What Is Medical Credentialing? Complete Guide 2026
The Qualigenix Editorial Team consists of certified billing and coding experts with over 40 years of experience across 38+ medical specialties. Our content is rigorously researched against CMS, AMA, and payer-specific guidelines to ensure total compliance and accuracy. We apply the same elite standards to our resources as we do our client work, consistently delivering high claim accuracy and significant reductions in AR days.
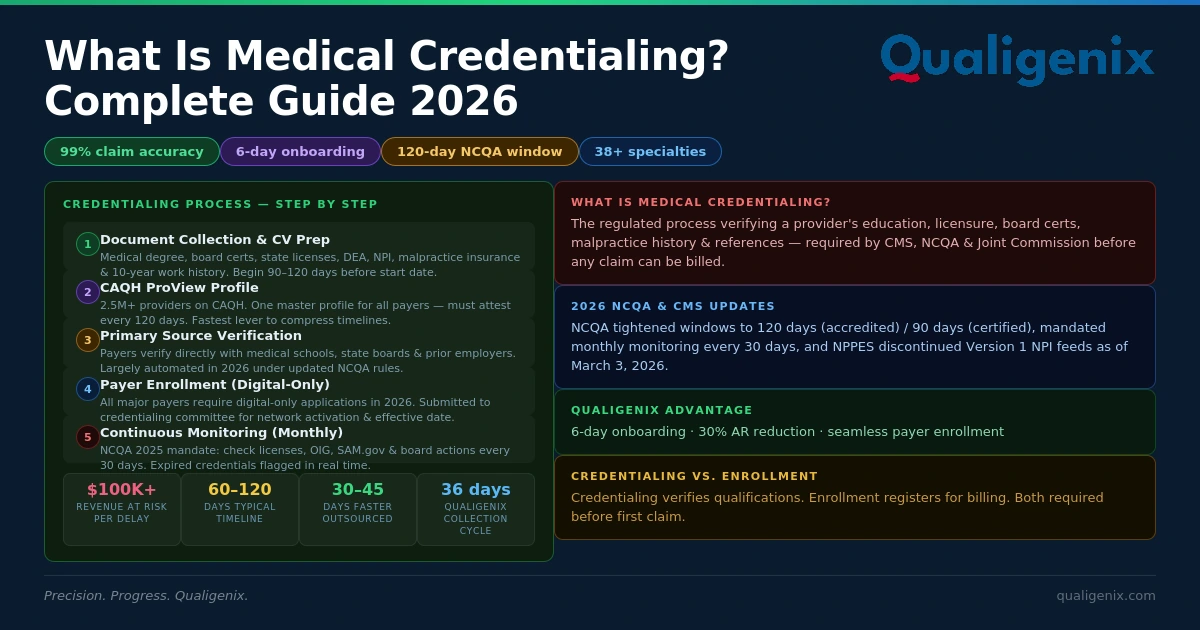
Key Takeaways: Medical credentialing is the required verification process that confirms a provider’s qualifications before they can treat patients and get paid by insurance payers. Without it, your practice cannot submit a single billable claim. In 2026, NCQA’s tighter windows (120 days) and new monthly monitoring rules make getting this right — and fast — more consequential than ever. This guide covers every step, every pitfall, and how to protect your revenue from Day 1.
Medical credentialing sits at the very beginning of your revenue cycle. Before your new physician sees a single patient, before your billing team submits one claim, every insurance payer wants proof that your provider is exactly who they say they are. That’s what the credentialing process delivers. Skip a step, leave a document incomplete, or let your CAQH profile expire — and the revenue pipeline stalls for weeks, sometimes months.
For solo physicians and group practices alike, the stakes are real. A 90-day enrollment delay for a high-volume specialist can create a six-figure backlog of unbillable services (ProMBS, 2026). That’s cash your practice earned but cannot collect until the paperwork is resolved. Understanding the full credentialing process — and managing it proactively — is one of the most direct ways to protect your financial health.
