What Is Healthcare Coding and How It Works
The Qualigenix Editorial Team consists of certified billing and coding experts with over 40 years of experience across 38+ medical specialties. Our content is rigorously researched against CMS, AMA, and payer-specific guidelines to ensure total compliance and accuracy. We apply the same elite standards to our resources as we do our client work, consistently delivering high claim accuracy and significant reductions in AR days.
Healthcare coding is the translation layer between what a physician does and what an insurer pays for. A physician sees a patient, makes clinical decisions, performs services, and documents the encounter. A coder reads that documentation and assigns standardized codes. CPT codes for what was done, ICD-10 codes for why it was done, and modifiers for how it was done when that context changes how the payer adjudicates it. Those codes travel on the insurance claim to the payer, who reimburses based on the code submitted, not based on what the physician actually did. Every coding decision has a revenue consequence. A correctly coded claim pays at the right rate. An undercoded claim pays at a lower rate with no signal that revenue was left behind. A miscoded claim denies. The accuracy of the translation determines the financial outcome of every encounter the practice bills.
Healthcare coding is one of those functions that is invisible when it works correctly and highly visible when it doesn’t. When a physician sees a patient with moderately complex medical needs, the coder assigns the right E/M code, links it to the right diagnosis codes, applies the appropriate modifier, and the claim pays at the correct rate within 30 days. Nobody noticed healthcare coding working. The money arrived.
When a physician sees the same patient and the coder assigns an E/M code one level below what the documentation supports, the claim also pays at a lower rate, without a denial, without an alert, without any indication that the practice collected $40 less than it was entitled to on that encounter. If that pattern holds across 15% of all visits the practice bills, the annual revenue loss compounds into tens of thousands of dollars per physician that no billing report surfaces because it never appears as an unpaid claim.
Healthcare coding is not administrative overhead. It is a clinical translation function whose accuracy determines revenue outcomes at the level of every individual encounter, every day, across the full lifetime of the practice. Understanding what it covers, how it works, and what its failure modes cost is foundational knowledge for any practice that wants to manage its revenue cycle effectively.
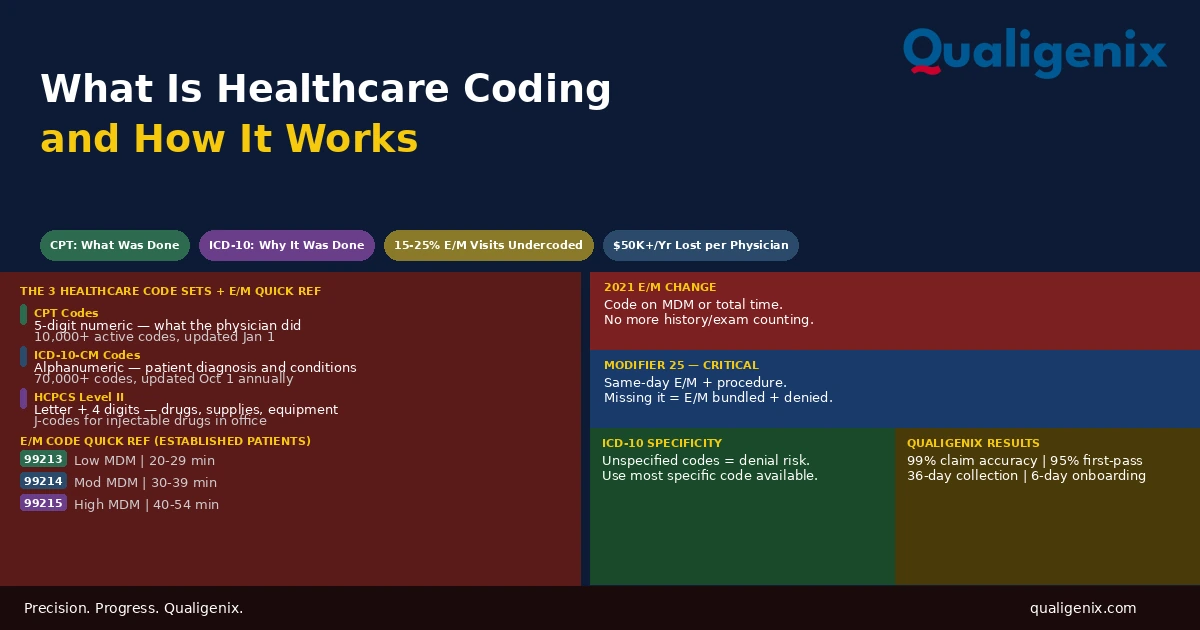
Healthcare coding is the process of translating physician documentation into standardized codes that communicate clinical services to insurance payers. The three primary code sets are CPT codes (what the physician did), ICD-10-CM codes (why it was done), and HCPCS Level II codes (supplies and drugs). Coding accuracy determines whether the correct amount is reimbursed, whether the claim passes payer edits on first submission, and whether the practice’s revenue cycle operates at benchmark performance or below it.
