Inpatient vs Outpatient Coding: Key Differences Explained
The Qualigenix Editorial Team consists of certified billing and coding experts with over 40 years of experience across 38+ medical specialties. Our content is rigorously researched against CMS, AMA, and payer-specific guidelines to ensure total compliance and accuracy. We apply the same elite standards to our resources as we do our client work, consistently delivering high claim accuracy and significant reductions in AR days.
Inpatient and outpatient coding are not two versions of the same process. They use different CPT code sets, different documentation frameworks, different place-of-service codes that affect reimbursement rates, and different rules for what can be billed on which day. A physician who treats patients in both settings and applies one framework to the other produces billing errors in both directions: revenue loss from undercoding where the inpatient code set allows more, compliance risk from applying outpatient logic to inpatient encounters, and incorrect reimbursement from wrong place-of-service coding. The differences are not minor. They affect every claim.
Every physician who practices medicine in more than one setting, the office, the hospital floor, the emergency department, the ambulatory surgery center is operating under a different billing framework in each one. The patient may have the same insurance. The physician may be performing the same clinical work they perform in other settings. But the codes, the documentation standards, the claim forms, the reimbursement rates, and the rules governing what can be billed all change depending on where the service is delivered.
This is not an administrative technicality. It is a structural feature of how the billing system works, and misunderstanding it produces real revenue consequences. A physician who bills an outpatient office visit code for a service delivered in an inpatient hospital room has made a place-of-service error and a code set error simultaneously. A coder who applies 2021 outpatient E/M time-based selection logic to an inpatient subsequent care encounter has applied the wrong selection criteria. Both errors cost money or create compliance risk, and both are common in practices that move between settings without a clear framework for which rules apply where.
This blog explains the key differences between inpatient and outpatient coding across every dimension that affects how a claim is built and how much it pays.
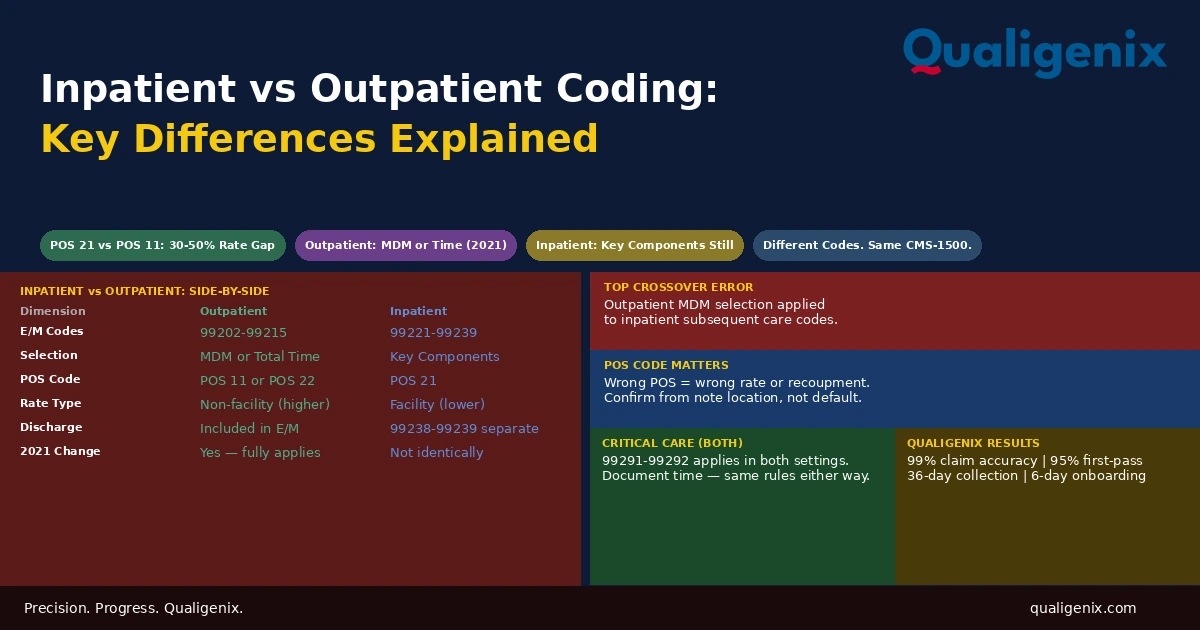
Inpatient coding for physicians uses CPT codes 99221-99223 for hospital admission, 99231-99233 for daily subsequent visits, and 99238-99239 for discharge, with code selection based on key component documentation. Outpatient coding uses CPT codes 99202-99215 for office visits, with code selection based on medical decision making or total time under 2021 AMA guidelines. Both use the CMS-1500 form under the physician’s NPI, but different place-of-service codes apply: POS 21 for inpatient, POS 11 for office, and POS 22 for outpatient hospital, each triggering a different fee schedule reimbursement rate.
