Drug Prior Authorization Explained: What Every Provider Needs to Know Before Prescribing
The Qualigenix Editorial Team consists of certified billing and coding experts with over 40 years of experience across 38+ medical specialties. Our content is rigorously researched against CMS, AMA, and payer-specific guidelines to ensure total compliance and accuracy. We apply the same elite standards to our resources as we do our client work, consistently delivering high claim accuracy and significant reductions in AR days.

Drug prior authorization is the payer approval step that sits between a physician’s prescription and a patient’s access to medication. When it’s required and not obtained before dispensing, the payer won’t cover the drug. When it’s submitted incomplete, it denies. When it’s approved but the PA number isn’t on the claim, the claim denies. Every one of these failures is preventable. All of them require knowing how the process works before writing the prescription.
From the physician’s perspective, the prescription ends the clinical decision. The right drug for the right patient at the right dose. From the patient’s perspective, the prescription begins the access problem. Because between the prescription pad and the pharmacy counter, there is often a payer decision that neither the physician nor the patient controls directly but both must navigate.
Drug prior authorization is that decision. A payer’s requirement that clinical justification be reviewed and approved before a specific medication is dispensed or reimbursed. It applies to a growing number of drugs across every specialty and every payer. It takes time. It requires documentation. And when the process isn’t managed correctly from the moment the drug is prescribed, it produces delays, denials, and patients who either can’t access their medication or pay for it themselves.
This blog explains what drug prior authorization is, how the approval process works from start to finish, which categories of drugs most commonly require it, what documentation payers actually expect, and how to prevent the denials that happen most often when the process isn’t treated as seriously as the clinical decision that preceded it.
Drug prior authorization is the process of obtaining payer approval before a medication is dispensed or covered. The payer reviews clinical documentation to confirm the drug meets their formulary requirements, medical necessity criteria, and coverage policies. Without an approved PA, the payer will not reimburse the medication. The PA request must include the patient’s diagnosis with ICD-10 codes, the prescribing provider’s NPI, step therapy documentation, and a clinical justification that addresses the payer’s specific criteria for that drug.
Drug Prior Authorization: Key Numbers Every Practice Needs
| Metric | Data Point | Source |
|---|---|---|
| Average PA requests per physician per week | 45 across all service types | AMA prior authorization survey |
| Physicians reporting PA causes care delays | 94% of surveyed physicians | AMA prior authorization survey 2024 |
| Patients who abandon treatment due to PA delays | Up to 27% | AMA patient impact data |
| Drug PA denial rate across all medication types | 10% to 15% of requests | Payer utilization management data |
| Specialty drug PA denial rate | 25% to 40% of requests | Specialty PA processing benchmarks |
| CMS 2026 standard PA response time requirement | 7 calendar days | CMS prior authorization final rule |
| CMS 2026 urgent PA response time requirement | 72 hours | CMS prior authorization final rule |
| PA denials overturned after peer-to-peer review | Up to 75% | AMA PA reversal data |
| Physicians with 13+ staff hours per week on PA | 35% of surveyed physicians | AMA prior authorization survey 2024 |
| Practices reporting serious adverse events from PA delays | 25% of surveyed physicians | AMA prior authorization impact data |
| Qualigenix first-pass acceptance rate | 95% | Qualigenix performance data |
| Qualigenix claim accuracy rate | 99% | Qualigenix performance data |
| Qualigenix average collection cycle | 36 days | Qualigenix performance data |
| Qualigenix client onboarding time | 6 days | Qualigenix operations data |
What Drug Prior Authorization Actually Is
Drug prior authorization is a utilization management mechanism used by insurance payers to review whether a prescribed medication meets their criteria for coverage before it is dispensed. The payer is not reviewing whether the drug is safe or effective. The FDA handles that. The payer is reviewing whether the drug is the appropriate choice given the patient’s specific situation, their diagnosis, their treatment history, and the payer’s coverage policies for that drug.
The practical effect is that a drug requiring PA cannot be filled at a pharmacy, administered in a clinic, or reimbursed on a claim until the payer has reviewed and approved the request. If the patient or pharmacy proceeds without authorization, the payer denies coverage. The patient pays out of pocket or the drug goes unaccessed entirely.