Healthcare Coding: Key Facts and Benchmarks
| Data Point | Value | Source / Context |
|---|---|---|
| Active CPT codes in current code set | Over 10,000 | AMA CPT 2026 |
| Active ICD-10-CM diagnosis codes | Over 70,000 | CMS ICD-10-CM 2026 |
| Annual CPT code update effective date | January 1 each year | AMA CPT annual revision cycle |
| Annual ICD-10-CM update effective date | October 1 each year | CMS ICD-10 update cycle |
| E/M visits billed below documented complexity | 15% to 25% of outpatient encounters | Coding audit benchmarks |
| Annual revenue lost to undercoding per physician | $10,000 to $50,000+ | Physician revenue analysis |
| Denials tracing to coding errors | Approximately 25% to 30% of all denials | Medical billing denial analysis |
| Clean claim rate benchmark | 95% or higher | MGMA and HFMA standards |
| 2021 AMA E/M code selection basis (outpatient) | MDM complexity or total time on DOS | AMA E/M guideline revision 2021 |
| Qualigenix claim accuracy rate | 99% | Qualigenix performance data |
| Qualigenix first-pass acceptance rate | 95% | Qualigenix performance data |
| Qualigenix average collection cycle | 36 days | Qualigenix performance data |
The Three Code Sets in Healthcare Coding
Healthcare coding draws on three distinct code sets, each serving a specific purpose on the insurance claim. Understanding what each covers and what happens when each is applied incorrectly that clarifies why coding is the revenue-determining function it is.
CPT Codes: What Was Done
Current Procedural Terminology codes are published and maintained by the American Medical Association and updated annually each January. They are five-digit numeric codes organized into six major categories: Evaluation and Management, Anesthesia, Surgery, Radiology, Pathology and Laboratory, and Medicine.
CPT codes describe the specific service the physician performed. A 99214 describes a moderate-complexity established patient office visit. A 27447 describes a total knee arthroplasty. A 93000 describes a routine electrocardiogram with interpretation and report. Each code has a specific definition, a specific set of documentation requirements, and a specific reimbursement amount under each payer’s fee schedule.
The CPT code on a claim is the primary determinant of reimbursement amount. Payers maintain fee schedules that assign a dollar value to each CPT code. When the code is correct, the reimbursement matches the service delivered. When the code understates the service a lower-complexity E/M code when a higher one was documented, a less-specific procedure code when a more-specific one exists, the reimbursement is permanently lower than what the service warranted. No denial is generated. The claim pays at the lower rate and the revenue difference is gone.
CPT codes are updated annually. New codes are added for new technologies and procedures. Old codes are deleted when they are no longer appropriate. Existing codes are revised when their descriptions change. A coder using a deleted CPT code after January 1 of the year it was deleted will produce a claim that denies for invalid code. Annual training before the code update takes effect is not optional it is a revenue cycle requirement.
ICD-10-CM Codes: Why It Was Done
ICD-10-CM codes are the diagnosis classification system used for physician professional billing in the United States. They are alphanumeric codes of up to seven characters that identify specific diseases, conditions, symptoms, injuries, and reasons for encounters. The system contains over 70,000 codes, providing a level of specificity that allows the patient’s clinical situation to be communicated precisely.
ICD-10-CM codes serve two critical functions on the insurance claim. First, they establish medical necessity, they communicate to the payer that the services billed were clinically appropriate for the patient’s documented condition. Second, they provide clinical data that feeds quality reporting, risk adjustment, population health analytics, and value-based care contracts that increasingly affect practice revenue beyond fee-for-service payment.