This guide walks through what medical credentialing means, how the step-by-step process works, what the 2026 regulatory updates from NCQA and CMS require, and how Qualigenix’s medical credentialing services help practices start billing faster with fewer delays.
What Is Medical Credentialing?
Medical credentialing is the regulated process of verifying a healthcare provider’s education, training, state licensure, board certifications, malpractice history, and professional references before they are approved to practice within a healthcare organization or bill insurance payers. Required by CMS, NCQA, and the Joint Commission, credentialing confirms that every licensed provider delivering care meets established safety and competency standards.
Think of it as the healthcare industry’s background check — except the stakes are clinical and financial simultaneously. Hospitals, health plans, and physician groups must credential every provider independently. That means a physician joining a new practice may need to credential with five or six payers in parallel. Each one follows its own timeline, uses its own application format, and has its own internal review committee.
There is an important distinction worth clarifying early: credentialing and payer enrollment are related but different. Credentialing confirms qualifications. Enrollment registers the approved provider with a specific insurance plan so they can receive reimbursement. You cannot complete enrollment until credentialing is done — and your practice cannot bill until both are complete and an effective date is confirmed.
Medical Credentialing: Key Statistics and Benchmarks (2026)
| Metric | Value / Benchmark |
|---|---|
| Typical credentialing timeline | 60–120 days (up to 6 months without proper documentation) |
| NCQA credentialing window (accredited orgs) | 120 days (reduced from 180 days, effective 2025) |
| NCQA credentialing window (certified orgs) | 90 days (reduced from 120 days, effective 2025) |
| NCQA monthly monitoring requirement | Every 30 days — licenses, OIG, SAM.gov, board actions (effective July 1, 2025) |
| Providers in CAQH ProView | 2.5+ million (accepted by most commercial payers in all 50 states) |
| CAQH attestation frequency required | Every 120 days (180 days in Illinois) |
| Revenue at risk per enrollment delay | $100,000+ unbillable backlog per delayed specialist (ProMBS, 2026) |
| Timeline reduction from outsourced credentialing | 30–45 days faster (ProMBS, 2026) |
| Qualigenix claim accuracy rate | 99% |
| Qualigenix first-pass acceptance rate | 95% |
| Qualigenix average onboarding time | 6 days |
| Qualigenix AR days reduction | 30% average reduction after credentialing and RCM optimization |
| Qualigenix average collection cycle | 36 days — from claim submission to payment posting |
What Documents Are Required for Medical Credentialing?
The documentation demands vary slightly by payer, but the core set is consistent across Medicare, Medicaid, and commercial carriers. Missing even a single item sends the entire application back for corrections — losing weeks in the queue. Prepare these before you submit anything:
- Medical school diploma and official transcripts: The National Student Clearinghouse enables electronic degree verification from most accredited schools.
- Residency and fellowship completion certificates: With full program name, address, dates attended (month and year), and director contact.
- Current state medical license(s): Every state where the provider practices. Check expiration dates — expired licenses auto-reject applications.
- DEA registration certificate: Required for prescribing providers; must show a current expiration date.
- Board certification certificate(s): From the American Board of Medical Specialties (ABMS) or equivalent specialty board.
- Malpractice insurance face sheet: Minimum coverage amounts vary by payer and state. Include the full 10-year claims history.
- National Provider Identifier (NPI): Type I (individual) and Type II (group/organization) from NPPES. Note: NPPES discontinued Version 1 file support as of March 3, 2026.
- Hospital and group affiliations: Current and past, with addresses and dates.
- NCQA-compliant CV: Month and year format throughout, no employment gaps, 10-year minimum history.
- Peer references: Typically two or three non-family physicians who can vouch for clinical competence.
⚠️ 2026 Compliance Alert: As of March 3, 2026, CMS discontinued support for the NPPES Version 1 downloadable file format. If your practice or billing vendor uses automated NPI data feeds, confirm those systems have migrated to Version 2. Outdated feeds can create data mismatches that delay downstream credentialing applications (MedSoler RCM, 2026).
How Does the Medical Credentialing Process Work — Step by Step?
