What Is Aging Accounts Receivable in Medical Billing
The Qualigenix Editorial Team consists of certified billing and coding experts with over 40 years of experience across 38+ medical specialties. Our content is rigorously researched against CMS, AMA, and payer-specific guidelines to ensure total compliance and accuracy. We apply the same elite standards to our resources as we do our client work, consistently delivering high claim accuracy and significant reductions in AR days.
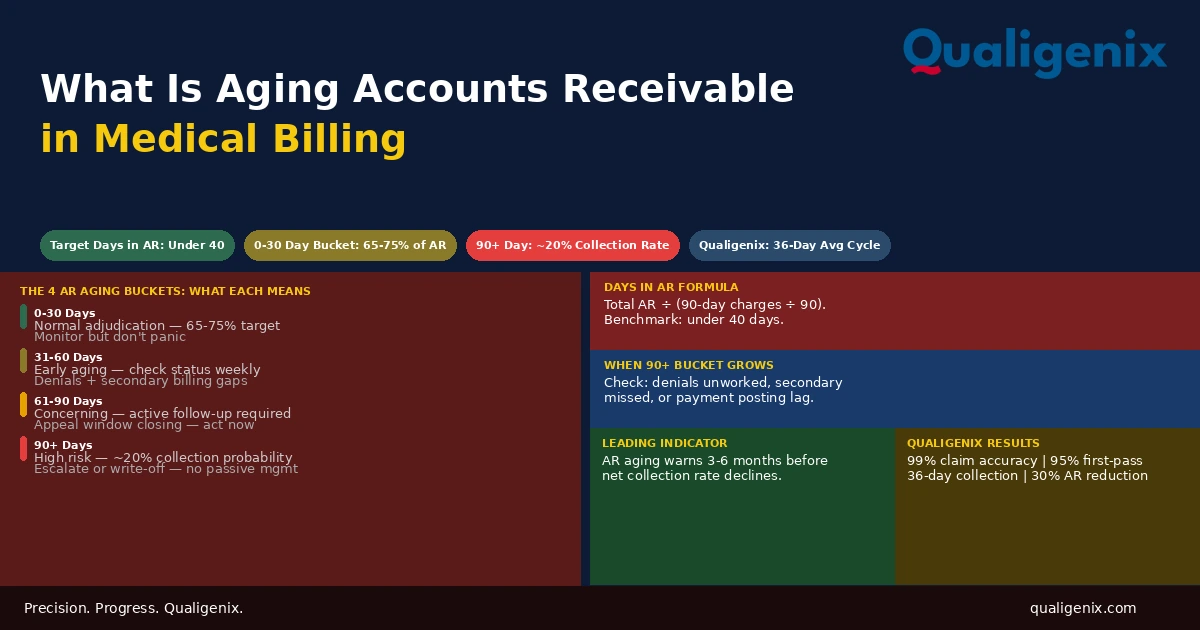
Aging accounts receivable is the financial picture of revenue owed but not yet collected, organized by how long it has been waiting. The AR aging report divides outstanding balances into time buckets 0-30, 31-60, 61-90, and 90-plus days, the distribution of AR across those buckets tells a practice more about the health of its revenue cycle than almost any other single metric. AR concentrated in the 0-30 bucket is normal and expected. AR accumulating in the 60-plus and 90-plus buckets is a signal: claims are being denied and not worked, secondary billing is being missed, payment posting is delayed, or follow-up isn’t happening before accounts cross the threshold where collection probability drops to roughly 20%. Understanding what the aging report shows and acting on it before AR ages past the recovery window is the difference between a revenue cycle that collects what it earns and one that writes off what it couldn’t get to in time.
Accounts receivable is the money a practice has earned but not yet collected. It represents the full universe of services delivered, claims submitted, and revenue awaiting payment from insurance companies and patients. Every practice has AR. The question that determines financial health is not whether AR exists but how it is distributed across time.