The most consequential ICD-10 coding failure is specificity gaps. ICD-10 provides more specific codes for most conditions than many practices routinely use. Type 2 diabetes mellitus with diabetic peripheral angiopathy without gangrene has a specific code. Type 2 diabetes mellitus, unspecified also has a code. The unspecified code is technically acceptable when the documentation genuinely doesn’t support the more specific code. But using the unspecified code when the documentation clearly documents the specific complication is a coding specificity failure that represents both a clinical documentation accuracy problem and a revenue risk for payers who use diagnosis specificity to evaluate medical necessity.
ICD-10-CM is updated by CMS twice per year: October 1 is the primary update cycle with the largest set of additions, deletions, and revisions. A mid-year update may add codes effective April 1 for time-sensitive clinical needs. Practices that don’t incorporate October 1 ICD-10 updates before they take effect will generate claims with deleted codes or miss new, more specific codes that payers require for covered services. Coding compliance with the current code set is a revenue cycle function, not just a regulatory one.
HCPCS Level II Codes: Supplies, Equipment, and Drugs
HCPCS Level II codes cover services, supplies, and drugs that CPT codes don’t describe. They are alphanumeric codes beginning with a letter (A through V) followed by four digits, organized into code groups by category.
For physician practices, the most frequently used HCPCS Level II codes are J-codes, the subset of HCPCS codes used to bill drugs administered in the physician’s office. When a physician administers an injectable medication, infusion therapy, or biologic drug in the office or clinic, the drug itself is billed using its specific J-code in addition to the administration CPT code. J-code billing requires knowing the specific drug, its form, the unit of billing, and the units administered. An incorrect J-code wrong drug, wrong unit, wrong quantity produces a claim that either denies or pays at an incorrect rate.
For practices that provide durable medical equipment, orthotics, prosthetics, or other supplies billed separately from physician services, HCPCS Level II codes are the primary coding mechanism. Each item has a specific HCPCS code with specific documentation requirements for medical necessity and coverage.
Evaluation and Management Coding: The Core of Most Physician Practices
For the majority of physician practices, Evaluation and Management coding is the dominant revenue-generating coding category. E/M codes represent the intellectual and clinical work of the physician visit the history obtained, the examination performed, the data reviewed, and the decisions made. The code level assigned determines the reimbursement for the physician’s professional work, independent of any procedures that may also be billed.
The 2021 AMA revision to E/M coding guidelines was the most significant change to this code set in decades. The prior system required counting specific history and physical examination elements to justify code levels. The revised system allows outpatient office visit code selection based on either medical decision making (MDM) complexity or total time spent on the date of the encounter. This change eliminated the documentation burden of counting elements and aligned code selection with clinical complexity rather than documentation quantity.
Outpatient E/M Code Structure (2026)
| Code | Patient Type | MDM Level | Time Range | Typical Encounter |
|---|---|---|---|---|
| 99202 | New | Straightforward | 15-29 min | Single self-limited problem |
| 99203 | New | Low | 30-44 min | Stable chronic condition |
| 99204 | New | Moderate | 45-59 min | New problem requiring workup |
| 99205 | New | High | 60-74 min | Complex problem, high risk |
| 99212 | Established | Straightforward | 10-19 min | Self-limited minor problem |
| 99213 | Established | Low | 20-29 min | 1-2 stable chronic conditions |
| 99214 | Established | Moderate | 30-39 min | Chronic with complexity or Rx mgmt |
| 99215 | Established | High | 40-54 min | Severe exacerbation or high risk |
The most costly E/M coding failure in most practices is systematic undercoding of established patient visits. A physician who habitually bills 99213 for encounters that document moderate MDM prescription drug management, two or more active chronic conditions, or a new problem requiring workup is leaving $35 to $50 per encounter in Medicare reimbursement on the table, and proportionally more with commercial payers that typically pay at multiples of Medicare rates. At 10 to 15 undercoded visits per day across a practice, this represents revenue in the low to mid tens of thousands of dollars per physician per year that produces no denial and triggers no audit flag.
Medical Decision Making: The Coding Standard That Determines E/M Level
Medical decision making is the primary standard for outpatient E/M code selection under the 2021 guidelines. It is assessed across three elements that together determine the overall MDM complexity of the encounter.
Element 1: Problems Addressed
The number and complexity of the problems the physician addressed during the encounter contribute to MDM complexity. A single self-limited or minor problem supports straightforward MDM. One stable chronic illness supports low MDM. Two or more stable chronic illnesses, or one unstable chronic illness, supports moderate MDM. A chronic illness with severe exacerbation or a problem that threatens life or bodily function supports high MDM.