The process moves in sequence. Skipping steps or submitting out of order doesn’t save time — it creates rework. Here is the standard workflow followed by NCQA-compliant organizations and most commercial payers.
Step 1 — Document Collection and CV Preparation
Start gathering documents months before the provider’s intended start date. Smart practices create a credentialing checklist per provider and begin this phase 90–120 days in advance. A CV with a single unexplained gap in work history is one of the top reasons applications stall in committee review. Set the right foundation and the rest of the process moves significantly faster.
Step 2 — CAQH ProView Profile Build or Update
The Council for Affordable Quality Healthcare (CAQH) operates the ProView database used by most commercial payers. Over 2.5 million providers maintain profiles here, and payers access it directly instead of requesting redundant documentation. A complete, fully attested CAQH profile is the single fastest lever you have for compressing credentialing timelines. Incomplete profiles generate supplemental document requests — each one adding days. Attest the profile on submission and set a calendar reminder: re-attestation is required every 120 days or the profile suspends automatically.
Step 3 — NPI Verification
Confirm Type I and Type II NPIs through NPPES. Ensure addresses and specialty codes are current. A single address discrepancy between your medical license and your Medicare enrollment can trigger automatic payment suspension (ProMBS, 2026). With the March 2026 NPPES Version 1 discontinuation, any practice using automated NPI data feeds must confirm migration to Version 2 before submitting any new credentialing application.
Step 4 — Medicare Enrollment via PECOS
CMS manages Medicare enrollment through PECOS (Provider Enrollment, Chain and Ownership System). The system went fully paperless — mailing paper applications only adds delays and is no longer necessary as of March 2026. Use Form CMS-855I for individual providers, CMS-855B for group practices, and CMS-855R for reassignment of benefits. Medicaid adds another layer, processed through each state’s dedicated portal with its own requirements.
Step 5 — Commercial Payer Applications
Submit individual applications to Aetna, Cigna, UnitedHealthcare, BCBS, Humana, and other commercial carriers. Even though CAQH supplies baseline data, most payers still require supplemental forms, executed contracts, and fee schedule acknowledgements. Each payer has its own portal, its own quirks, and its own processing team. Tracking every application with a credentialing matrix is essential — without it, follow-up falls through the cracks and delays compound quietly.
Step 6 — Primary Source Verification (PSV)
This is the most time-intensive stage. Each payer verifies credentials directly from the issuing authority: state licensing boards, the National Practitioner Data Bank (NPDB), the American Medical Association (AMA), and accredited medical schools. The CAQH Primary Source Verification solution automates much of this through database checks, but manual follow-up is often still required. Expect this stage to consume 30–60 days per payer.
Step 7 — Credentialing Committee Review and Approval
The payer’s credentialing committee conducts a final review of the verified file. Any sanctions, malpractice claims, licensing gaps, or board actions trigger additional scrutiny. Under NCQA’s updated 2025–2026 standards, accredited organizations must complete this entire process within 120 days (down from 180). That’s a 33% reduction in available time while verification requirements have actually increased.
Step 8 — Effective Date Confirmation
Approval alone does not authorize billing. Get written confirmation of the provider’s effective billing date with each payer and verify that NPI and Tax ID alignments are correct. Most commercial payers prohibit retroactive billing entirely. Bill before the confirmed effective date, and those claims will be denied — often permanently.
Can a Provider See Patients Before Credentialing Is Complete?
Clinically yes — financially, no. Hospitals and ASCs may grant provisional privileges before full credentialing is complete under specific JCAHO policies. However, most commercial payers will not process claims for services rendered before the provider’s confirmed effective enrollment date. Medicare and Medicaid do not allow retroactive billing in most circumstances. The safe assumption: a provider cannot be paid for services until credentialing and enrollment are both complete and an effective date is confirmed in writing.
Credentialing vs. Payer Enrollment vs. Privileging: What Is the Difference?