The Master Comparison: Inpatient vs Outpatient Physician Coding
| Dimension | Outpatient (Office) | Inpatient (Hospital) |
|---|---|---|
| Physician claim form | CMS-1500 | CMS-1500 |
| Billed under | Physician individual NPI | Physician individual NPI |
| Medicare program | Part B | Part B (physician); Part A (facility) |
| Place of service code | POS 11 (office) or POS 22 (outpatient hospital) | POS 21 |
| Fee schedule rate | Non-facility (higher) for POS 11 | Facility (lower) |
| E/M code set (new patients) | 99202–99205 | 99221–99223 (admission) |
| E/M code set (established/daily) | 99212–99215 | 99231–99233 (subsequent) |
| Discharge/end of encounter | Included in E/M; no separate code | 99238–99239 (discharge day) |
| Critical care | 99291–99292 (if criteria met) | 99291–99292 (if criteria met) |
| E/M code selection basis (2026) | MDM complexity or total time (2021 AMA) | Key components: history, exam, MDM |
| Documentation standard | MDM or time-based per 2021 AMA guidelines | Key component documentation |
| Global period rules | Applies for office procedures | Applies for inpatient surgery |
| Same-day admission and discharge | N/A | Bill initial hospital care only (99221-99223) |
| Concurrent care | Rarely applicable | Common; each specialist bills own E/M |
| Facility billing (separate) | Not applicable for office; UB-04 for outpatient hospital | Hospital bills UB-04 under facility NPI |
Why the Claim Form Is the Same but Everything Else Differs
Both inpatient and outpatient physician professional services are submitted on the CMS-1500 claim form under Medicare Part B. This is the point of similarity that sometimes leads practices to treat inpatient and outpatient billing as interchangeable. The form is the same. The NPI is the same. The payer is the same. But the code, the documentation, the place-of-service indicator, and the reimbursement rate are all different, and the differences are not marginal.
The place-of-service code is the field that carries the most immediate financial consequence. POS 11 (office) triggers the non-facility fee schedule rate. POS 21 (inpatient hospital) and POS 22 (outpatient hospital) trigger the facility rate. The gap between the non-facility and facility rate for the same CPT code ranges from 30% to 50% depending on the service. A physician who uses POS 11 for services delivered in a hospital is paid at the higher non-facility rate, which is both a billing error and an overpayment that CMS will recoup during audit.
The place-of-service code is not a minor field. It determines the fee schedule rate applied to every service on the claim. A physician with a mixed practice seeing both office patients and hospital patients must ensure the correct POS code is applied to each claim, every time. The most common place-of-service error in multi-setting practices is office visit codes billed at POS 11 for encounters that took place in a hospital outpatient department or on an inpatient floor. The claim submits, the payment arrives at the wrong rate, and no denial flags the discrepancy.
The E/M Code Sets: A Detailed Comparison
The clearest structural difference between inpatient and outpatient physician coding is the E/M code set. These are not interchangeable. Using an outpatient code for an inpatient encounter, or vice versa, produces a code that either doesn’t match the service delivered or doesn’t match the place of service on the claim.
Outpatient Office E/M Codes
Outpatient office visits use codes in the 99200 series. New patient visits range from 99202 (straightforward complexity) to 99205 (high complexity). Established patient visits range from 99212 (straightforward) to 99215 (high complexity). Code selection since the 2021 AMA guideline revision is based on either medical decision making (MDM) complexity across three elements problems addressed, data reviewed, and risk or total time spent on the date of the encounter by the billing physician.
The 2021 changes were significant. The prior requirement to document specific history and examination components to justify code levels was eliminated for most outpatient office visits. Physicians can now select the level entirely based on MDM or time. This reduces documentation burden for outpatient visits and aligns code selection with clinical complexity rather than note length.