Drug prior authorization is not optional for drugs that require it, and it is not a formality. It is a payer-controlled gate that will not open unless the required clinical information is submitted in the required format and found to meet the payer’s medical necessity criteria. The clinical strength of the prescription does not override the administrative requirement to go through the gate.
The number of drugs requiring PA has grown consistently over the past decade. Payers have expanded their PA requirements to include not just specialty biologics and high-cost agents but also brand-name medications with available generics, GLP-1 agonists for weight management, certain anticoagulants, controlled substances, and many drugs where the payer has a preferred formulary alternative. The administrative burden has grown proportionally. According to AMA surveys, physicians and their staff now spend an average of 13 or more hours per week managing prior authorization requests of all types, with drug PA representing a significant share.
Why Payers Require Drug Prior Authorization
Understanding why payers require drug prior authorization matters because it shapes how to structure the documentation that gets requests approved. Payers have four main reasons for requiring PA, and each one maps to a specific documentation need.
Formulary Compliance
Every payer maintains a formulary: a list of covered drugs organized into tiers that determine cost-sharing levels. When a physician prescribes a drug that sits on a higher formulary tier or requires review before coverage is confirmed, PA is the mechanism the payer uses to verify the prescription is appropriate. Drugs on the lowest formulary tiers typically don’t require PA. Drugs on higher tiers, or non-formulary drugs, almost always do.
Step Therapy Enforcement
Payers require step therapy to ensure patients try lower-cost alternatives before accessing more expensive options. PA is how payers enforce this requirement. A physician who prescribes a biologic for a condition that the payer’s step therapy protocol requires treating first with conventional drugs must document that the step therapy sequence was followed, failed, or is contraindicated. Without that documentation, the PA request doesn’t meet the criteria and denies.
Medical Necessity Confirmation
Payers apply medical necessity criteria to specific drugs to confirm the prescribed medication is appropriate for the patient’s documented condition. This isn’t a judgment about clinical expertise. It’s a confirmation that the drug is being used for an indication the payer covers, at an appropriate dose, for a patient whose diagnosis supports the use. A prescription for a drug that treats a condition not reflected in the patient’s submitted diagnosis codes will fail medical necessity review.
Cost Management
For high-cost medications, PA is explicitly a cost management function. Biologics costing $3,000 to $10,000 per month, oncology agents, gene therapies, and other premium-priced drugs receive the most intensive PA scrutiny because they represent the largest potential cost exposure for the payer. The documentation requirements are most demanding for these drugs, which is why specialty drug PA denial rates of 25% to 40% are so much higher than the 10% to 15% seen across all drug types.
Which Drugs Most Commonly Require Prior Authorization
PA requirements vary by payer, plan, and formulary. There is no universal list. But patterns exist across most commercial payers and government programs that allow practices to anticipate which prescriptions will trigger the PA process.
| Drug Category | Why PA Is Required | Common Documentation Needed |
|---|---|---|
| Biologics and specialty drugs | High cost, complex clinical criteria, step therapy | Diagnosis, disease activity scores, prior therapy failure |
| Brand-name drugs with generics | Formulary alternative exists at lower tier | Clinical justification for brand over generic |
| GLP-1 agonists (weight management) | High cost, diagnosis-specific criteria | BMI documentation, comorbidities, prior weight loss attempts |
| Controlled substances (Schedule II-III) | Abuse potential, quantity limit enforcement | Diagnosis, prior treatment, pain management plan |
| Anticoagulants (NOACs) | Cost differential vs. warfarin, indication review | Diagnosis, contraindication to alternatives |
| Growth hormones | High cost, strict diagnostic criteria | Growth data, lab results, specialist diagnosis |
| Oncology agents | High cost, biomarker requirements, line of therapy | Pathology, molecular testing, staging, NCCN guidelines |
| Sleep aids (non-benzodiazepine) | Step therapy with behavioral interventions | Sleep study or clinical diagnosis, prior treatment |
| Dermatologic agents (topical/systemic) | High-cost alternatives to standard topicals | Disease severity score, prior topical failure |
| ADHD medications | Diagnosis criteria, quantity limits | Diagnosis documentation, prescriber specialty |
The most important operational lesson from this list is that drug PA requirements change. Payers update formularies regularly, add new drugs to their PA lists, and modify criteria without always notifying practices directly. A drug that didn’t require PA last year may require it this year. The safest practice is to check every new prescription against the patient’s current formulary rather than relying on historical knowledge of what required PA previously.
