Outsource Claims Processing: What Changes for Your Practice
The Qualigenix Editorial Team consists of certified billing and coding experts with over 40 years of experience across 38+ medical specialties. Our content is rigorously researched against CMS, AMA, and payer-specific guidelines to ensure total compliance and accuracy. We apply the same elite standards to our resources as we do our client work, consistently delivering high claim accuracy and significant reductions in AR days.
When a practice outsources claims processing, the billing administration moves to the partner but the clinical and registration inputs that make billing work stay with the practice. Documentation quality, accurate insurance data capture at the front desk, and timely responses to coding queries remain the practice’s responsibility regardless of who submits the claims. What changes is everything downstream of those inputs: coding, claim construction, scrubbing, submission, payment posting, denial management, secondary billing, and AR follow-up all become the partner’s operational function. The practice’s job shifts from managing a billing operation to reviewing performance reports and maintaining the clinical and registration quality that feeds one. This is a meaningful operational change. Understanding it clearly before transitioning prevents the most common outsourcing disappointment, expecting the partner to improve outcomes that depend on practice-side inputs the partner cannot control.
The decision to outsource claims processing is often made in response to a performance problem rising denials, aging AR, billing staff turnover and the expectation that follows is that outsourcing fixes the performance problem. That expectation is correct when the performance problem originates in the billing function. It is incorrect when the performance problem originates in documentation quality, front-desk registration accuracy, or the physician’s completion time for clinical notes. An outsourced claims processing partner is an exceptionally capable billing operation. It is not a substitute for timely, specific physician documentation or accurate patient insurance data capture at the point of registration.
Practices that understand this distinction enter outsourcing transitions with realistic expectations, well-prepared workflows, and a clear picture of what they need to do to make the partnership work. Practices that don’t understand it outsource billing, find that some performance problems persist, and conclude that outsourcing didn’t help when the reality is that outsourcing helped with everything it was responsible for and the remaining problems were never billing problems to begin with.
This blog walks through each stage of the claims processing lifecycle and explains precisely what changes when the function moves to an outside partner, what the practice still owns, and what a well-run outsourced claims processing engagement looks like from the practice’s perspective on a day-to-day and month-to-month basis.
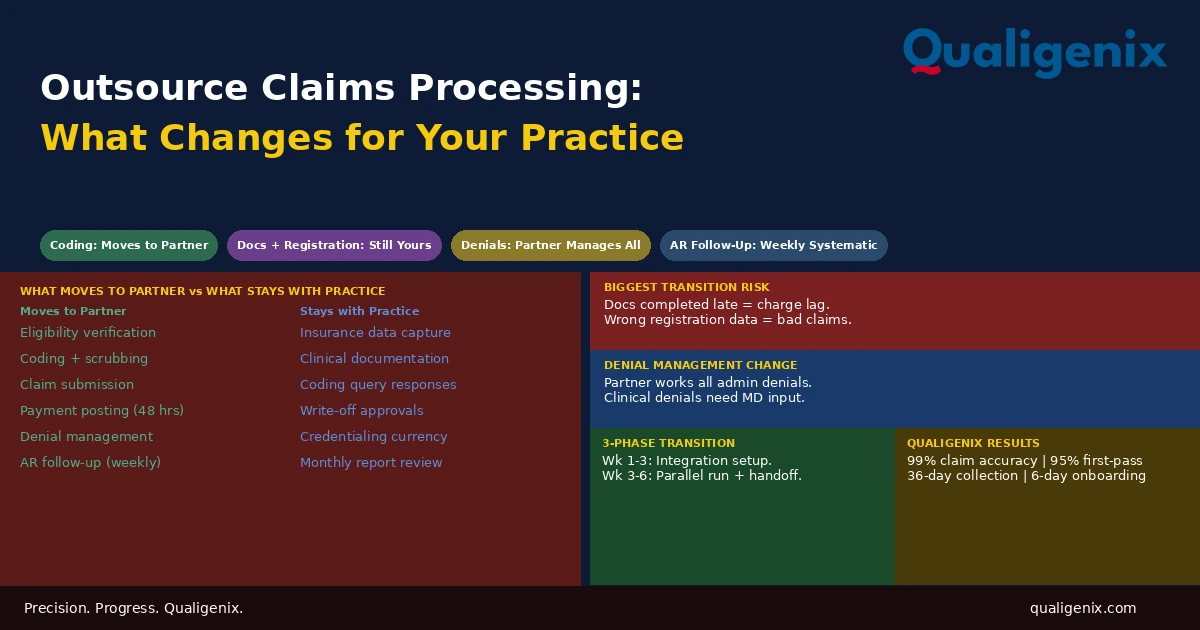
When claims processing is outsourced, the partner takes operational ownership of eligibility verification, charge entry, claim scrubbing and submission, payment posting, denial management, secondary billing, and AR follow-up. The practice retains ownership of clinical documentation quality, accurate registration data capture, coding query responses, and write-off decisions. The practice’s daily billing management workload shifts to reviewing monthly performance reports and maintaining the clinical and registration inputs the partner depends on to process claims correctly.