Inpatient Hospital E/M Codes
Inpatient hospital visits use a completely different code series. The initial visit on the day of admission uses 99221, 99222, or 99223. Each subsequent day uses 99231, 99232, or 99233. The discharge day uses 99238 or 99239. These are not interchangeable with outpatient codes and must not be billed in outpatient settings.
Code selection for inpatient E/M codes uses the traditional key component framework: history, physical examination, and medical decision making. This framework was not replaced by the 2021 outpatient E/M changes for the inpatient code set. Initial hospital care requires all three key components documented at the highest level supporting the code. Subsequent care requires at least two of three. A physician who carries over their outpatient MDM-only documentation approach to inpatient notes may be under-documenting the history and exam components needed to support the inpatient code level.
| Setting | Code Range | Selection Basis | 2021 AMA Changes Apply? |
|---|---|---|---|
| Office (new patient) | 99202–99205 | MDM or total time | Yes |
| Office (established patient) | 99212–99215 | MDM or total time | Yes |
| Inpatient admission | 99221–99223 | All 3 key components | Not identically |
| Inpatient subsequent visit | 99231–99233 | 2 of 3 key components | Not identically |
| Inpatient discharge | 99238–99239 | Time (30 min threshold) | Partial |
| Critical care (either setting) | 99291–99292 | Documented time | N/A — separate framework |
| Observation (initial) | 99221–99223 | Key components | Not identically |
| Observation (subsequent) | 99224–99226 | Key components | Not identically |
Facility Coding: A Separate System Running in Parallel
Beyond physician professional billing, hospital settings generate a parallel stream of facility claims. Understanding this parallel system helps clarify why the physician’s bill and the hospital’s bill are separate and why they follow different rules.
In the inpatient setting, the hospital bills under Part A on the UB-04 claim form using ICD-10-PCS procedure codes for surgeries and interventions. The hospital’s payment is determined by the Diagnosis Related Group (DRG) assigned based on the principal diagnosis, secondary diagnoses that are complications or comorbidities (CCs and MCCs), and procedures performed during the stay. The physician has no role in facility DRG coding and receives no portion of the DRG payment.
In the outpatient hospital setting, the facility also bills on the UB-04, but using CPT codes and Ambulatory Payment Classification rates rather than DRGs. When a physician performs a procedure in a hospital outpatient department, the hospital bills the facility component on the UB-04 and the physician bills the professional component on the CMS-1500. The patient receives two separate bills from the same encounter.
Warning: Physicians who work in hospital settings sometimes assume their documentation feeds into the facility billing system and affects DRG assignment. It doesn’t, directly. Hospital coding is performed by facility coders from the medical record, not from physician billing submissions. However, the physician’s documentation in the medical record absolutely affects the quality of facility coding. If a physician documents a diagnosis that qualifies as a major complication or comorbidity but uses an unspecified code that doesn’t capture the severity, the facility coders may miss the CC/MCC designation and the hospital’s DRG payment is reduced. Physician documentation quality has indirect but real facility revenue consequences.
Place-of-Service Codes: The Revenue Switch Most Practices Miss
The place-of-service code on the CMS-1500 is a two-digit field that tells the payer where the physician delivered the service. It is one of the most consequential fields on the claim because it determines which fee schedule rate the payer applies. The rate difference between the non-facility and facility rates for the same service can be substantial.
| POS Code | Setting | Rate Type | Rationale |
|---|---|---|---|
| 11 | Office or clinic | Non-facility (higher) | Physician bears overhead costs |
| 21 | Inpatient hospital | Facility (lower) | Hospital receives Part A payment |
| 22 | Outpatient hospital | Facility (lower) | Hospital receives outpatient facility payment |
| 23 | Emergency department | Facility (lower) | Hospital receives ED facility payment |
| 24 | Ambulatory surgery center | Facility (lower) | ASC receives facility payment |
| 02 | Telehealth (off-site) | Facility (lower in most cases) | CMS telehealth payment rules apply |
| 10 | Telehealth (patient’s home) | Non-facility in some scenarios | Post-PHE telehealth flexibility rules |
For a physician who delivers a service in both office and outpatient hospital settings, the POS code determines whether they receive the non-facility or facility rate. There is no correct answer that maximizes reimbursement: the POS code must accurately reflect where the service was actually delivered. Using POS 11 for a service delivered in a hospital outpatient department is an error, even though it would produce higher payment. It is an overpayment that the payer can recoup.