The Drug Prior Authorization Process: Step by Step
Understanding what happens at each stage of the PA process explains where delays and denials originate. Most PA failures are not the result of an impossible standard. They result from gaps in documentation, errors in submission, or delays in response to payer requests that could have been avoided with better process management.
Step 1: Prescription and PA Trigger Identification
When a physician prescribes a medication, the pharmacy receiving the prescription runs it through the patient’s insurance to check for PA requirements. If PA is required, the pharmacy notifies the prescriber’s office. In practices with electronic prescribing and integrated PA workflows, this check can happen before the prescription leaves the practice. In practices without this integration, the pharmacy rejection is often the first indication that PA is needed.
The better approach is to check PA requirements at the point of prescribing. Many practice management systems, electronic health records, and clearinghouses support real-time formulary and PA requirement checks. Using this capability converts a pharmacy rejection that delays the patient by days into a front-end flag that allows the practice to start the PA process immediately.
Warning: A pharmacy rejection for PA is not the same as a payer denial. It is a notification that PA is required before the drug can be dispensed. Practices that treat it as a denial and move to alternative medications without first checking whether the original drug can be authorized through PA are substituting clinical decisions for administrative process failures. The better response is to initiate the PA request immediately.
Step 2: Clinical Criteria Review
Before submitting the PA request, identify exactly what the payer requires for the specific drug. Every payer publishes clinical coverage criteria for drugs requiring PA, accessible through their provider portal or by calling provider services. These criteria specify the diagnosis codes required, the step therapy sequence, any lab values or clinical scores needed, and the medical necessity standard the request must meet.
This step is where most submission failures originate. Practices that skip the criteria review and submit based on what they believe the payer will accept are submitting blind. The payer’s criteria may require specific documentation elements the practice hasn’t collected. Finding this out after a denial adds 5 to 10 business days to the patient’s treatment timeline.
Step 3: Documentation Assembly
Once the criteria are known, assemble every piece of documentation the payer requires. This typically includes the patient’s confirmed diagnosis with supporting chart notes, the relevant ICD-10 codes, any required lab results, step therapy documentation showing prior medications tried with doses, durations, and outcomes, and a clinical justification statement or letter from the prescribing physician.
The step therapy documentation deserves special attention because it is the most common single point of failure in drug PA submissions across all drug categories, not just specialty medications. Documentation of step therapy must be explicit. It must name each prior drug, the dose, how long the patient took it, and specifically what happened: inadequate response after the full trial period, intolerable adverse effect with clinical documentation, contraindication based on the patient’s comorbidities. General statements that the patient failed prior therapy are routinely rejected by payer reviewers as insufficient.
Step 4: Request Submission
Drug PA requests are submitted through the payer’s preferred channel. Increasingly, this is an electronic portal. The CMS 2026 electronic PA rule requires Medicare Advantage, Medicaid managed care, and ACA marketplace plans to support electronic PA through FHIR-based APIs, which means electronic submission is becoming the standard across most plan types. Electronic submission is faster than fax or phone, produces a confirmation of receipt, and typically routes to review faster than paper processes.
The submission must include the prescribing provider’s NPI, the patient’s member ID, the drug name, strength, dose form, quantity, and days supply, and all required clinical documentation. Missing any of these fields causes the request to be returned as incomplete before clinical review even begins.
Step 5: Payer Review and Response
After submission, the payer’s clinical review team evaluates whether the request meets their criteria. For standard drug PA, the CMS 2026 rule requires a response within 7 calendar days. For urgent requests, 72 hours. Commercial payers not subject to the CMS rule vary. Many match these timelines. Some take longer for complex clinical reviews.
During this window, the payer may request additional clinical information. This is not a denial. It is an information request. Responding to it within 24 hours keeps the review moving. Delayed responses extend the timeline proportionally and may result in the payer closing the request as incomplete if the response window passes.