Element 2: Data Reviewed and Analyzed
The amount and complexity of data the physician reviewed and analyzed during the encounter contributes to MDM complexity. This includes reviewing tests ordered, external notes or records, independent interpretations of results, and discussion with another provider about the patient’s care. The data element distinguishes encounters where the physician is managing straightforward conditions from encounters where active investigation, consultation review, or complex data analysis is occurring.
Element 3: Risk of Complications
The risk associated with the clinical decisions made contributes to MDM complexity. Low risk includes over-the-counter medications or minor procedures without identified risk factors. Moderate risk includes prescription drug management, decisions about minor surgery with identified risk factors, or social determinants that affect treatment. High risk includes decisions about major surgery, drug therapy requiring intensive monitoring for toxicity, or diagnoses with a possible threat to life or bodily function requiring urgent referral.
The overall MDM level is determined by the highest level achieved in at least two of the three elements. A physician managing two chronic conditions (moderate problems), reviewing recent lab results (moderate data), and prescribing a new medication (moderate risk) has three elements at moderate, supporting 99214. A physician managing the same patient but documenting only the prescription change without documenting the complexity of the conditions being managed or the data reviewed may only support 99213 not because the clinical work was less complex but because the documentation didn’t capture the complexity.
Modifiers: The Context Layer That Changes How Claims Pay
Modifiers don’t change what a CPT code describes. They add context about the circumstances of service delivery that affects how the payer should adjudicate the claim. Missing a required modifier causes a denial. Applying the wrong modifier causes incorrect adjudication. Applying no modifier when one is needed allows payers to bundle separately payable services together, eliminating payment for one of them.
The Most Consequential Modifiers in Physician Billing
Modifier 25 is appended to an E/M code when a significant, separately identifiable E/M service was performed on the same day as a procedure. Without it, the payer bundles the E/M into the procedure fee and denies the separate E/M charge. In practices where physicians frequently perform procedures and E/M services at the same visit, missing modifier 25 across dozens of encounters per week produces a systematic denial category that billing teams often work individually without identifying the upstream coding root cause.
Modifier 59 indicates that a procedure was distinct from another service on the same day a different anatomical site, a different encounter, or a different procedure not ordinarily reported together. Without modifier 59 when the services were genuinely distinct, the payer bundles them and denies one as a component of the other. Applying modifier 59 incorrectly is an unbundling error that creates compliance exposure.
Modifier 24 is applied during the surgical global period for E/M services that are unrelated to the surgery. Without it, the E/M is bundled into the surgical global period payment and denied. With it, the separately identifiable unrelated E/M is paid independently of the surgical global fee.
Modifier 51 indicates that multiple procedures were performed at the same session. Some payers require it; some payers want it suppressed. Knowing the modifier 51 rules for each payer in the practice’s mix is a payer-specific knowledge requirement that generalist billing teams frequently get wrong on at least some payer combinations.
How Healthcare Coding Connects to Billing
Healthcare coding and medical billing are sequential functions in the revenue cycle, not simultaneous or interchangeable ones. Coding comes first: the coder reviews documentation, assigns codes, and produces a coded encounter. Billing comes second: the biller takes the coded encounter, builds the claim, submits it, posts the payment, and manages anything that doesn’t resolve correctly.
The quality of the coding determines the quality of the claim. A correctly coded encounter submitted by a competent biller produces a clean claim that pays at the right rate. A miscoded encounter submitted by the same biller produces a claim that either pays at a wrong rate or generates a denial. The biller’s process quality can’t compensate for a coding error in the input they received. And the coder’s accuracy can’t compensate for a billing error downstream a correctly coded claim submitted to the wrong payer, with the wrong place-of-service code, or missing the authorization number still fails.
The claim scrubber that sits between the coded encounter and submission is the quality control gate where coding errors that billing has the ability to catch should be stopped before they reach the payer. A well-configured scrubber catches invalid code combinations, missing modifiers, diagnosis codes that don’t support the procedure billed, and payer-specific edit failures. Coding errors the scrubber doesn’t catch reach the payer as submitted claim errors that become denials — more expensive to resolve than if they had been caught internally.
Related: Medical Billing vs Coding: Key Differences Explained
Healthcare Coding Across Clinical Settings
Healthcare coding rules are not uniform across clinical settings. The code sets, documentation requirements, code selection logic, and applicable guidelines differ depending on where the service was delivered and who delivered it.