The specific situation where POS errors are most common is physicians who have practices in both a private office and a hospital-affiliated clinic or outpatient department. The two locations look similar in daily workflow. The billing difference is substantial. A process that confirms the POS code based on the location documented in the note, not from a default setting in the billing software, is the control that prevents systematic POS errors in multi-site practices.
Documentation Standards: The 2021 Asymmetry
One of the less-understood differences between inpatient and outpatient physician coding is the documentation standard that drives code selection. The 2021 AMA E/M guideline revision changed how outpatient office visit codes are selected. It did not change the inpatient code set in the same way.
For outpatient office visits, the 2021 guidelines allow code selection based entirely on MDM complexity (assessed across problems, data, and risk) or based on total time spent on the date of the encounter. History and exam components no longer determine the code level for most outpatient visits. A physician documenting a complex outpatient encounter does not need to enumerate examination elements to support 99215. MDM complexity or 40-plus minutes of total time is sufficient.
For inpatient initial and subsequent hospital care, the key component framework still applies. All three components history, physical examination, and medical decision making, remain relevant to code selection. Initial hospital care requires all three at the highest level that supports the code. Subsequent care requires at least two of three. A physician who has internalized MDM-only documentation for outpatient encounters and applies the same approach to their inpatient notes may be under-documenting the history and exam elements that help support the inpatient code level.
The documentation asymmetry between outpatient and inpatient coding is one of the most common sources of inpatient undercoding in physician practices with mixed settings. A hospitalist who learned outpatient E/M coding under the 2021 guidelines documents MDM and time for outpatient visits. When they document inpatient notes in the same way, the history and exam documentation that still supports inpatient code selection may be thin or absent. The clinical complexity is there. The documentation to support the highest defensible code level isn’t, because the selection framework they’re using for that note was designed for a different setting.
What Changes for Specific Physician Roles
The inpatient-outpatient coding distinction plays out differently depending on the physician’s practice model and where they spend their clinical time.
Primary Care Physicians
Primary care physicians who make hospital rounds for their own patients are moving between outpatient coding (office visits) and inpatient coding (hospital visits) in the same day. The transition between code sets must be clean. A morning hospital rounding visit for an admitted patient uses inpatient codes with key component documentation. An afternoon office visit for a different patient uses outpatient codes with MDM or time-based selection. The billing system must correctly attribute each encounter to its setting and apply the correct code set and POS code accordingly.
Hospitalists
Hospitalists work exclusively in the inpatient setting, so the inpatient-outpatient distinction matters for them primarily in the context of the hospital’s billing rather than their own. However, hospitalists who practice at facilities that use observation status frequently need to understand the observation coding rules as a third framework sitting between inpatient and outpatient.
Related: Inpatient Coding for Physicians
Surgeons
Surgeons operate in both settings: office consultations and pre-operative visits are outpatient, the surgical procedure and post-operative inpatient care are inpatient, and follow-up visits during the global period may be either. Managing the global period rules correctly across both settings — knowing which post-op visits are bundled and which new-problem visits are separately billable with modifier 24 — is the core coding challenge for surgical practices. Related: Outpatient Coding Accuracy at Scale
Consulting Specialists
A cardiologist, nephrologist, or infectious disease specialist may provide consults in both the inpatient and outpatient settings. The initial consult in an outpatient clinic uses office E/M codes. The same specialist’s initial consult at the bedside uses inpatient initial hospital care codes. Subsequent visits in each setting use the respective code set for that setting. The distinction matters and the billing system must be configured to apply the correct codes based on the documented location of each encounter.
Critical Care: The Code That Crosses Both Settings
Critical care coding (99291-99292) applies in both inpatient and outpatient settings when the clinical criteria are met. It is one of the few code categories that operates the same way regardless of the patient’s admission status because it is defined by the patient’s clinical condition and the physician’s direct management involvement rather than by the administrative setting.
