliance for current year | Whether January code updates were applied correctly | Confirms annual code set transitions were handled properly |
A vendor who responds to reporting requests with “we’ll set up a call to review your collections” is providing billing performance reporting, not coding quality reporting. These are different data sets. Insist on coding-specific metrics from the proposal stage so the expectation is established before the contract is signed.
Criterion 6: HIPAA Compliance Documentation
Clinical documentation contains protected health information. Every entity that receives, processes, or stores PHI on behalf of a covered entity is a HIPAA business associate and must operate under a signed Business Associate Agreement. This is not optional, and it is not satisfied by a vendor’s verbal assurance that they take HIPAA seriously.
Before transmitting any clinical documentation to an outsourced coding partner, confirm three things. First, a BAA has been signed by an authorized representative of both organizations and is on file. Second, the partner can produce their HIPAA security documentation their Privacy and Security policies, their workforce training records, their breach notification procedures. Third, if the partner is a cloud-based platform or processes data through third-party systems, the security architecture of those systems is covered by their BAA and their security documentation.
For partners with offshore coding components, additional due diligence applies. HIPAA’s business associate requirements extend to offshore partners, but enforcement mechanisms are more limited, and the security controls that are standard in US healthcare IT environments may not be uniformly present in offshore facilities. Practices transmitting PHI to offshore coding teams should request specific documentation of the security controls at those facilities, not a general assurance that the partner’s overall HIPAA compliance covers offshore operations.
Criterion 7: Specialty-Matched Reference Clients
A coding vendor’s track record with clients in a different specialty provides limited information about how they will perform in your specialty. A vendor with strong performance in primary care billing is not necessarily strong in orthopedic surgical coding. A vendor with excellent oncology coding results has not demonstrated their capability in behavioral health coding.
Request references from current clients who are in the same specialty and at a similar practice size. Ask those references specifically: what is the vendor’s actual coding turnaround performance (not claimed), what does the monthly reporting show about code distribution relative to benchmarks, have there been any periods where coding quality dropped and how was it handled, and what does the documentation query process look like in practice versus how it was described in the sales process.
The reference call is one of the most underutilized evaluation steps in vendor selection. A vendor who cannot provide two or three current specialty-matched references — or who provides references that seem coached or reluctant to provide specific detail, it is telling the practice something important about the depth of their proven track record in that specialty.
Criterion 8: Annual Code Update Process
CPT codes are updated by the AMA annually with changes effective January 1. ICD-10-CM codes are updated by CMS twice per year. Each update includes new codes, deleted codes, and revised code descriptions. Outsourced coding partners must incorporate these updates before they take effect — not after the practice notices that claims are denying for invalid codes in February.
Ask specifically: what is the vendor’s process for incorporating annual CPT updates? When are coders trained on the new code set? Is training completed before January 1 or after? Is there a documented process for catching encounters coded with deleted or outdated codes after the transition date? How are mid-year ICD-10 updates handled?
A vendor who describes their code update process as “we receive the updates and train our coders on them” without specifying when training is completed and how compliance is verified is describing an undocumented process. An undocumented process is a process that may or may not happen on schedule, depending on whoever is responsible for it that year. Practices have received coding from vendors who were still using deleted CPT codes in March because training was delayed and no one verified that the transition was complete before claims were submitted with the new year’s coding requirements.
Criterion 9: Integrated Billing Availability
The handoff between coding and billing is where errors accumulate most silently in revenue cycles where the two functions are managed separately. A coded encounter leaves the coding partner and enters the billing workflow. If the billing team doesn’t understand what the codes mean, applies the wrong place-of-service, forgets the authorization number, or submits without catching a payer-specific edit rule the scrubber should have caught, a correctly coded claim produces an incorrect or denied claim.
When both coding and billing are managed by the same partner, this handoff doesn’t exist. There is no gap between the coding output and the billing input. The same team that assigns the codes builds the claim, scrubs it, and submits it. When a denial arrives, the team that coded the claim also works the denial, which creates an accountability structure that identifies whether the denial originated in a coding decision or a billing workflow step.
A coding-only vendor creates a split-ownership structure where each function can attribute performance problems to the other. The billing team says the denials are from coding errors. The coding team says the claims were submitted without the right modifiers. Neither claim can be independently verified because each function’s output is only visible to the other after the fact. Single-partner accountability eliminates this attribution problem entirely.
Related: Medical Billing vs Coding: Key Differences
Red Flags That Should End the Conversation
Some vendor responses during the evaluation process are red flags that should disqualify the vendor regardless of how attractive their pricing or their demo appears. The revenue consequences of selecting the wrong coding partner are too significant to proceed past a disqualifying response on the hope that it will be different in practice.
Refusing to grant independent audit rights is the most significant red flag. There is no legitimate reason for a coding vendor to refuse independent auditing of their work. The only reason to refuse it is that the work cannot withstand independent scrutiny. A vendor who claims 96% accuracy and refuses to allow independent verification of that number is claiming a performance level they are not willing to defend.