Step 6: Approval, Denial, or Appeal
The payer issues one of three responses: approved, denied, or pended for additional information. An approval comes with a PA number, an effective date, and an expiration date. All three must be documented and the PA number must appear on every claim submitted for the authorized drug during the authorization period.
A denial comes with a reason code. This is the starting point for the appeal, not the end of the road. The specific denial reason determines the appeal strategy. An appeal with the same documentation as the original submission almost never overturns a denial. An appeal that directly addresses the specific criterion the payer said wasn’t met, with new or better documentation, has a much higher success rate.
The PA Number: The Billing Connection Most Practices Miss
When a drug PA is approved, the payer assigns a unique prior authorization number. This number is the link between the clinical approval and the billing claim. It must be included on every pharmacy claim or medical claim submitted for the authorized drug during the authorization period.
A claim submitted without the PA number denies even if the authorization was legitimately obtained and is active. A claim submitted with an expired PA number denies. A claim submitted with a PA number that doesn’t match the drug, dose, or patient on the claim denies. None of these situations requires a new PA request. All of them require a corrected claim resubmission. But each one adds days or weeks to the payment timeline and requires staff time to identify and fix.
The PA number is not just a clinical record. It is a billing credential for every claim associated with the authorized drug. Practices that obtain PA approvals but don’t have a system for recording the number, its effective dates, and its expiration date are completing the hardest part of the process and then losing the benefit of it at claim submission.
What the CMS 2026 Electronic PA Rule Actually Changes
The CMS prior authorization final rule, which began phasing in for applicable payers in 2026, is the most significant federal action on prior authorization in years. It establishes enforceable response time standards, requires electronic PA functionality, mandates specific denial reasons, and requires payers to publicly report their PA metrics. For providers, the most immediately relevant changes are the response time requirements and the shift to electronic submission.
The 7-calendar-day standard for non-urgent requests and 72-hour standard for urgent requests apply to Medicare Advantage plans, Medicaid managed care organizations, Children’s Health Insurance Program plans, and ACA marketplace plans. For practices that previously dealt with payers taking 14 to 21 days to respond to standard drug PA requests, this represents a meaningful improvement in predictability.
What the rule does not change is the clinical documentation burden. The requirement for step therapy evidence, disease activity documentation, diagnosis code alignment, and clinical justification letters remains entirely the responsibility of the prescribing practice. Electronic PA tools make submission faster. They do not generate the clinical documentation that supports the request. That still requires clinical staff time and a documentation workflow aligned to each payer’s criteria.
Warning: Electronic PA does not mean automatic approval. A drug PA request submitted electronically with incomplete documentation will be denied electronically and just as fast. The speed of electronic PA accelerates both approvals and denials. Practices that interpret the shift to electronic PA as a simplification of the process rather than a change in the delivery mechanism will see faster denials on the same incomplete submissions that were previously getting slower denials through fax.
Appealing a Denied Drug Prior Authorization
A denied drug PA is not a final answer. It is the beginning of an appeal process, and that process has real overturn rates when executed correctly. The key is matching the appeal strategy to the specific reason for the denial.
Peer-to-Peer Review
The fastest and most effective appeal for most drug PA denials is a peer-to-peer review. This is a direct conversation between the prescribing physician and the payer’s medical reviewer. The prescribing physician presents the clinical case, addresses the denial reason, and provides additional clinical context that the written submission couldn’t convey. Peer-to-peer reviews overturn drug PA denials up to 75% of the time when the physician is prepared with the specific denial criteria and has additional clinical data to address it.
Most payers allow peer-to-peer review requests within 14 to 30 days of the denial. Missing this window converts the most effective appeal tool available into a missed opportunity. Every practice that receives drug PA denials should have a protocol for requesting peer-to-peer reviews immediately, not as a last resort after formal written appeals fail.
Formal Written Appeal
For denials where the peer-to-peer window has closed or where the denial reflects a coverage policy dispute rather than a clinical documentation gap, a formal written appeal is the next step. The appeal must directly address the denial reason with new documentation. An appeal letter that restates the original clinical justification without adding new information rarely succeeds. The appeal must show the payer reviewer something they didn’t see in the original request.
Expedited Review
When a drug PA denial creates an urgent clinical situation, an expedited review can be requested. Most payers must respond to expedited appeals within 72 hours under the CMS 2026 rule for applicable plan types. The request for expedited review must include clinical documentation of why the standard timeline creates a risk to the patient’s health.