These three terms are frequently used interchangeably — and incorrectly. Each represents a distinct function in the provider onboarding process. Understanding the difference prevents costly operational confusion.
| Factor | Medical Credentialing | Payer Enrollment | Clinical Privileging |
|---|---|---|---|
| Purpose | Verify provider’s qualifications and identity | Register provider with a specific insurance plan for payment | Grant permission to perform specific procedures at a facility |
| Who performs it | Hospital, health plan, or credentialing organization | Insurance payer (Medicare, Medicaid, commercial) | Hospital or ASC medical staff committee |
| Required by | CMS, NCQA, Joint Commission | CMS (PECOS), state Medicaid, commercial payers | The Joint Commission, state hospital licensing boards |
| Output | Approved provider status + credential | Provider ID, effective date, in-network participation | Approved procedure list for a specific facility |
| Comes first? | Yes — must occur before enrollment | Second — follows credentialing approval | Parallel — hospital-specific, separate from payer enrollment |
| Renewal cycle | Every 2–3 years (recredentialing) + monthly monitoring | Medicare revalidation every 3–5 years | Typically every 2 years per facility |
Why Does Medical Credentialing Take So Long?
The single biggest driver of credentialing delays is incomplete or inaccurate documentation — not payer processing speed. Most delays practices experience are self-inflicted: missing malpractice history, an unexplained CV gap, an expired DEA certificate, or a CAQH profile that hasn’t been attested in six months. When a payer requests supplemental documents mid-process, the application re-enters the queue from the beginning.
Primary source verification with licensing boards and medical schools adds additional wait time — especially for international medical graduates. The National Practitioner Data Bank (NPDB) query, DEA confirmation, and OIG exclusion screening are all separate workflows. Each runs independently, and the slowest one sets the final timeline. Practices that outsource credentialing to a specialist can reduce this timeline by 30–45 days by eliminating the back-and-forth that comes from incomplete initial submissions (ProMBS, 2026).
What Changed in Credentialing Regulations for 2026?
Three major regulatory shifts took effect in 2025 and 2026. First, NCQA reduced credentialing approval windows by 33% — accredited organizations now have 120 days (down from 180), and certified organizations have 90 days. Second, all credentialing files processed on or after July 1, 2025 require provider monitoring every 30 days. Third, CMS discontinued NPPES Version 1 file support on March 3, 2026. Telehealth credentialing is now also a separate process requiring payer-specific attestation.
The monthly monitoring requirement is the most operationally disruptive change. Before 2025, practices checked credentials every six months or during recredentialing cycles every two to three years. Now every provider file must be reviewed monthly for license status, OIG exclusions, state medical board actions, and SAM.gov screening. Manual tracking at this frequency is practically impossible without a credentialing management system or outsourced partner.
The Interstate Medical Licensure Compact (IMLCC) now includes 42 member states following North Carolina’s addition. While this simplifies multi-state licensure applications, each state still has its own renewal cycles and documentation standards — meaning multi-state practices still need disciplined tracking systems.
How Does Qualigenix Handle Medical Credentialing for Your Practice?
Qualigenix’s medical credentialing services cover the entire provider lifecycle — from initial document collection through ongoing monthly monitoring and triennial recredentialing. The difference between managing this in-house and outsourcing to an experienced RCM partner is measurable in both time and revenue.
Most practices that handle credentialing internally spend three to four times longer in the process because of incomplete initial submissions, missed follow-up windows, and CAQH attestation lapses. Qualigenix’s credentialing specialists manage:
- CAQH profile builds and quarterly attestations: Every profile is built completely from the start, with re-attestation tracked and executed on schedule — no lapses, no suspended profiles.
- PECOS and Medicare enrollment submissions: CMS-855I, CMS-855B, and CMS-855R submissions handled in parallel with commercial applications to compress total timelines.
- Commercial payer applications across all major carriers: Aetna, Cigna, UnitedHealthcare, BCBS, Humana, and regional plans — tracked in a live credentialing matrix with proactive follow-up.
- Primary source verification coordination: Proactive follow-up with licensing boards, medical schools, and certification bodies to prevent PSV from becoming a bottleneck.