Inability to provide specialty-matched client references is a close second. If a vendor has been providing coding services for two or more years and cannot produce two current clients in the same specialty willing to speak positively about the service, their track record in that specialty is insufficient to warrant a long-term coding contract.
No defined documentation query process. A coder who encounters a documentation gap and has no defined process for resolving it will either code conservatively without flagging the gap, or contact the physician informally without creating an audit trail. Both outcomes are worse than a defined query process. A vendor who has been providing coding services at any scale should have a defined query workflow. The absence of one indicates either that queries are not being raised at all (coders are coding conservatively without identifying improvement opportunities) or that queries are handled so informally that no one has documented the process.
Pricing significantly below market without explanation. Legitimate cost advantages in outsourced coding come from scale, workflow efficiency, or offshore labor. If a vendor is priced 30% to 40% below the market without a clear explanation, one of three things is likely: the accuracy delivered is proportionally lower, the coder credentials are proportionally weaker, or the service model depends on offshore labor without the quality oversight that offshore coding requires to produce domestic-equivalent accuracy.
How Qualigenix Approaches Outsourced Medical Coding
At Qualigenix, we meet every criterion in this evaluation framework because we designed our coding operation to be auditable, measurable, and accountable by default not as a negotiated concession to demanding clients.
Our coders hold specialty-specific credentials matched to the encounter types they code. We provide independent audit rights in every service agreement. We commit to 24-to-48-hour turnaround in writing. Our documentation query process is structured, tracked, and reported monthly. Our monthly reporting package includes E/M code distribution by physician, query volume and resolution rate, coding-related denial root cause data, and turnaround performance against the contractual commitment.
We also manage billing. Coding and billing at Qualigenix are integrated functions with unified accountability. The team that codes the encounter also submits the claim, posts the ERA, and works any denial that arrives. When a denial traces to a coding decision, the coder who made it is part of the resolution process. When it traces to a billing workflow step, the billing team owns it. The attribution is clear because the ownership is unified.
Our results reflect this integrated accountability: 99% claim accuracy rate, 95% first-pass acceptance rate, 36-day average collection cycle, and 30% reduction in AR days for practices transitioning to our platform. We onboard in as few as 6 days.
Related: Outpatient Coding Accuracy at Scale | What Is RCM in Medical Billing | What Is Physician Billing
Outsourced Coding Partner Evaluation Checklist
- Specialty coder credentials requested and verified for your specific encounter mix
- Backup coverage credentials confirmed for when assigned specialty coder is unavailable
- Coding accuracy rate defined in service agreement with measurement methodology specified
- Accuracy definition is documentation-based, not payment-based
- Independent audit rights granted in service agreement before signing
- Turnaround commitment of 24 to 48 hours written into SLA with defined consequences
- Documentation query workflow documented: format, physician response window, escalation process
- Monthly reporting package confirmed to include E/M distribution, query data, and denial root cause
- HIPAA BAA signed before any documentation is transmitted
- Security documentation reviewed: Privacy policy, Security policy, breach notification procedure
- Specialty-matched client references contacted and specific performance questions asked
- Annual CPT and ICD-10 update training process documented with completion timeline
- Independent accuracy audit conducted within first 90 days of engagement
- Integrated billing option evaluated and compared against split-vendor cost and risk
Frequently Asked Questions: Outsource Medical Coding Partner Selection
What should I look for when outsourcing medical coding?
Evaluate on six criteria: specialty-matched coder credentials, a contractually defined 95%+ accuracy rate with independent audit rights, a 24-to-48-hour turnaround commitment in the SLA, a structured documentation query process, monthly reporting including E/M distribution and denial root cause data, and a signed HIPAA BAA before data transmission. Partners who cannot meet all six should not receive a long-term coding contract. The revenue consequences of selecting a low-quality coding partner compound over the full contract term in ways that a lower fee cannot offset.
What coding accuracy rate should an outsourced partner guarantee?
The minimum contractual accuracy standard is 95%, measured as the percentage of coded encounters where CPT, ICD-10, modifiers, and diagnosis linkage are all correct when audited against clinical documentation. Confirm the definition is documentation-based, not payment-based — a claim that pays at a lower level because it was undercoded passes a payment-based accuracy test while failing a documentation-based one. The difference between those two definitions is the difference between a standard that protects revenue and one that merely avoids obvious denials.
How do I verify an outsourced coding partner’s claimed accuracy rate?
Request the measurement methodology: sample size, time period, who conducts the audit, and what elements are reviewed. Request specialty-specific accuracy data, not aggregate rates across all clients. Negotiate independent audit rights in the service agreement and conduct an independent audit of 15 to 20 encounters within the first 90 days. A partner who resists independent auditing is protecting a performance number that cannot withstand outside review. Confident vendors welcome independent audits because the results validate what they are claiming.
What is a documentation query process and why does it matter?