Outpatient Office and Clinic Coding
Outpatient coding uses the CPT code set for physician professional services, with E/M code selection under the 2021 AMA MDM or time-based guidelines. The claim is submitted on the CMS-1500 form under the physician’s NPI with place-of-service code 11 (office) or 22 (outpatient hospital). This is the most common coding context for physician practices.
Inpatient Hospital Coding
Physician inpatient coding uses a different CPT code set than outpatient: 99221-99223 for hospital admission, 99231-99233 for daily subsequent visits, and 99238-99239 for discharge. Code selection still uses the key component framework history, examination, and medical decision making — rather than the 2021 outpatient MDM revision. A physician who applies outpatient MDM-only documentation to inpatient notes may be under documenting the key components that support the highest appropriate inpatient E/M code level. Related: Inpatient Coding for Physicians: What Changes
Facility Coding
Hospital facility coding is distinct from physician professional coding. It uses ICD-10-PCS procedure codes on the UB-04 form for inpatient services, and CPT codes on the UB-04 for outpatient hospital services. Facility coding drives the hospital’s DRG reimbursement under Medicare Part A, which is completely separate from the physician’s Part B professional fee. The physician’s coding and the hospital’s coding run on parallel tracks from the same patient encounter and neither directly affects the other, though the physician’s documentation quality influences the facility coder’s ability to assign the most accurate facility codes.
Healthcare Coding Compliance: What It Requires
Healthcare coding compliance is the requirement that codes assigned accurately represent what was documented in the clinical record, in accordance with the official coding guidelines and payer-specific coverage policies. Compliance is not a separate activity from accurate coding — it is the standard that accurate coding meets by definition.
The OIG compliance guidance for physician practices identifies several specific coding compliance risks: upcoding (billing a higher-level service than documented), unbundling (billing separately for services that should be billed together), and billing for services not documented. These are intentional compliance violations. The more common and less visible compliance risk is systematic undercoding billing lower-level services than documented, which is not a compliance violation but is a revenue loss that compounds invisibly.
Coding compliance requires three ongoing activities that most practices need to maintain consistently. Annual code update training before the effective date of each update. Quarterly chart audits that review coded encounters against the clinical documentation to confirm accuracy and identify systematic patterns. And a physician documentation improvement program that communicates specific documentation gaps to physicians in time for them to correct the pattern prospectively rather than retroactively.
How Qualigenix Manages Healthcare Coding
At Qualigenix, healthcare coding is a specialty-matched, continuously audited function integrated with billing into a unified revenue cycle operation. Our coders hold specialty-specific credentials for the encounter types they code, apply the 2021 AMA E/M MDM guidelines to every outpatient encounter, and review inpatient notes against key component documentation standards for hospital-based physician services.
We run monthly E/M code distribution reports for every physician across every client practice, comparing distributions against specialty benchmarks and flagging physicians where the pattern suggests systematic undercoding. We conduct quarterly chart audits sampling 10 to 15 encounters per physician and return findings with specific documentation examples. We feed audit findings back to physicians through a structured query process that identifies precisely what documentation elements would have supported a higher code on the encounters we reviewed.
Our coding feeds directly into our billing operation — no handoff gap, no attribution ambiguity when a denial arrives. The team that coded the encounter is accountable for the coded output. The team that submitted the claim is accountable for the billing output. Both are accountable to the same performance standard: 99% claim accuracy, 95% first-pass acceptance rate, 36-day collection cycle.
Related: What Is RCM in Medical Billing | Should Your Practice Outsource Medical Coding?
Healthcare Coding Readiness Checklist
- Annual CPT update training completed before January 1 each year
- Annual ICD-10-CM update training completed before October 1 each year
- E/M code distribution report pulled monthly per physician and compared to specialty benchmarks
- Quarterly chart audits sampling 10-15 encounters per physician against current MDM criteria
- ICD-10 codes assigned at maximum specificity — unspecified codes reviewed monthly
- Diagnosis-to-procedure linkage verified — each CPT linked to a supporting ICD-10
- Modifier 25 applied for same-day E/M and procedure combinations
- Coder credentials verified as specialty-matched for encounter mix
- Documentation query process in place with defined physician response window
- Coding-related denial root cause tracked monthly — above 15% of total denials triggers review
- Charge entry standard of 24-48 hours enforced to prevent charge lag
Frequently Asked Questions: Healthcare Coding
What is healthcare coding?