A practice where 70% of AR is in the 0-30 day bucket is a practice with a healthy revenue cycle where most claims are in normal adjudication and payments are arriving on schedule. A practice where 30% of AR is in the 90-plus day bucket is a practice with a significant and compounding problem: three months of revenue sitting in accounts with a collection probability of approximately 20%, accumulating toward write-off while the billing team is managing current claims without enough capacity to address what already aged.
The AR aging report is the diagnostic tool that reveals which situation a practice is in. Most practices generate it. Fewer practices read it correctly and act on it consistently enough to prevent the 90-plus bucket from growing quarter over quarter. This blog explains what aging AR is, how the aging report works, what each bucket indicates, how days in AR is calculated and what it means, and what the distribution of AR across buckets tells practice leadership about the specific billing failures driving the problem.
Aging accounts receivable in medical billing refers to outstanding insurance and patient balances organized by how long they have been unpaid, reported in time buckets of 0-30, 31-60, 61-90, and 90-plus days. In a healthy revenue cycle, 65% to 75% of AR should be in the 0-30 day bucket and less than 10% in the 90-plus bucket. When these benchmarks are exceeded, the AR aging report identifies where the collection failure is concentrated and at which payers, providing the roadmap for recovery.
Aging AR Benchmarks and Warning Levels
| Metric | Healthy Benchmark | Warning Level | Critical Level |
|---|---|---|---|
| Days in AR | Under 40 days | 40 to 50 days | Above 50 days |
| AR in 0-30 day bucket | 65% to 75% of total AR | 55% to 64% | Below 55% |
| AR in 31-60 day bucket | Under 15% of total AR | 15% to 20% | Above 20% |
| AR in 61-90 day bucket | Under 8% of total AR | 8% to 12% | Above 12% |
| AR in 90-plus day bucket | Under 10% of total AR | 10% to 20% | Above 20% |
| Net collection rate | 95% or higher | 90% to 94% | Below 90% |
| Clean claim rate | 95% or higher | 90% to 94% | Below 90% |
| Collection probability — AR past 90 days | N/A — prevent | ~20% without active follow-up | ~10% past 120 days |
| AR review frequency — billing team | Weekly | Biweekly | Monthly or less |
| Qualigenix average collection cycle | 36 days | N/A | N/A |
| Qualigenix AR days reduction for clients | 30% improvement | N/A | N/A |
What Accounts Receivable Is and How It Ages
Accounts receivable represents every balance owed to the practice that hasn’t been collected yet. It begins the moment a service is delivered and a claim is generated. From that point, the balance sits in the AR ledger as an asset money the practice has earned and expects to collect until one of three things happens: the payer pays the claim, the balance is adjusted off as a contractual write-down, or the balance is written off as uncollectable.
AR “ages” in the most literal sense: it gets older. Every day that passes between the date of service and the date of payment adds to the age of the account. An account that was 30 days old last week is 37 days old this week. An account that was 75 days old and hasn’t been worked becomes a 90-plus day account that will need escalated recovery effort.
The aging categories matter because collection probability, the likelihood that a balance will ultimately be collected decreases as accounts age. This is not a universal rule; some old accounts are eventually collected. It is a statistical reality. The older an unpaid account, the more likely it is that the claim has been denied without appeal, the patient’s coverage has changed, the timely filing window has closed, or the balance simply falls through the gaps of a billing team with limited follow-up capacity.
The most important thing to understand about aging AR is that it is a lagging indicator. By the time a balance appears in the 90-plus day bucket on this month’s report, the failure that put it there happened 90 days ago, a denial that wasn’t worked, a secondary claim that wasn’t initiated, a charge that wasn’t entered on time. The aging report tells you where problems are accumulating. It doesn’t tell you how to prevent them. Prevention requires tracing each aging account to its root cause and implementing the upstream process fix that stops the same type of account from appearing in the same bucket next quarter.