CPT 99291 covers the first 30 to 74 minutes of critical care time per calendar day. CPT 99292 covers each additional 30 minutes. The requirements are the same in an intensive care unit and in an emergency department: critically ill or injured patient, high-complexity decision making to manage life-threatening conditions, direct physician involvement, and documented time.
Critical care replaces the standard E/M code for that encounter. A physician does not bill both 99233 and 99291 for the same visit. When critical care criteria are met and time is documented, 99291 is the appropriate code. When they are not met, the appropriate inpatient subsequent care code is used. The decision between them is clinical, not administrative.
The Crossover Errors That Cost the Most
When practices don’t clearly distinguish inpatient from outpatient coding rules, specific and predictable errors occur. Understanding the pattern allows practices to build the process controls that prevent them.
The first is billing outpatient office E/M codes for inpatient encounters. A physician who bills 99213 or 99214 for a patient they saw on an inpatient hospital floor has used the wrong code set and the wrong place-of-service code. The payment may come back at the office rate rather than the facility rate, but the code itself is incorrect and creates compliance exposure in post-payment audit.
The second is applying 2021 outpatient time-based selection to inpatient daily visits. A physician who bills 99232 because they spent 30 minutes with the patient is using a time-based selection logic that doesn’t apply to subsequent hospital care codes. The subsequent care code level is based on key components, not time. Time-based selection for inpatient visits applies to discharge codes and critical care, not to daily rounding visits.
The third is using the wrong POS code. POS 11 for a hospital encounter, or POS 21 for an office encounter, both create incorrect reimbursement: overpayment in one direction, underpayment in the other. Neither is acceptable.
The fourth is billing the same code for both admission and discharge on a same-day admission and discharge. When a patient is admitted and discharged on the same calendar day, only the initial hospital care code is billed. Billing both an initial care code and a discharge code for the same patient on the same day is duplicate billing.
How Qualigenix Manages Both Coding Frameworks
At Qualigenix, we manage physician billing across inpatient and outpatient settings with a single standard: the correct code, with the correct documentation support, with the correct place-of-service code, submitted to the right payer. That sounds simple. In practices with physicians moving between settings, it requires a billing infrastructure that correctly identifies the setting for each encounter and applies the appropriate framework automatically rather than relying on the physician to specify it.
We configure billing workflows that map encounter locations to the correct POS codes, apply the correct E/M code set based on the setting, and flag crossover scenarios same-day encounters in multiple settings, same-day admission and discharge, critical care eligibility in either setting — for coding review before submission.
We also run monthly code distribution reports across both settings, identifying physicians whose inpatient and outpatient coding patterns suggest framework crossover errors or systematic undercoding in either setting. The reports surface the pattern. Targeted chart reviews confirm it. Physician-specific feedback corrects it prospectively.
Related: What Is Physician Billing | What Is RCM in Medical Billing | Provider Credentialing
Inpatient vs Outpatient Coding Accuracy Checklist
- Patient admission status confirmed before coding each hospital encounter
- Correct E/M code set applied: 99202-99215 for outpatient, 99221-99239 for inpatient
- Outpatient code selection based on MDM or total time per 2021 AMA guidelines
- Inpatient code selection based on key components: history, exam, and MDM
- Place-of-service code confirmed to match documented service location before submission
- POS 11 used only for office-based services where physician bears overhead
- POS 21 used for all inpatient hospital physician professional services
- POS 22 used for outpatient hospital department physician services
- Critical care eligibility assessed in both settings; time documented when applicable
- Same-day admission and discharge billed with initial hospital care code only
- Global period tracked across both inpatient and outpatient post-op visits
- Modifier 24 applied for new unrelated E/M visits during surgical global period
- Monthly code distribution audits run per physician per setting
Frequently Asked Questions: Inpatient vs Outpatient Coding
What is the difference between inpatient and outpatient coding?
Inpatient coding uses CPT codes 99221-99239 for physician hospital services with key component documentation. Outpatient coding uses CPT codes 99202-99215 for office visits with MDM or time-based selection under 2021 AMA guidelines. Both use the CMS-1500 form but different place-of-service codes that trigger different fee schedule rates. The documentation standards, code selection logic, and reimbursement structures differ substantially between the two settings, and applying one framework to the other creates billing errors in both directions.
How do outpatient E/M codes differ from inpatient E/M codes?