How Credentialing Connects to Drug Prior Authorization
Drug PA requests are submitted under the prescribing provider’s NPI. If that provider is not enrolled with the patient’s payer, the PA request is rejected before clinical review. The payer cannot verify the prescriber’s network status, and a PA request from an unrecognized provider ID is treated as invalid.
This creates a specific and recurring problem in practices that add new providers. A physician joins the practice and begins seeing patients and writing prescriptions before their commercial payer credentialing is complete. The pharmacy or the practice submits PA requests under that physician’s NPI. The payers where enrollment is still pending reject the requests. Patients wait. Medications get delayed. The credentialing gap created a patient access problem that looks, from the practice’s perspective, like a PA problem.
The solution is the same one that applies to all credentialing gaps: start the enrollment process the day a hire is confirmed, not the day a provider walks in the door. Commercial payer credentialing takes 90 to 120 days. Any PA request submitted under a non-enrolled provider during that window will fail.
Related: Provider Credentialing Services | Payer Enrollment Services | Prior Auth for Medication in Specialty Practices
Building a Drug PA Workflow That Prevents Avoidable Denials
The practices that manage drug prior authorization most effectively treat it as a workflow function built into the prescribing process, not a billing reaction triggered by a pharmacy rejection. Here is what that workflow looks like in practice.
PA Check at Point of Prescribing
Use your EHR or practice management system to check formulary and PA requirements before the prescription is written. Electronic prescribing with real-time benefit check (RTBC) capabilities show PA requirements at the time of prescribing. Knowing before the prescription leaves the practice that PA is required allows the process to start the same day.
Criteria-Specific Documentation Templates
For the drugs your practice prescribes most frequently that require PA, build documentation templates that prompt collection of every element the relevant payers require. A template for biologic PA in a rheumatology practice looks different from a template for GLP-1 PA in a primary care setting. Both are more effective than submitting general chart notes and hoping the payer finds what they need.
Centralized PA Tracking
Maintain a tracker that shows every active PA by patient, including the drug, the payer, the PA number, the approval date, the expiration date, and the renewal trigger date. Any PA approaching expiration requires a renewal submission. Any PA number must be referenced on every claim for the authorized drug. A tracker makes both visible before they become billing problems.
Escalation Protocol for Denials
Every drug PA denial should trigger an immediate review to determine whether the denial reason is addressable through peer-to-peer review within the payer’s allowed window. Assign this determination as a required step, not an optional follow-up. The cost of the peer-to-peer review is 20 to 30 minutes of physician time. The cost of an uncontested denial is the full value of the denied medication coverage plus the clinical impact on the patient.
How Qualigenix Supports Drug Prior Authorization
At Qualigenix, we manage the credentialing and enrollment infrastructure that makes every drug PA request submitted by your providers valid from the start. A PA request submitted under a non-enrolled provider fails before a reviewer sees it. We ensure that doesn’t happen by starting provider enrollment the day a hire is confirmed, managing CAQH profiles across all providers, and tracking enrollment status across every payer in your network.
We also manage the full billing cycle that follows PA approval. When a specialty drug is authorized and administered or dispensed, the claim must include the PA number, the correct diagnosis codes, and the right billing modifiers. Our 99% claim accuracy rate reflects a billing process that handles these requirements correctly at first submission, protecting the revenue that the practice’s PA effort made possible.
Across 38+ specialties, we see how PA connects to every other part of the revenue cycle. An unapproved PA leads to a denied claim. A denied claim goes into the denial management queue. A denial that sits past the appeal window becomes an unrecoverable write-off. Fixing the process at the PA stage prevents the cascade. That’s where we help practices close the loop.