- NCQA monthly monitoring cadence: Every provider file reviewed every 30 days for license status, OIG exclusions, board actions, and SAM.gov screening — fully compliant with July 2025 requirements.
- Recredentialing management: Our recredentialing services handle payer cycles every 2–3 years, ensuring no provider’s credentials lapse mid-cycle.
The result: faster effective dates, fewer claim denials tied to enrollment gaps, and a practice that starts generating revenue from new providers weeks sooner. Qualigenix achieves a 99% claim accuracy rate and 95% first-pass acceptance rate — numbers that reflect the downstream benefit of getting credentialing right from the start. Average onboarding to active credentialing management takes just 6 days.
Credentialing also integrates directly with denial management and claim submission services. When a provider’s enrollment status is tracked in real time alongside claim workflows, enrollment-related denials get caught before submission — not after.
What Is the Revenue Risk of a Credentialing Delay?
A 90-day enrollment delay for a high-volume specialist can create a $100,000+ backlog of unbillable services (ProMBS, 2026). That’s revenue your practice earned but cannot collect until the credentialing and enrollment paperwork resolves. Most commercial payers prohibit retroactive billing, meaning those claims may be permanently unrecoverable — not just delayed.
The financial exposure compounds when you factor in staff time spent chasing payers, the cost of locum coverage, and patient dissatisfaction from scheduling delays. Practices that start the credentialing process 90–120 days before a provider’s first date of service — and submit complete applications the first time — eliminate most of this exposure entirely.
Medical Credentialing Readiness Checklist: 10 Steps Before You Submit
- ☐ CV audit complete: Every position accounted for with month and year, no gaps exceeding 30 days unexplained, minimum 10-year history
- ☐ All licenses current and verified: State medical license(s), DEA, and any specialty certifications checked for expiration dates at least 90 days ahead of submission
- ☐ CAQH ProView fully populated and attested: All sections completed — work history, education, malpractice coverage, affiliations. Attested within the last 120 days
- ☐ NPPES NPI confirmed: Type I and Type II NPIs verified, specialty codes current, NPPES migrated to Version 2 data feeds as of March 2026
- ☐ PECOS profile active and current: Medicare enrollment records in PECOS match license and practice address. Revalidation deadlines tracked
- ☐ Malpractice face sheet secured: Current policy, minimum coverage confirmed per payer requirements, 10-year claims history documented
- ☐ Board certification status confirmed: ABMS or specialty board certification current; maintenance of certification requirements met
- ☐ Hospital and group affiliations documented: All current and former affiliations listed with complete contact information and dates
- ☐ NPDB self-query run: Provider has verified their own National Practitioner Data Bank record and resolved any discrepancies before payers find them
- ☐ Monthly monitoring cadence established: Process in place to check license status, OIG exclusions, board actions, and SAM.gov every 30 days per NCQA 2025 requirements
Frequently Asked Questions About Medical Credentialing
What is medical credentialing?
Medical credentialing is the formal process of verifying a healthcare provider’s education, training, licensure, board certifications, malpractice history, and professional references before they are approved to treat patients and bill insurance payers. It is required by CMS, NCQA, and the Joint Commission as a condition of Medicare, Medicaid, and commercial network participation.
Every payer maintains its own credentialing committee, and every provider must credential separately with each payer they want to join. There is no single universal credentialing approval — though the CAQH ProView database standardizes much of the underlying data collection across commercial carriers.
How long does medical credentialing take?
Medical credentialing typically takes 60–120 days, though it can extend to six months when documentation is incomplete or applications are submitted via fax or mail. NCQA’s 2025 updates shortened the maximum credentialing window from 180 to 120 days for accredited organizations and from 120 to 90 days for certified organizations.
The fastest way to compress that timeline is to start 90–120 days before the provider’s intended start date and submit a complete, fully documented application. Outsourcing to a credentialing specialist eliminates the back-and-forth caused by incomplete submissions and can shorten the process by 30–45 days.
What is the difference between credentialing and payer enrollment?