The AR Aging Report: Structure and What Each Section Shows
The AR aging report is a financial report generated by the practice management or billing system that shows all outstanding balances organized by aging bucket. Most reports are presented in two dimensions: rows by payer or patient, and columns by time bucket. The intersection of each row and column shows the dollar amount outstanding at that payer in that time range.
A standard AR aging report for a medical practice shows insurance AR, outstanding balances on submitted claims awaiting payer adjudication and patient AR outstanding balances on billed patient responsibilities after insurance has processed. These two categories have different causes, different follow-up workflows, and different collection challenges. Most billing software allows filtering to view each separately.
Insurance AR by Payer and Bucket
Insurance AR sorted by payer reveals which payers are generating disproportionate aging. When a specific payer has unusual concentration in the 61-90 or 90-plus bucket relative to the volume of claims submitted to that payer, it indicates a systemic issue: a recurring denial category at that payer not being worked, a credentialing or enrollment gap causing claims to be rejected, or a payer with unusually slow adjudication that requires active follow-up to advance.
Payer-level aging analysis is the diagnostic tool that converts “we have too much old AR” into “Blue Shield has 40% of our 90-plus bucket and we submitted only 18% of our claims to them.” That asymmetry has a specific cause. Finding it a denial category specific to that payer, an enrollment issue, a fee schedule dispute and fixing it prevents the pattern from repeating next month while the team works through the current backlog.
Patient AR by Bucket
Patient AR ages differently from insurance AR. Insurance AR is driven by claim adjudication, denial management, and follow-up. Patient AR is driven by patient responsibility that wasn’t collected at the time of service, patient billing that wasn’t generated promptly after insurance processing, and patient communication that wasn’t consistent enough to collect the balance before it aged.
Patient AR in the 60-plus bucket typically indicates one or more of: patient statements that were generated late, patient balance that is higher than the patient can pay without a payment plan, patient who has moved or changed contact information without notifying the practice, or a disputed balance where the patient believes insurance should have paid more. Each requires a different resolution pathway, and a blanket follow-up approach that treats all patient AR the same way produces lower recovery rates than a segmented approach that distinguishes between these categories.
Days in AR: How to Calculate It and What It Means
Days in AR is the summary metric that reflects the overall performance of the revenue cycle at collecting what it bills. It is calculated as follows:
Days in AR = Total Outstanding AR ÷ (Total Charges over Last 90 Days ÷ 90)
This formula produces the average number of days from service delivery to payment receipt across the full AR portfolio. If a practice has $600,000 in total outstanding AR and generates $15,000 in charges per day (calculated from 90-day trailing charge data), the days in AR is 40 exactly at the benchmark.
If the same practice’s AR grows to $900,000 without a proportional increase in daily charges, days in AR rises to 60. That 20-day increase represents $300,000 in AR that is sitting older than it should be. If the average allowed amount per claim is $150, that’s 2,000 claims worth of AR that has accumulated beyond where it should be each one representing a payment that is either delayed, denied and unworked, or approaching the write-off threshold.
What Causes Days in AR to Rise
Days in AR rises when the rate at which AR is being resolved slows relative to the rate at which new AR is being created. The most common causes are:
Clean claim rate declining. When more claims fail payer edits on first submission, they require correction and resubmission before they can adjudicate. The adjudication clock doesn’t start until a clean claim reaches the payer. Each resubmission adds days to the collection timeline for that account.
Denial backlog growing. Denied claims sit in the denial queue aging toward write-off while the billing team manages current submissions. When the denial queue isn’t worked promptly, the oldest denials age past the appeal window and become permanent losses. The accounts they were attached to remain in AR until they are written off, distorting the overall days-in-AR calculation upward.
Payment posting lag. When ERA payments are not posted within 48 hours, accounts that have been paid still appear as outstanding in the AR report. Days in AR reflects artificially high aging because payment exists in the ERA but hasn’t been applied to the account. Payment posting lag distorts the AR aging report in both directions: it makes the overall balance appear higher and makes the distribution appear older than the actual collection timeline warrants.