Related: What Is RCM in Medical Billing | CAQH Profile Management
Drug Prior Authorization Readiness Checklist
- PA requirement checked against patient’s current formulary before every prescription is written
- Payer-specific PA clinical criteria reviewed for every drug requiring authorization
- Step therapy documentation explicitly names each prior drug, dose, duration, and outcome
- ICD-10 diagnosis codes align with the drug’s covered indication per payer criteria
- Relevant lab results and clinical measures collected before submission
- PA request submitted electronically with all required fields and documentation attached
- PA status followed up every 1 to 2 business days until decision received
- Additional information requests responded to within 24 hours
- PA number, effective date, and expiration date recorded in patient record and PA tracker
- PA number included on every claim for the authorized drug
- Peer-to-peer review requested within payer window immediately on any denial
- Renewal submissions initiated 30 days before each PA expiration
- Prescribing provider confirmed enrolled with patient’s payer before PA submission
Frequently Asked Questions: Drug Prior Authorization
What is drug prior authorization?
Drug prior authorization is the process of obtaining payer approval before a medication is dispensed or covered. The payer reviews clinical documentation to confirm the drug meets their formulary requirements, medical necessity criteria, and coverage policies. Without approval, the payer will not reimburse the medication. The process requires clinical justification, diagnosis documentation, step therapy history, and a submission under the prescribing provider’s enrolled NPI.
Why do payers require prior authorization for drugs?
Payers require drug PA to enforce formulary compliance, manage costs for high-priced medications, ensure step therapy is followed, and confirm the prescribed drug is appropriate for the patient’s documented diagnosis. Each of these reasons maps to a specific documentation requirement in the PA request. Understanding which reason applies to a specific drug tells the practice exactly what documentation the payer needs to see.
How long does drug prior authorization take?
Under CMS 2026 rules, standard drug PA requires a payer response within 7 calendar days and urgent requests within 72 hours for applicable plan types. Standard drug PA often resolves in 1 to 3 business days for complete submissions. Specialty drug PA takes 5 to 14 business days due to clinical review requirements. Incomplete submissions extend every timeline. Starting the PA process before the prescription is written rather than after a pharmacy rejection removes the most common source of patient-facing delay.
What happens if a drug is dispensed without prior authorization?
If a drug requiring PA is dispensed without an approved authorization, the payer will deny coverage and the patient bears the full cost. Retroactive PA approval is possible in limited circumstances but not standard practice at most payers. For urgent or emergent situations, some payers allow a short supply of medication while PA is being processed. Dispensing without PA is not a practice workaround. It transfers the financial burden to the patient and damages trust in the practice’s ability to manage their insurance access.
What information is needed to request drug prior authorization?
A drug PA request requires the patient’s name, date of birth, and insurance ID, the prescribing provider’s NPI, the drug name, strength, dose, and days supply, ICD-10 diagnosis codes, step therapy documentation, relevant labs or clinical measures, and a clinical justification for the medication. Missing any field delays processing. Missing step therapy documentation on drugs that require it produces an automatic denial. Knowing the payer’s specific criteria before assembling the submission prevents the most common documentation gaps.
What is step therapy in drug prior authorization?
Step therapy requires documentation that the patient tried and failed one or more lower-cost alternatives before the requested drug will be authorized. Documentation must name each prior drug, the dose, the duration of the trial, and the specific outcome that makes the step therapy progression medically necessary. Statements that a patient failed prior therapy without these specifics are treated as incomplete and denied. Step therapy documentation failure is the leading cause of drug PA denials across all drug categories.
Can drug prior authorization be appealed if denied?
Yes. A denied drug PA can be appealed through peer-to-peer review, formal written appeal, or expedited review for urgent situations. Peer-to-peer review is the fastest and most effective option, overturning denials up to 75% of the time when the prescribing physician is prepared with the specific denial reason and additional clinical context. Most payers allow peer-to-peer requests within 14 to 30 days of the denial notice. Missing that window eliminates the most effective appeal option available.
What is the CMS 2026 electronic prior authorization rule?
The CMS 2026 electronic PA rule requires applicable payers to implement FHIR-based electronic PA, respond to standard requests within 7 calendar days, respond to urgent requests within 72 hours, and provide specific denial reasons. It applies to Medicare Advantage, Medicaid managed care, and ACA marketplace plans. The rule improves PA turnaround and transparency but does not reduce the clinical documentation burden on prescribing practices. Electronic submission is faster. The documentation requirements remain the same.
What is a prior authorization number and why does it matter for billing?