What Changes and What Doesn’t: The Master Reference
| Claims Processing Function | In-House | Outsourced |
|---|---|---|
| Insurance eligibility verification | Front desk or billing team | Partner — automated pre-visit checks |
| Patient demographic and insurance data capture | Front desk | Still the practice’s front desk |
| Clinical documentation completion | Physician | Still the physician |
| Coding (CPT, ICD-10, modifiers) | In-house coder or biller | Partner’s specialty-trained coders |
| Documentation query resolution | In-house coder to physician | Partner’s coder to physician — still needs physician response |
| Claim construction and scrubbing | In-house billing team | Partner |
| Electronic claim submission | In-house billing team | Partner |
| Payment posting (ERA auto-posting) | In-house billing team | Partner — 48-hour standard |
| Denial management and appeals | In-house billing team | Partner — with clinical input when needed |
| Secondary billing | In-house billing team | Partner |
| Patient statement generation | In-house billing team | Partner |
| AR follow-up on aging accounts | In-house billing team (often ad hoc) | Partner — weekly systematic review |
| Write-off decisions above threshold | Practice administrator | Still practice administrator |
| Performance reporting and analysis | In-house — often incomplete | Partner — monthly standardized reports |
| Credentialing and payer enrollment | Practice manages or outsources separately | Qualigenix includes — others may not |
Stage 1: Eligibility Verification — What Changes
Pre-visit insurance eligibility verification is one of the most consistently under-executed functions in in-house billing operations. The workflow exists in most practices. It is executed inconsistently in most practices — run on some patients, skipped for established patients assumed to have the same insurance as their last visit, and omitted entirely when the front desk is managing a full waiting room.
When claims processing is outsourced, eligibility verification shifts to the partner and becomes a systematic automated function rather than a manual front-desk task. The partner runs 270/271 eligibility transactions against the appointment schedule, typically the evening before or the morning of each day’s schedule and returns a report flagging any patient whose coverage has changed, lapsed, or cannot be confirmed. The practice receives this report before the patients arrive and can take action: verify coverage, collect updated insurance information, or flag the patient for financial counseling.
The piece that doesn’t change is the practice’s responsibility for capturing accurate insurance data at registration. The partner’s eligibility check queries the payer with the member ID and plan information the practice has on file. If that information is wrong the member ID was transposed, the patient switched from a PPO to an HMO and the front desk wasn’t updated, the eligibility check will either return inaccurate results or fail entirely. Eligibility verification is only as good as the data it operates on, and that data comes from the practice’s front desk.
The single most impactful front-end change a practice can make when transitioning to outsourced claims processing is improving the rigor of insurance data capture at registration. Confirming the insurance card at every visit — not just new patients — and updating the system when plans change prevents a significant category of claim failures that no amount of billing expertise downstream can correct once the wrong plan information is on the claim.
Stage 2: Documentation Transmission and Coding — What Changes
In an in-house billing model, the coder (or billing staff performing coding) has physical or system access to the EHR and can review documentation as soon as it is completed. The feedback loop between the coder and the physician is informal and fast, a question can be answered in passing in the hallway.
When coding moves to an outsourced partner, the documentation must be transmitted from the practice’s EHR or practice management system to the partner’s coding platform. This transmission happens through one of three mechanisms: a direct API integration between the EHR and the partner’s platform, an HL7 interface that sends clinical data in a structured format, or a secure file transfer of exported documentation. The transmission method is configured during onboarding and should be tested before the go-live date.
The coding turnaround standard for outsourced coding is 24 to 48 hours from the time complete documentation is received. For the practice, this means physician documentation must be completed and finalized within a defined window after the encounter typically same-day or next-day or the coding timeline extends and charge lag accumulates. Practices where physicians routinely complete notes three to five days after the encounter will find that outsourcing coding doesn’t eliminate charge lag; it relocates the bottleneck from the billing team to the documentation completion step.