Secondary billing delays. After primary insurance adjudicates, the secondary billing must be initiated promptly to keep the account moving toward resolution. When secondary billing is delayed, because the billing team didn’t identify secondary coverage, because secondary billing isn’t triggered automatically by the practice management system, or because the secondary claim wasn’t generated until the account entered the aging queue the account sits in AR accumulating days while waiting for a step in the process that was missed.
The AR Aging Buckets: What Each One Tells You
0-30 Days: Normal Adjudication
The 0-30 day bucket contains the current universe of claims in normal adjudication submitted, received by the payer, and being processed according to the payer’s standard timeline. Medicare typically processes clean claims within 14 to 30 days. Most commercial payers process clean claims within 30 days. AR in this bucket does not require active follow-up under normal circumstances. It requires monitoring: confirming that claims are being received and adjudicated on the expected timeline rather than sitting in a pending status.
The health signal in the 0-30 bucket is its share of total AR. In a healthy revenue cycle, 65% to 75% of all outstanding AR should be current. When this percentage falls below 60%, it typically indicates that older AR is accumulating faster than current AR is resolving a sign of compounding collection problems in the older buckets.
31-60 Days: Early Aging Requiring Attention
The 31-60 day bucket contains claims that haven’t resolved in the normal adjudication window. For Medicare, a clean claim not paid within 30 days has either not been received, is in a pending status requiring follow-up, or was denied. For commercial payers, the 31-60 day bucket is where denied claims accumulate when the billing team’s denial management workflow has a backlog, and where secondary billing should be generating activity if primary adjudication completed in the prior period.
Active monitoring of the 31-60 day bucket weekly status checks on claims approaching 45 days catches denial situations before they age further and identifies secondary billing opportunities that need to be acted on before the primary adjudication ages out of the secondary payer’s filing window.
61-90 Days: Concerning — Active Follow-Up Required
The 61-90 day bucket is where revenue cycle problems become urgent. Claims in this range have been outstanding for two to three months. The most common reasons are denials that weren’t appealed during the initial response window, secondary billing that wasn’t initiated after primary adjudication, and credentialing or authorization issues that produced denials requiring escalated resolution.
Warning: Accounts in the 61-90 day bucket are approaching a critical threshold. Commercial payer appeal windows for denied claims are typically 30 to 180 days from the denial date. An account that was denied at 30 days and reaches the 61-90 bucket without being worked has potentially consumed half or more of its appeal window. If the denial isn’t appealed before the window closes, the revenue is permanently lost. Weekly review of the 61-90 bucket with active follow-up on every account is not optional it is the process that keeps collectible revenue from becoming uncollectable.
90-Plus Days: High Risk — Escalated Recovery
The 90-plus day bucket is the revenue cycle’s critical care unit. Accounts here have a collection probability of approximately 20% without active, targeted recovery effort. They represent balances that have passed through the normal follow-up cycle without resolving, and they require a different level of intervention than routine billing follow-up.
For insurance AR in the 90-plus bucket, the options are: late appeal if the payer’s window is still open and the denial is documented, resubmission if the claim hasn’t technically been denied but was simply not followed up, escalated payer contact for accounts where payment status is unclear, or write-off if the account has exhausted all recovery options. For patient AR in the 90-plus bucket, the options are: payment plan offer with documentation of terms, collection agency referral for balances above the practice’s threshold, or financial hardship write-off for qualifying patients.
The 90-plus bucket is also where the AR aging report becomes a management accountability document. When the 90-plus bucket exceeds 20% of total AR, the practice has a write-off liability forming in real time. Every week that the accounts in this bucket go without action, a portion of them crosses from recoverable to unrecoverable. The report identifies the problem. Leadership must ensure the recovery effort is funded and staffed proportionally to the size of the problem.
How to Read the AR Aging Report as a Revenue Cycle Diagnostic
A practice administrator or billing manager who reviews the AR aging report monthly should be asking a series of diagnostic questions, each of which points to a specific process failure that can be addressed.
