What Is Charge Entry in Medical Billing and How It Works
The Qualigenix Editorial Team consists of certified billing and coding experts with over 40 years of experience across 38+ medical specialties. Our content is rigorously researched against CMS, AMA, and payer-specific guidelines to ensure total compliance and accuracy. We apply the same elite standards to our resources as we do our client work, consistently delivering high claim accuracy and significant reductions in AR days.
Charge entry is the step in the revenue cycle that converts a clinical encounter into a billable record. It is not the same as coding, not the same as claim submission, and not a function that can be deferred without consequences. Every day a charge sits unprocessed after a service is delivered is a day the collection clock isn’t running. Every field entered incorrectly in the charge entry step travels onto the claim and into the payer’s adjudication system as an error that produces either a rejection or a denial. Every service delivered but not entered is revenue that doesn’t exist in the billing system and will never be collected unless a charge reconciliation process catches it. Charge entry accuracy and timeliness are the inputs that determine billing outcomes. No downstream billing process produces accurate, timely payments from inaccurate, delayed charge entry.
When a practice’s days-in-AR metric is above benchmark, the billing team’s first instinct is often to look at denial management, payment posting, or AR follow-up. These are reasonable places to investigate. But many of the most persistent days-in-AR problems trace back further to charge entry, where the clock on the collection cycle starts. A claim that was entered three days after the encounter is already three days older than it needed to be at submission. A charge entered with the wrong place-of-service code submits with an error. A charge never entered at all never generates a claim.
Charge entry is one of those revenue cycle functions whose quality is most visible when it fails and least visible when it works. When charge entry is accurate and timely, claims submit clean, payment arrives on schedule, and the billing operation appears to be running well. When charge entry is delayed or error-prone, the consequences appear in the billing queue days later as rejections and denials by which time the charge entry step that caused them is often already forgotten.
Understanding what charge entry is, what it covers, and how its performance affects every downstream billing outcome is foundational knowledge for any practice that wants to understand where its revenue cycle performance is actually coming from.
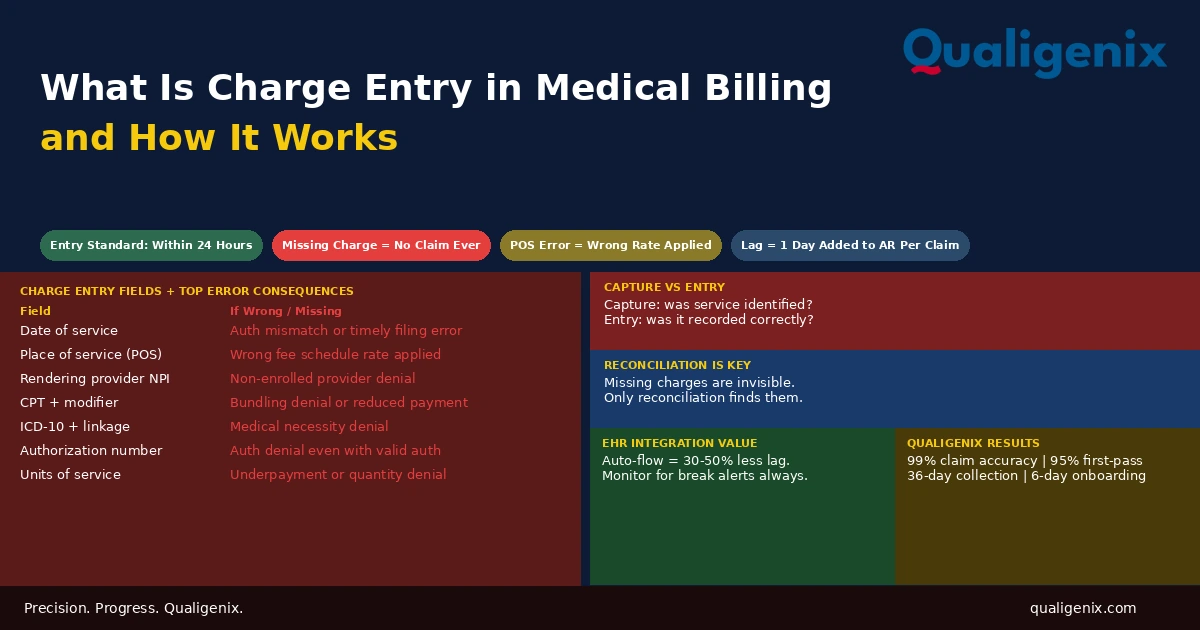
Charge entry in medical billing is the process of recording the services delivered during a clinical encounter date of service, place of service, rendering provider NPI, CPT codes, ICD-10 diagnosis codes, modifiers, units, billed charge, and authorization number into the billing system to create the billable record from which an insurance claim is built. The industry standard is within 24 hours of the encounter. Charge lag beyond this standard contributes directly to elevated days in AR, timely filing exposure, and memory-based coding risk when documentation isn’t reviewed promptly.