Credentialing verifies a provider’s qualifications and grants them approved status. Payer enrollment is the separate process of registering that approved provider with specific insurance plans — Medicare, Medicaid, and commercial carriers — so they can receive reimbursement. Credentialing must be completed before enrollment can begin, and both must be complete before billing starts.
Many practices confuse the two and assume that credentialing approval automatically means billing can begin. It doesn’t. You still need a signed contract, an active effective date, and confirmed provider identifiers before your first claim can be submitted.
What is CAQH and why does it matter for credentialing?
CAQH (Council for Affordable Quality Healthcare) operates ProView, the centralized credentialing database used by most commercial insurance payers. More than 2.5 million providers maintain profiles in CAQH, which payers access directly. The profile must be fully completed and attested every 120 days — an expired or incomplete profile delays every application tied to it.
A well-maintained CAQH profile eliminates the bulk of supplemental documentation requests. Think of it as your credentialing resume that follows you across carriers. Neglect it, and everything slows down.
Can a provider bill insurance before credentialing is complete?
No. A provider cannot bill Medicare, Medicaid, or most commercial payers until credentialing and payer enrollment are both complete and a confirmed effective billing date is on file. Submitting claims before the effective date results in automatic denials. Most commercial payers prohibit retroactive billing entirely — meaning those claims may never be recoverable.
What are the most common reasons medical credentialing gets delayed?
The most common causes are: incomplete CAQH profiles, missing or outdated malpractice history, CV gaps or formatting errors, inconsistent information across applications, failure to follow up during primary source verification, expired licenses or DEA registration, and missing peer references. Most of these are self-inflicted and preventable with a complete first submission.
What are the 2026 NCQA credentialing requirements?
NCQA’s 2025 updates require monthly provider monitoring (every 30 days) for all files processed on or after July 1, 2025 — covering license status, OIG exclusions, state board actions, and SAM.gov screening. Credentialing approval windows were shortened to 120 days for accredited organizations and 90 days for certified organizations. Telehealth credentialing now requires separate payer attestation.
These changes require practices to fundamentally redesign their credentialing workflows. Manual tracking at monthly frequency is not practical without automation or an outsourced credentialing partner. Failure to comply risks loss of accreditation and potential payment suspension.
How does Qualigenix help with medical credentialing?
Qualigenix manages the full credentialing lifecycle — document collection, CAQH profile builds and attestations, PECOS Medicare enrollment, commercial payer applications, primary source verification coordination, monthly NCQA monitoring, and triennial recredentialing. Practices benefit from faster provider activation, fewer enrollment-related denials, and a 99% claim accuracy rate. Average onboarding is 6 days.
Related Qualigenix Resources
Service Pages:
- Medical Credentialing Services
- Recredentialing Services
- Medicare Revalidation Services
- Denial Management Services
- Claim Submission Services
- Revenue Cycle Management Services
Blog Guides:
- How Payer Enrollment Services Speed Credentialing
- Provider Enrollment Process: Step-by-Step Guide
- Top Provider Enrollment and Credentialing Services (2026)
- Denial Management Process: 5 Essential Steps
- How to Appeal an Insurance Claim Denial Step by Step
- What Is Revenue Cycle Management? A Beginner’s Guide
- What Is CAQH? The Complete Provider Guide
- Healthcare Billing Process Explained: End-to-End Workflow
Ready to Get Your Providers Credentialed Faster?
Every day of delay is revenue your practice can’t recover. Qualigenix’s credentialing specialists manage the entire process — from CAQH builds to effective date confirmation — so your team can stay focused on patient care.
Our team delivers 99% claim accuracy, a 95% first-pass acceptance rate, and an average 36-day collection cycle. We onboard in as few as 6 days, starting with a comprehensive AR assessment that identifies every credentialing gap costing your practice revenue.
Precision. Progress. Qualigenix.
What’s Next

Prior authorization turnaround requirements under the CMS interoperability rule: what changed for practices
The CMS interoperability rule (CMS-0057-F) forces impacted payers to decide standard prior authorizations in 7 calendar days and...