Is Days in AR Trending Up Over Three Consecutive Months?
A single month of elevated days in AR may reflect a seasonal pattern, a billing system transition, or a temporary staffing gap. Three consecutive months of rising days in AR is a trend that indicates a systemic process failure. Identify the month the trend started, investigate what changed in the billing process around that time, and trace the increase to its root cause: a new payer with slower adjudication, a denial category that grew suddenly, a staff departure that created a backlog, or a documentation change that reduced clean claim rates.
Is the 90-Plus Bucket Growing as a Percentage of Total AR?
The most dangerous AR trend is a 90-plus bucket that is growing as a percentage of total AR month over month. It means that AR is accumulating in the high-risk aging category faster than it is being resolved there. Each month of growth represents more revenue at 20% collection probability. When this trend appears, the 90-plus bucket recovery effort must be scaled up immediately not next month before the next month’s accumulation adds to an already critical backlog.
Which Payers Are Disproportionately Represented in the 60-Plus Buckets?
Payer-level aging analysis identifies whether aging is practice-wide (indicating billing workflow problems) or payer-specific (indicating a targeted issue at specific payers). When a single payer generates 40% of 90-plus bucket AR while representing only 20% of claims volume, the cause is specific to that payer: a denial category, an enrollment issue, a fee schedule dispute, or a claims processing delay. The targeted fix is different from the systemic fix and is more efficiently pursued when identified rather than worked as part of a general AR catch-up effort.
The Connection Between AR Aging and Upstream Billing Performance
AR aging is a downstream outcome metric. It reflects what happened to claims that were submitted weeks and months ago. Improving AR aging requires not just working old accounts but fixing the billing process failures that are continuously generating new ones.
A practice that works its 90-plus bucket aggressively this month, recovers 60% of the accounts, and then generates a new cohort of 90-plus accounts next month because the underlying denial management backlog wasn’t addressed has improved its current AR picture without improving its revenue cycle performance. The work will need to be done again next quarter on the new cohort.
Sustainable AR aging improvement requires connecting the AR aging analysis to upstream process fixes. When the 61-90 bucket is dominated by a specific denial category authorization denials from a specific specialty procedure, coding errors that a scrubber update would catch, eligibility failures from a specific payer’s plan type, the AR aging report is providing the data to implement the upstream fix. Implementing that fix reduces the monthly inflow into the aging queue at the category level, which compounds over time into a lower average days in AR without requiring proportionally more follow-up effort each month.
Related: Denial Management: Common Denials and How to Fix Them | Signs It’s Time to Outsource Claims Processing
How Qualigenix Manages Aging Accounts Receivable
At Qualigenix, AR management is a systematic, scheduled function not a reactive one. We run AR aging reviews every week for every client practice, identifying accounts in the 31-60 bucket approaching the 60-day threshold for active follow-up escalation, working the 61-90 bucket with payer contact and resubmission within 48 hours of the review, and presenting the 90-plus bucket with recovery recommendations which accounts are still within the appeal window, which require payment plans, and which have exhausted all options and should be written off with documentation of the recovery effort.
Our monthly reporting package includes the full AR aging distribution by payer and bucket, days-in-AR trend over the prior six months, net collection rate, and an analysis of which denial categories and payer-level patterns are contributing the most to 60-plus day aging. We review these findings with each practice’s billing liaison on a monthly call and implement the upstream process fixes that prevent recurring aging patterns from generating new cohorts of old AR month after month.
For practices transitioning from in-house billing with elevated 90-plus day AR, our onboarding includes a dedicated aged AR recovery project in the first 90 days that systematically works through the prior billing operation’s backlog while the normal billing cycle is managed under our standard workflow. Practices that transition with significant aged AR typically see meaningful 90-plus bucket reduction within the first quarter.
Our results reflect this systematic approach: 99% claim accuracy rate, 95% first-pass acceptance rate, 36-day average collection cycle, and 30% reduction in AR days for practices transitioning from in-house billing operations. We onboard in as few as 6 days.