A PA number is the payer-assigned identifier confirming an authorization is active. It must appear on every pharmacy or medical claim for the authorized drug during the authorization period. A claim submitted without the PA number, with an expired number, or with a number that doesn’t match the authorized drug will deny even when the authorization itself is valid. Recording PA numbers, effective dates, and expiration dates in a centralized tracker is the administrative step that turns an approved authorization into collected revenue.
How does provider credentialing affect drug prior authorization?
Drug PA requests submitted under a provider not enrolled with the patient’s payer are rejected before clinical review because the payer cannot verify the prescriber’s network status. For practices adding new providers, this means PA submissions under that provider will fail until payer credentialing is complete, which takes 90 to 120 days for commercial payers. Starting credentialing the day a hire is confirmed, not the start date, closes this gap and prevents PA rejections that delay patient medication access.
Related Resources from Qualigenix
Drug PA Fails Before It Starts When Credentialing Is Missing. We Fix That.
Qualigenix ensures every prescribing provider in your practice is enrolled with the right payers before drug PA requests go out. We manage credentialing, payer enrollment, CAQH maintenance, and the full billing cycle so authorized medications get claimed, posted, and collected accurately.
Our team delivers 99% claim accuracy, a 95% first-pass acceptance rate, an average 36-day collection cycle, and a 30% reduction in AR days. We onboard in as few as 6 days.
Precision. Progress. Qualigenix.
What’s Next
Medical Coding Errors That Cost Practices the Most (And How to Catch Them Before They Submit)
Medical Coding Errors That Cost Practices the Most (And How to Catch Them Before They Submit) Written by the...
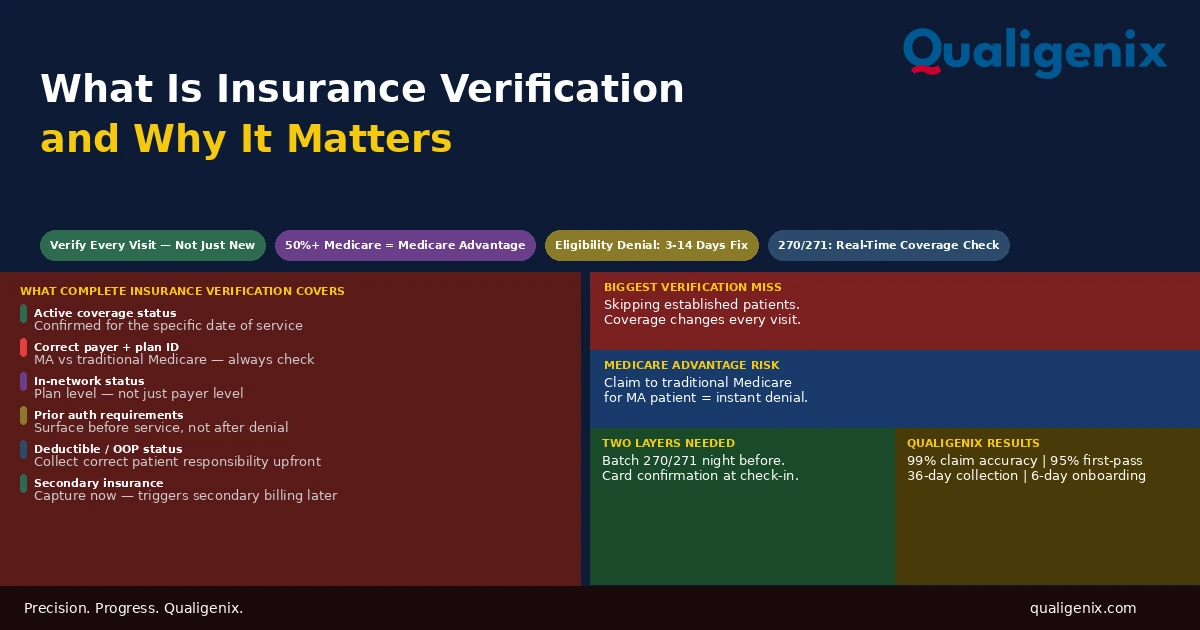
What Is Insurance Verification and Why It Matters
Insurance verification is the front-end process that determines whether a claim will be paid before the patient ever enters...

Insurance Denial Appeals: What Practices Miss
Most insurance denial appeals that fail don’t fail because the clinical case was weak. They fail because the...