The documentation query process changes in character but not in fundamental requirement. When an in-house coder has a documentation question, they ask the physician informally. When the outsourced coder has a documentation question, it comes through a structured query — a formal written request identifying the specific encounter, the specific gap, and the specific information needed to support accurate code assignment. The physician responds within the defined window (typically 24 to 48 hours). If no response is received, the coder codes conservatively to what is documented and marks the encounter as queried-unresolved.
Some physicians experience the formal query process as more burdensome than the informal hallway question. In practice, structured queries are more efficient for the revenue cycle because they create an audit trail, force specificity about what documentation is missing, and generate pattern data that identifies which physicians need documentation improvement coaching. The informality of the in-house query process is a convenience for the physician; the formality of the outsourced query process is a revenue cycle quality control.
Stage 3: Claim Construction, Scrubbing, and Submission — What Changes
This is the stage where the operational change is most complete. In an in-house billing model, building the claim, running it through the scrubber, and submitting it electronically are billing staff functions that happen on whatever schedule the billing team manages. In an outsourced model, this entire stage is the partner’s operational responsibility and happens on a defined schedule that the practice never needs to monitor.
The partner builds each claim from the coded encounter with all required fields: patient demographics, insurance member ID, rendering provider NPI, billing entity NPI and Tax ID, place-of-service code, date of service, CPT codes, ICD-10 codes, modifiers, billed charges, and authorization number where applicable. The claim is then run through the partner’s payer-specific scrubber, which applies the current edit rules for the destination payer. Errors caught by the scrubber are corrected before transmission. Clean claims transmit to the payer through the clearinghouse.
The practice’s interaction with this stage is zero under normal circumstances. The practice didn’t build the claim, didn’t scrub it, and didn’t submit it. The first signal the practice receives about this stage is the monthly reporting that shows the clean claim rate for the period. If the rate is at or above 95%, the stage is performing correctly. If it drops below that threshold, the partner’s account manager communicates the root cause and the corrective action.
Warning: The practice is not removed from responsibility for the inputs to this stage even though it doesn’t manage the stage itself. If the practice’s front desk captured the wrong member ID, if the physician’s documentation didn’t support a specific CPT code, or if a new provider’s NPI isn’t yet enrolled with the payer — the partner will produce a claim from whatever inputs were provided, and the scrubber will catch what it’s configured to catch. Input errors that the scrubber isn’t designed to catch will reach the payer as submitted claim errors. The partner’s process quality is high; it is not a substitute for accurate inputs from the practice side.
Stage 4: Payment Posting — What Changes
Payment posting is one of the most underestimated revenue cycle functions in terms of its downstream consequence. When payment posting is delayed or inaccurate, every function that depends on it — secondary billing, patient balance billing, AR management, and reporting — is delayed or distorted in parallel.
In in-house billing operations, payment posting is often the function most affected by competing workload demands. When a biller is managing denials, submitting new claims, and handling patient phone calls simultaneously, ERA posting gets deferred. Deferred posting means secondary billing doesn’t trigger, patient statements don’t generate, AR balances show as outstanding when payment has been received, and reporting reflects a distorted picture of actual performance.
When claims processing is outsourced, payment posting becomes a defined operational standard: ERA files are received through the clearinghouse and auto-posted within 48 hours of receipt. Standard payment and contractual adjustment transactions post automatically. Denied lines route to the denial management queue. Payments below the expected contractual rate are flagged as potential underpayments for follow-up. The practice’s AR ledger is current within 48 hours of every ERA receipt, without any practice-side action required.
The practice interaction with this stage is limited to reviewing the payment posting section of the monthly report, which shows posting volume, auto-posting rate, underpayment flags generated, and any ERA processing exceptions that required manual handling. In a well-run outsourced engagement, this section of the report confirms that posting is current and accurate rather than requiring any action.
Stage 5: Denial Management — What Changes
Denial management is where the difference between in-house and outsourced claims processing is most practically significant. In-house billing teams frequently manage denials reactively: a denial arrives, a biller reviews it, takes the action the denial code seems to require, and moves on. The pattern data that would reveal that 40 claims per month are denying for the same reason at the same payer — indicating a systemic upstream problem — never gets analyzed because the volume of individual claim work consumes the time that analysis would require.