A documentation query process is the mechanism through which coders request physician clarification when documentation is insufficient for accurate coding. It matters because without it, documentation gaps are handled by coding conservatively with no record of what was missed and no feedback to the physician about what would have supported a higher code. A good query process — structured format, defined physician response window, pattern reporting — does two things simultaneously: maintains coding accuracy on individual encounters and drives documentation improvement over time through physician feedback.
What red flags should disqualify an outsourced coding partner?
The primary red flags are: refusing independent audit rights, inability to provide specialty-matched client references, no defined documentation query process, accuracy claims without measurement methodology, turnaround commitments beyond 48 hours, and pricing significantly below market without a clear explanation. Any one of these individually warrants serious concern. Multiple red flags together indicate a vendor whose performance cannot be verified and whose service quality is likely to disappoint in the ways that matter most for revenue: coding accuracy, turnaround reliability, and documentation feedback.
Is it better to outsource coding and billing to the same partner?
Yes. A single partner managing both coding and billing is accountable for the full claim lifecycle, which eliminates the handoff gap where coding output errors become billing problems and each vendor attributes performance issues to the other. Split ownership of coding and billing creates an attribution problem that is difficult to resolve and tends to persist because neither vendor has full visibility into the other’s function. Unified ownership creates unified accountability — when a denial arrives, the same team that coded the encounter also submits it and works the denial, which makes root cause identification and correction straightforward.
Related Resources from Qualigenix
- Medical Billing vs Coding: Key Differences
- Inpatient Coding for Physicians
- What Is RCM in Medical Billing
- Provider Credentialing Services
- AAPC Certified Professional Coder (AAPC.com)
We Meet Every Criterion on This List. Ask Us to Prove It.
Qualigenix provides outsourced medical coding for specialty practices across 38+ specialties, paired with integrated billing management. Specialty-certified coders. Contractual accuracy standards. Independent audit rights. Monthly performance reporting. We welcome the audit.
Our team delivers 99% claim accuracy, a 95% first-pass acceptance rate, an average 36-day collection cycle, and a 30% reduction in AR days. We onboard in as few as 6 days.
Precision. Progress. Qualigenix.
What’s Next

Medical Coding Errors That Cost Practices the Most (And How to Catch Them Before They Submit)
Medical Coding Errors That Cost Practices the Most (And How to Catch Them Before They Submit) Written by the...
What Is Insurance Verification and Why It Matters
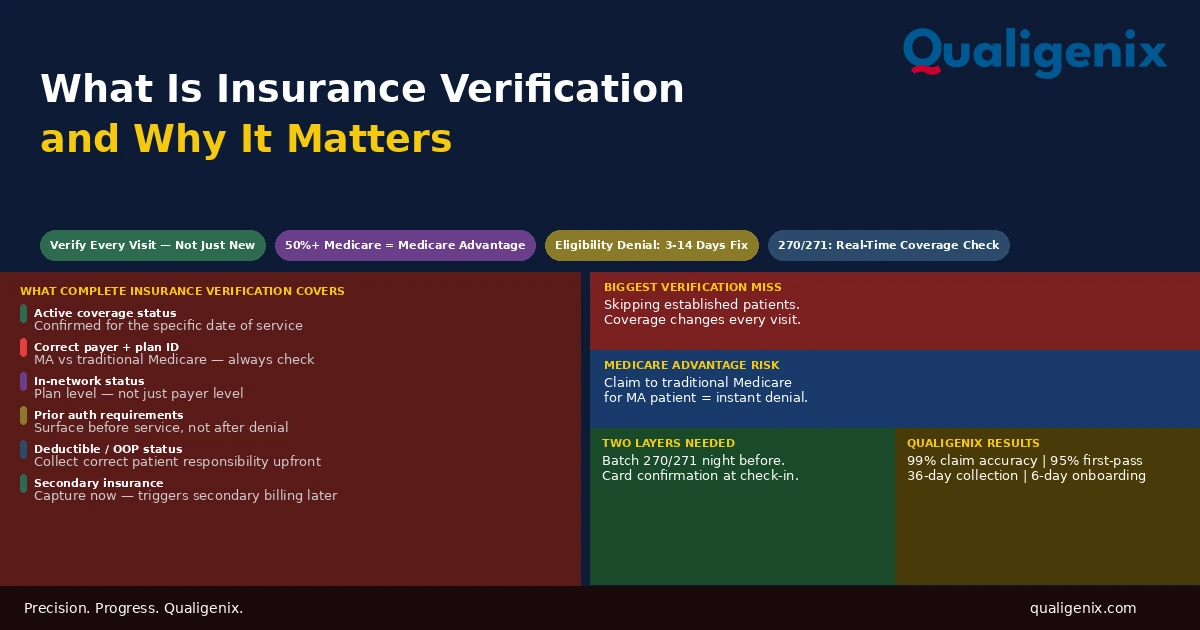
Insurance verification is the front-end process that determines whether a claim will be paid before the patient ever enters...

Insurance Denial Appeals: What Practices Miss
Most insurance denial appeals that fail don’t fail because the clinical case was weak. They fail because the...