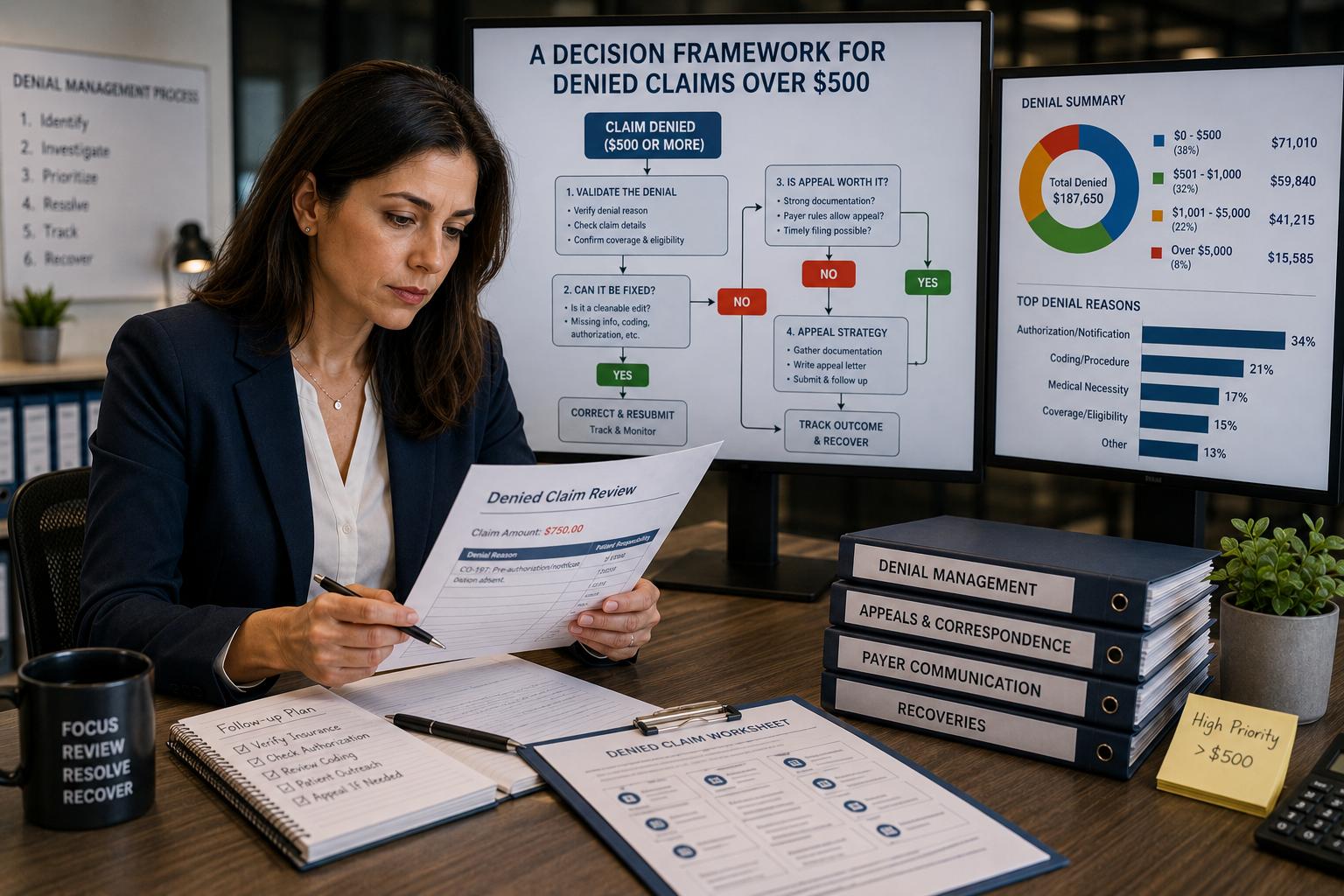
Appeal or Write Off? A Decision Framework for Denied Claims Over $500
Don’t let the dollar amount make the call by itself. Sort the denial by reason code, run the...