When claims processing is outsourced, denial management becomes a systematic two-layer function. At the individual claim level, each denial is received, categorized by root cause, routed to the appropriate resolution workflow, and worked within a defined response window. At the pattern level, denial trend data is analyzed monthly to identify systemic issues that require upstream process changes rather than individual claim remediation.
The practice’s involvement in denial management shifts from doing the work to receiving the output. Clinical denials — denials based on medical necessity or requiring peer-to-peer review — require physician involvement that the partner initiates. The partner identifies the denial, determines that physician clinical input is required for the appeal, and sends a structured request to the practice with the relevant documentation and a defined response window. The physician provides the clinical context; the partner builds and submits the appeal.
Administrative denials — wrong place-of-service code, missing modifier, authorization number omitted, eligibility failure — are resolved entirely by the partner without practice involvement. Credentialing denials — provider not enrolled with the payer — require escalation to the credentialing function, which at Qualigenix is managed as part of the same engagement rather than as a separate track.
What the Practice Sees in Denial Management Reporting
The monthly denial management report should show denial volume by reason code and by payer, trend versus prior month, resolution rate and average resolution time, pending appeals by status, and any systemic denial categories that require upstream practice-side changes — documentation improvements, authorization workflow adjustments, or credentialing actions. The report replaces the denial queue that in-house billing staff work from; the practice’s role is to review the report, act on any practice-side items identified, and hold the partner accountable for resolution performance on the items within their control.
Stage 6: Secondary Billing and Patient Statements — What Changes
Secondary billing — billing the patient’s secondary insurance after the primary payer has adjudicated — is a function that in-house billing operations frequently delay or execute inconsistently because it requires active follow-up after primary adjudication rather than being built into the initial claim submission workflow. When primary ERA receipt triggers secondary billing automatically in a well-configured outsourced billing platform, the delay that in-house operations typically produce disappears.
The partner receives the primary payer’s ERA, identifies claims with secondary insurance on file, generates the secondary claim with the primary payer’s EOB attached, and submits it within the same 48-hour posting window. The practice is not involved in this step. The secondary claim is submitted, tracked, and its payment posted by the partner on the same schedule as primary claims.
Patient statements generate after both primary and secondary adjudication are complete and a patient balance is confirmed. The partner generates and sends statements on a defined cycle and tracks patient balance outstanding versus patient balance collected. The practice maintains responsibility for its financial hardship policy and write-off approval for patient balances above the agreed threshold. The partner recommends write-off or collection referral on accounts that exhaust the collection cycle without payment; the practice approves.
Stage 7: AR Follow-Up — What Changes
Accounts receivable follow-up is the function where the difference between systematic outsourced management and ad hoc in-house management produces the largest measurable revenue difference over time. In-house billing teams follow up on aging AR when they have time — which means they follow up inconsistently, prioritize the largest accounts when they do follow up, and allow smaller accounts to age to write-off without sufficient intervention.
When AR follow-up moves to the outsourced partner, it becomes a weekly scheduled function with defined escalation triggers. The partner runs AR aging reviews every week, identifies accounts in the 31-to-60-day bucket approaching the 60-day threshold, and makes follow-up contact — payer call, portal inquiry, or resubmission — on each one. Accounts that reach 60 days without resolution escalate to a dedicated AR follow-up team. Accounts that reach 90 days receive accelerated resolution effort with a write-off or collection referral recommendation if exhausted.
The practice’s involvement in AR management is limited to approving write-off recommendations above the agreed threshold and receiving the monthly AR aging report that shows how AR is distributed across time buckets. For practices transitioning from in-house billing with a significant 90-plus-day AR balance, the partner’s systematic follow-up in the first 90 to 120 days of the engagement typically produces a notable recovery of aged accounts that in-house staff had deprioritized or abandoned.
Related: Accounts Receivable Medical Billing: How to Reduce Days in AR
What the Practice’s Day-to-Day Looks Like After Outsourcing
The most common question practices ask before outsourcing claims processing is: what will my day look like after this? The answer is: considerably less billing administration, more focused on the clinical and registration inputs that feed the billing function, and replaced daily billing management with monthly reporting review.
On a daily basis, the practice’s billing-related activity is documentation completion on schedule, front-desk insurance data capture, and responding to any documentation queries that arrive from the coding team. None of these are new activities. They are existing activities that need to be done more consistently because the outsourced partner depends on them and has defined performance expectations that make inconsistency visible.