Outpatient E/M codes 99202-99215 are selected based on MDM complexity or total time under the 2021 AMA revision. Inpatient codes 99221-99233 still use the key component framework requiring documentation of history, examination, and medical decision making. A physician who applies 2021 outpatient time-based selection to inpatient daily visits is using the wrong selection criteria. The 2021 changes applied to outpatient office visits, not to the inpatient subsequent care code set.
What is a place of service code and how does it differ between settings?
A POS code identifies where a physician delivered a service and determines the fee schedule rate applied. POS 11 is office (non-facility, higher rate). POS 21 is inpatient hospital (facility, lower rate). POS 22 is outpatient hospital (facility, lower rate). The rate difference between facility and non-facility for the same CPT code can be 30% to 50%. Using POS 11 for a hospital-delivered service is an overpayment error CMS recoupts in audit. Using POS 21 for an office-based service is an underpayment that reduces revenue permanently.
Does facility coding differ between inpatient and outpatient settings?
Yes. Inpatient facility coding uses ICD-10-PCS codes on the UB-04, with payment determined by DRG assignment. Outpatient facility coding uses CPT codes on the UB-04, with payment following Ambulatory Payment Classifications. Neither affects the physician’s professional billing directly. However, physician documentation quality influences facility DRG coding indirectly. An unspecified diagnosis code in the physician’s note may cause facility coders to miss a CC or MCC designation, reducing the hospital’s DRG payment even though the physician’s own billing was unaffected.
Can a physician bill both inpatient and outpatient codes on the same day?
Generally no — not for the same patient. A physician may bill an outpatient code for one patient and an inpatient code for a different patient on the same day, but cannot bill both for the same patient. If a patient is admitted and discharged on the same day, only the initial hospital care code (99221-99223) is billed, not both an admission code and a discharge code. If a patient transitions from outpatient to inpatient on the same day, the admission code is billed rather than the outpatient visit code.
How does reimbursement differ between inpatient and outpatient physician services?
Medicare pays the non-facility rate (higher) when the physician delivers services in their own office (POS 11) and the facility rate (lower) when services are in a hospital setting (POS 21 or 22). The rate difference is 30% to 50% for many CPT codes. This is not a penalty for hospital-based physicians — it reflects the fact that the hospital receives a separate payment for overhead. What practices must avoid is billing the non-facility rate for hospital-delivered services, which constitutes an overpayment that payers recoup during audit.
What are the most common coding errors when moving between settings?
The most common crossover errors are using outpatient E/M codes for inpatient encounters, applying 2021 outpatient time-based selection to inpatient daily visits, using the wrong POS code for the service location, billing both initial and discharge codes for same-day admission and discharge, and missing critical care coding opportunities in inpatient settings by defaulting to subsequent care codes. All are systematic in practices with physicians across multiple settings and all require specific process controls not just coder training to prevent reliably.
Related Resources from Qualigenix
- Inpatient Coding for Physicians: What Changes
- Outpatient Coding Accuracy at Scale
- What Is Physician Billing
- What Is RCM in Medical Billing
- Charge Capture for High-Volume Specialties
- Provider Credentialing Services
- AMA CPT E/M Guidelines (AMA-ASSN.org)
Right Codes in the Right Setting. Every Claim.
Qualigenix manages physician billing across inpatient and outpatient settings for practices across 38+ specialties. We apply the correct code set, correct POS code, and correct documentation standard to every encounter so setting transitions never produce billing errors.
Our team delivers 99% claim accuracy, a 95% first-pass acceptance rate, an average 36-day collection cycle, and a 30% reduction in AR days. We onboard in as few as 6 days.
Precision. Progress. Qualigenix.
What’s Next

CMS Prior Authorization Rules: What Every Practice Must Know to Protect Revenue
Prior authorization denial rates jumped 31% in 2026. That number alone should concern every practice manager, hospital administrator, and...
Medical Billing Denial Management in 2026: How Practices Are Fighting Back
Medical Billing Denial Management in 2026: How Practices Are Fighting Back Claim denial rates jumped to 10–15% industry-wide in...
CMS Prior Authorization Rules 2026: Stop Losing Revenue to Preventable Denials
Prior authorization denials jumped 31% year-over-year in 2026. That number isn’t an anomaly — it’s a signal. The CMS...