Related: What Is RCM in Medical Billing | What Is Claim Submission in Medical Billing | Accounts Receivable Medical Billing: How to Reduce Days in AR
Aging AR Management Checklist
- Days in AR calculated monthly and compared against 40-day benchmark
- Days in AR trend tracked over rolling 6 months — three-month uptrend triggers root cause investigation
- AR aging distribution calculated: 0-30, 31-60, 61-90, 90-plus as percentage of total AR
- 90-plus bucket percentage tracked monthly — above 10% triggers escalated recovery action
- AR aging report sorted by payer to identify disproportionate aging at specific payers
- Billing team reviews and works AR aging queue weekly — not monthly
- 31-60 day accounts receive payer status check and resubmission if needed
- 61-90 day accounts receive active payer follow-up call within 5 business days of entering bucket
- 90-plus accounts reviewed for appeal window status — peer-to-peer or formal appeal initiated if window open
- Payment posting standard maintained at 48 hours to prevent posting lag from distorting AR report
- Secondary billing triggered automatically after primary adjudication — no manual identification required
- Write-off recommendations presented to practice leadership with documentation of recovery steps taken
- Upstream process fixes implemented for recurring aging patterns identified in monthly AR analysis
Frequently Asked Questions: Aging Accounts Receivable
What is aging accounts receivable in medical billing?
Aging accounts receivable is outstanding revenue organized by how long it has been unpaid, reported in time buckets of 0-30, 31-60, 61-90, and 90-plus days. The distribution of AR across these buckets is the most actionable revenue cycle health indicator available. Healthy distribution keeps 65% to 75% of AR in the 0-30 bucket and less than 10% in the 90-plus bucket. Deviations from these targets indicate specific billing process failures that can be identified, traced to their root causes, and corrected through targeted upstream fixes.
What is days in AR and how is it calculated?
Days in AR measures the average number of days from service delivery to payment receipt. It is calculated by dividing total outstanding AR by average daily charges from the prior 90 days. The benchmark is under 40 days. Above 50 days indicates a systemic billing problem. Above 60 days indicates active AR management failure. Three consecutive months of rising days in AR is a trend requiring root cause investigation — not just more follow-up effort on the existing backlog.
What does AR in the 90-plus day bucket indicate?
AR in the 90-plus day bucket indicates accounts outstanding for over three months with a collection probability of approximately 20% without active follow-up. When the 90-plus bucket exceeds 10% to 15% of total AR, the practice has material write-off risk forming in real time. Every account in this bucket needs to be evaluated for appeal window status, payment plan eligibility, or write-off recommendation based on the recovery steps already taken. The 90-plus bucket cannot be managed passively — each week of inaction converts a higher percentage of it from recoverable to unrecoverable.
What causes AR to age in medical billing?
The most common causes of AR aging are claim denials not worked promptly, secondary billing not initiated after primary adjudication, payment posting delays, charge lag delaying initial submission, and insufficient follow-up on accounts approaching the 60-day threshold. Each cause is distinct and requires a different upstream fix. Identifying the specific cause at each payer level not just working old accounts in aggregate is the difference between recovering from the current backlog and preventing the next one.
How often should a practice review its AR aging report?
The billing team should work the AR aging queue weekly. Practice leadership or the billing manager should review the AR aging report monthly to monitor distribution trends and days-in-AR movement. Weekly working ensures accounts approaching the 60-day and 90-day thresholds receive follow-up before they age further. Monthly review identifies whether the distribution is improving or deteriorating over time and whether days in AR is trending in the right direction. Monthly review without weekly working is analysis without execution — it identifies the problem but doesn’t address it.
What is the connection between AR aging and net collection rate?
AR aging distribution is a leading indicator of net collection rate. When AR accumulates in the 90-plus bucket, those accounts are at high write-off risk and write-offs reduce net collection rate. Monitoring AR aging monthly provides three to six months of earlier warning of a declining net collection rate compared to waiting for the collection rate itself to fall. Practices that act on aging distribution deterioration when it appears in the 60-plus bucket prevent the write-offs that eventually show up as a lower net collection rate on their financial statements.