On a weekly basis, there may be denial-related requests for clinical documentation or physician involvement in peer-to-peer reviews. These are not frequent — a well-run outsourced engagement resolves the majority of denials without practice-side involvement — but they require prompt response when they occur. A denial appeal that requires a physician’s clinical context and doesn’t receive it within the payer’s appeal window is a lost appeal regardless of whose fault the delay is.
On a monthly basis, the practice receives the performance report from the partner. This report is the primary management tool for the outsourced engagement. It shows whether the partner is performing at the contracted standard, where performance gaps exist and what the partner is doing to address them, and what practice-side factors — documentation quality, registration accuracy, credentialing gaps — are affecting billing performance that the partner cannot control. Reviewing this report carefully and following up on practice-side items is the practice’s core management responsibility in an outsourced billing engagement.
How the Transition Actually Works
The transition to outsourced claims processing has three phases that determine how well the new arrangement performs from day one.
Phase 1: Integration and Configuration (Weeks 1 to 3)
The technical integration between the practice’s EHR or practice management system and the partner’s platform is configured, tested, and validated. Payer portal access is established for the partner. Documentation transmission protocols are defined and tested with sample encounters. The partner’s scrubber is configured with the practice’s payer-specific edit rules. ERA auto-posting rules are set up for each payer in the mix. This phase requires active IT coordination between the practice and the partner and should be led by a dedicated implementation contact from the partner’s team.
Phase 2: Parallel Running and Handoff (Weeks 3 to 6)
For practices with an existing in-house billing operation, a parallel running period where both the in-house team and the partner are processing claims simultaneously allows the partner to learn the practice’s payer patterns and catch any configuration issues before the in-house team fully disengages. The transition of pending AR — accounts that were in the in-house team’s queue at the time of transition — requires a defined handoff process so that accounts already in the AR management workflow are picked up by the partner’s team without falling through the gap.
Phase 3: Go-Live and Performance Stabilization (Weeks 6 to 12)
After full go-live, the first 90 days are the period where the partnership’s performance establishes its baseline. The partner is learning the nuances of the practice’s payer mix, documentation patterns, and specialty-specific billing rules. Clean claim rates typically improve from the practice’s prior baseline within 60 to 90 days as the partner’s scrubber configuration stabilizes and coding patterns are refined. AR days begin declining as the partner’s systematic follow-up replaces the ad hoc in-house approach.
Related: What Is Claim Submission in Medical Billing | What Is RCM in Medical Billing
How Qualigenix Manages Outsourced Claims Processing
At Qualigenix, outsourced claims processing is a comprehensive revenue cycle function that covers every stage described in this blog. Our eligibility verification runs automatically from the appointment schedule. Our coding team returns coded encounters within 24 to 48 hours. Our payment posting standard is 48 hours from ERA receipt with 85% or higher auto-posting rates. Our denial management team categorizes, routes, and resolves denials within 72 hours of receipt. Our AR team runs weekly aging reviews with escalation at the 60-day threshold.
We also manage the credentialing and payer enrollment function that makes every claim valid from submission. When a new provider joins a practice we manage, their enrollment status at every payer is tracked, and claim submissions under their NPI are held until enrollment is confirmed. We don’t submit claims under unenrolled providers and generate a denial that requires the practice to sort out after the fact.
Our monthly reporting package delivers every metric the practice needs to verify our performance: clean claim rate, days in AR, denial rate by reason code and payer, net collection rate, charge lag, posting lag, and AR aging distribution. The report is delivered within five business days of month end. We review it with the practice’s billing liaison on a scheduled monthly call and identify any practice-side actions required.
Our onboarding standard is 6 days for practices with standard EHR integrations and accessible payer mixes. Our performance results: 99% claim accuracy rate, 95% first-pass acceptance rate, 36-day average collection cycle, 30% reduction in AR days. These are the outcomes that define what outsourced claims processing is supposed to produce.