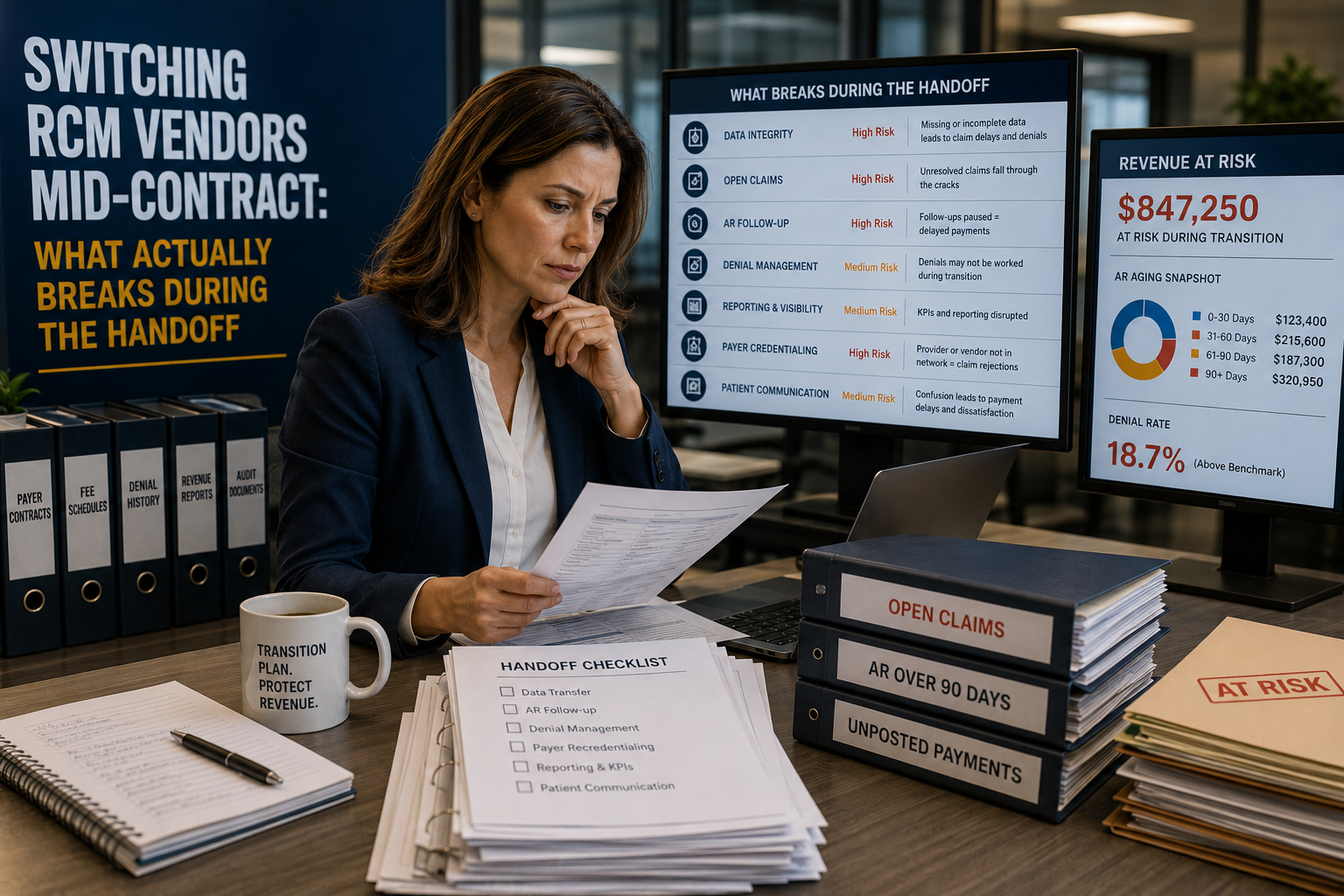
Switching RCM Vendors Mid-Contract: What Actually Breaks During the Handoff
Switching RCM vendors before a contract ends feels like the fast fix for a billing team that’s underperforming....