Related Resources from Qualigenix
- Denial Management: Common Denials and Fixes
- Signs It’s Time to Outsource Claims Processing
- What Is Physician Billing
- Provider Credentialing Services
- Contact Qualigenix Healthcare
Old AR Is Revenue That Didn’t Have to Be Lost. We Recover It.
Qualigenix manages accounts receivable for practices across 38+ specialties — weekly AR aging reviews, systematic follow-up by bucket, 90-plus day recovery projects for practices transitioning from in-house billing, and the upstream process fixes that prevent new aging cohorts from forming month after month.
Our team delivers 99% claim accuracy, a 95% first-pass acceptance rate, an average 36-day collection cycle, and a 30% reduction in AR days. We onboard in as few as 6 days.
Precision. Progress. Qualigenix.
What’s Next

Medical Coding Errors That Cost Practices the Most (And How to Catch Them Before They Submit)
Medical Coding Errors That Cost Practices the Most (And How to Catch Them Before They Submit) Written by the...
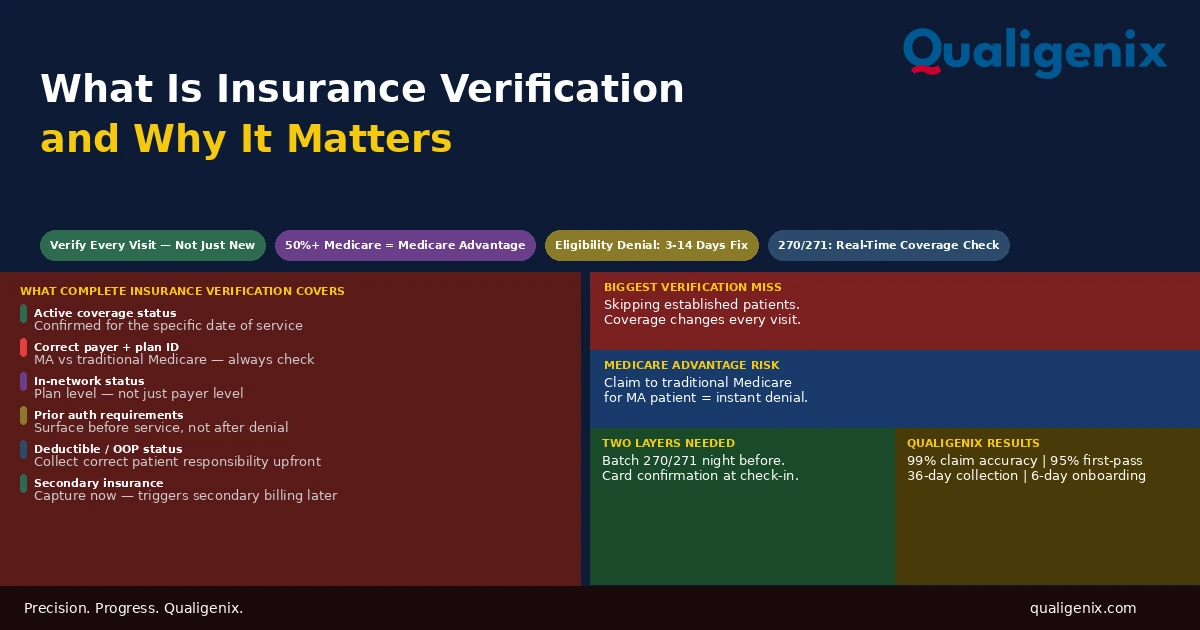
What Is Insurance Verification and Why It Matters
Insurance verification is the front-end process that determines whether a claim will be paid before the patient ever enters...

Insurance Denial Appeals: What Practices Miss
Most insurance denial appeals that fail don’t fail because the clinical case was weak. They fail because the...