Outsource Claims Processing Transition Checklist
- EHR or PM system integration method confirmed — API, HL7, or file transfer
- Documentation transmission schedule defined — same-day or next-day from encounter
- Front-desk registration workflow reviewed — insurance data capture standard confirmed
- Physician documentation completion expectations communicated — same-day or next-day standard
- Documentation query process explained to all physicians — response window standard set
- Payer portal access transferred to partner before go-live
- ERA auto-posting rules configured and tested before first live claims
- Pending AR handoff process defined — in-progress accounts transferred to partner queue
- Write-off approval threshold defined in service agreement
- Monthly reporting package format and delivery date confirmed
- Billing liaison role assigned within practice for partner interface
- HIPAA BAA signed before any documentation is transmitted
- Performance benchmarks written into service agreement: clean claim rate, days in AR, denial rate
Frequently Asked Questions: Outsource Claims Processing
What changes when a practice outsources claims processing?
The billing administration workflow shifts entirely to the partner: eligibility verification, coding, claim construction and submission, payment posting, denial management, secondary billing, and AR follow-up all become the partner’s operational responsibility. The practice retains clinical documentation, front-desk registration data capture, coding query responses, and write-off decisions. The practice’s daily billing management workload is replaced by monthly performance report review and maintenance of the documentation and registration inputs the partner depends on.
What does the practice still own after outsourcing claims processing?
The practice retains responsibility for clinical documentation quality, accurate insurance data capture at registration, timely responses to documentation queries, write-off decisions above the agreed threshold, and provider credentialing currency. None of these are new responsibilities. They are existing practice functions whose quality becomes more consequential when an outsourced partner depends on them to process claims correctly. The most impactful preparation for outsourcing is improving documentation completion speed and registration accuracy before the transition, not after.
How does denial management change when claims processing is outsourced?
Denial management becomes the partner’s systematic operational function rather than an ad hoc billing staff activity. The partner categorizes each denial by root cause, routes it to the appropriate resolution pathway, and resolves it within a defined window — with clinical input from the practice only when the denial requires physician documentation or a peer-to-peer review. The practice sees denial performance through monthly reporting rather than working individual denials. Trend reporting from the partner surfaces systemic denial patterns that require upstream process changes on the practice side.
How does the front desk workflow change when claims processing is outsourced?
The front desk no longer manages eligibility verification as a manual task. the partner handles this automatically from the appointment schedule. What doesn’t change is the front desk’s responsibility for capturing accurate insurance data at each visit. The partner’s automated eligibility checks query payers with the data on file. If that data is wrong, the check returns incorrect results. Confirming the insurance card at every visit and updating the system when plans change is the front-end practice action that makes every downstream billing function — in-house or outsourced — more accurate.
How long does transitioning to outsourced claims processing take?
A well-organized transition takes 30 to 60 days for practices with standard payer mixes and accessible EHR integrations. Qualigenix onboards new clients in as few as 6 days for practices with straightforward integration requirements. The transition includes integration setup, payer portal access configuration, workflow training for practice staff, and the initial period where the partner learns the practice’s payer patterns. The parallel running period where both in-house and the partner process claims simultaneously — allows validation before full handoff without creating a claims submission gap.
What reporting should the practice receive from an outsourced claims partner?
Monthly reporting should cover clean claim rate, days in AR by payer and aging bucket, denial rate by reason code and payer, net collection rate, charge lag, payment posting turnaround, and AR follow-up activity on accounts approaching 90 days. This reporting is the primary management tool for the outsourced engagement. Reviewing it monthly with the partner’s account manager and following up on any practice-side items identified is the core management responsibility the practice retains. Partners who provide only aggregate collections data without this performance detail are not giving the practice the visibility to verify that the engagement is delivering its contracted value.
Related Resources from Qualigenix
We Take the Billing. You Keep the Practice.
Qualigenix manages the full claims processing lifecycle for practices across 38+ specialties — eligibility through AR follow-up, with credentialing built in. You provide documentation and registration data. We handle everything from coded encounter to collected payment.
Our team delivers 99% claim accuracy, a 95% first-pass acceptance rate, an average 36-day collection cycle, and a 30% reduction in AR days. We onboard in as few as 6 days.
Precision. Progress. Qualigenix.
What’s Next

Underpayments vs. Denials: Which One Is Draining Your Practice More?
Denials get attention because they stop cash flow outright. Underpayments don’t stop anything, they just quietly shrink it....
Your AR Days Are Too High. Here’s What That Actually Means for Revenue
AR days over 50 usually means claims are aging into buckets that are hard to collect, not that payers...
From 6-Day Onboarding to First Clean Claim: How Qualigenix Transitions Practices
Most billing transitions take 30 to 90 days and stall revenue in the gap. Qualigenix compresses that timeline to...