Healthcare coding is the translation of clinical documentation into standardized CPT, ICD-10-CM, and HCPCS codes that communicate physician services and patient diagnoses to insurance payers. Payers reimburse based on the codes submitted, not directly on what the physician did. Coding accuracy determines whether the correct reimbursement is received, whether the claim passes payer edits on first submission, and whether the practice’s revenue cycle produces the outcomes that benchmark performance requires.
What is the difference between CPT codes and ICD-10 codes?
CPT codes describe what the physician did — procedures, services, and evaluations performed. ICD-10-CM codes describe why it was done — the patient’s diagnoses and conditions. Both are required on every claim. CPT codes determine the reimbursement amount. ICD-10 codes establish medical necessity by demonstrating that the services billed were clinically appropriate for the patient’s documented condition. A mismatch between the diagnosis code and the procedure code — either the wrong diagnosis or an insufficiently specific one — produces a medical necessity denial regardless of how accurately the procedure was coded.
What are E/M codes in healthcare coding?
E/M codes are CPT codes describing physician visits and consultations — the most frequently billed category for most physician practices. Outpatient codes range from 99202 to 99215; inpatient codes from 99221 to 99233. Since the 2021 AMA guideline revision, outpatient E/M code levels are selected based on medical decision making complexity or total time on the date of service. The distinction between adjacent code levels. particularly 99213 versus 99214 for established patients represents $35 to $50 per visit in Medicare reimbursement, making accurate E/M coding the single largest revenue variable in most physician practices.
How does healthcare coding affect reimbursement?
Healthcare coding determines reimbursement directly because payers pay based on the CPT code submitted. An undercoded claim pays at a lower rate than the service warranted, with no denial and no alert the revenue loss is permanent and silent. A miscoded claim produces a denial requiring rework. A claim with a missing modifier produces bundling that eliminates separate payment for a legitimately distinct service. Every coding decision at every encounter compiles into an annual revenue outcome that either matches what the practice’s clinical work is worth or falls short of it by the cumulative margin of every coding gap across every encounter billed.
What updated with the 2021 AMA E/M coding changes?
The 2021 AMA E/M revision changed outpatient office visit code selection from a history-and-exam component counting system to a MDM complexity or total time basis. Physicians no longer need to document specific history or examination elements to justify code levels for most outpatient visits. Code level is determined by the complexity of the clinical work: the number and nature of problems addressed, the data reviewed, and the risk of the treatment decisions made. Practices that haven’t fully adopted MDM-based documentation are either overcounting elements that no longer determine the level or under documenting the MDM elements that do.
Who performs healthcare coding and what credentials do they need?
Healthcare coding is performed by certified medical coders holding AAPC CPC or AHIMA CCS credentials, often with specialty certifications for complex encounter types. In smaller practices, billing staff with coding training sometimes perform coding alongside billing functions. Specialty certifications in orthopedics, cardiology, oncology, and other fields. Validate specialty-specific coding expertise beyond the general credential. As encounter complexity increases and specialty mix diversifies, the credential match between the coder and the encounter type becomes a direct determinant of coding accuracy.
Related Resources from Qualigenix
Accurate Coding. Correct Claims. Collected Revenue.
Qualigenix manages healthcare coding and billing as integrated, specialty-matched functions for practices across 38+ specialties. Our coders apply current guidelines, run monthly distribution audits, and feed findings back to physicians — so coding quality compounds into revenue performance, not into silent losses.
Our team delivers 99% claim accuracy, a 95% first-pass acceptance rate, an average 36-day collection cycle, and a 30% reduction in AR days. We onboard in as few as 6 days.
Precision. Progress. Qualigenix.
What’s Next

CMS Prior Authorization Rules: What Every Practice Must Know to Protect Revenue
Prior authorization denial rates jumped 31% in 2026. That number alone should concern every practice manager, hospital administrator, and...
Medical Billing Denial Management in 2026: How Practices Are Fighting Back
Medical Billing Denial Management in 2026: How Practices Are Fighting Back Claim denial rates jumped to 10–15% industry-wide in...
CMS Prior Authorization Rules 2026: Stop Losing Revenue to Preventable Denials
Prior authorization denials jumped 31% year-over-year in 2026. That number isn’t an anomaly — it’s a signal. The CMS...