Charge Entry in Medical Billing: Key Standards and Benchmarks
| Metric | Standard / Benchmark | Context |
|---|---|---|
| Charge entry turnaround standard | Within 24 hours of encounter | Industry best practice |
| Charge entry warning level | Beyond 48 hours average | Meaningful charge lag begins here |
| Timely filing risk level | Beyond 72 hours | Exposure for 90-day filing payers at volume |
| Charge entry error rate target | Under 2% of entered charges | Revenue cycle quality benchmark |
| Most common charge entry error | Wrong place-of-service code | Billing error analysis |
| Missing charge revenue impact | Up to 5% of potential revenue | Practices without charge reconciliation |
| EHR-integrated vs manual entry lag reduction | 30% to 50% faster | EHR integration benchmarks |
| Charge lag impact on days in AR | 1 day lag = 1 additional day per claim in AR | Direct arithmetic relationship |
| Qualigenix claim accuracy rate | 99% | Qualigenix performance data |
| Qualigenix first-pass acceptance rate | 95% | Qualigenix performance data |
| Qualigenix average collection cycle | 36 days | Qualigenix performance data |
| Qualigenix client onboarding time | 6 days | Qualigenix operations data |
Where Charge Entry Fits in the Revenue Cycle
The revenue cycle is a sequence of steps that converts delivered care into collected revenue. Each step depends on the one before it. Charge entry sits at the juncture between the clinical workflow and the billing workflow the handoff point where information generated during patient care becomes information the billing system can act on.
Before charge entry: the patient registers, insurance is verified, the physician delivers care, documentation is completed, and a coder assigns CPT and ICD-10 codes to the encounter. All of this feeds into charge entry as inputs.
After charge entry: the billing system builds a claim from the entered charge record, scrubs it for errors, submits it to the payer, tracks adjudication, posts the payment or denial, and manages follow-up through collection. All of this depends on charge entry as the foundation.
Charge entry is the last point in the revenue cycle where an error can be caught before it becomes a claim error. A wrong place-of-service code identified during charge review costs nothing to fix. The same error identified after claim submission as a payer rejection costs the time to correct and resubmit plus the days of delay added to the collection cycle. A missing charge identified during charge reconciliation before billing costs a few minutes to add. The same missing charge identified never costs the full allowed amount permanently. The economics strongly favor accuracy at charge entry over correction downstream.
What Charge Entry Captures: Every Required Field
Charge entry is not just entering a CPT code and a diagnosis code. A complete, accurate charge entry record contains a specific set of fields, each of which is required for the claim to be built correctly. An error or omission in any field travels directly onto the claim and produces a predictable billing consequence.
Date of Service
The date of service is the date the clinical encounter occurred. It is the starting point for timely filing calculations — the filing window opens on the date of service. It is also the reference date for authorization validity checks, global period calculations, and same-day service rules. An incorrect date of service on a charge produces a claim with the wrong date, which can cause the authorization to appear invalid (if the authorized date doesn’t match the billed date), the timely filing calculation to be inaccurate, or the same-day bundling rules to apply when they shouldn’t.
Place of Service Code
The place of service code is a two-digit code identifying where the service was delivered. It determines the fee schedule rate applied to the claim. POS 11 (office) triggers the non-facility rate. POS 21 (inpatient hospital) and POS 22 (outpatient hospital) trigger the lower facility rate. POS 23 (emergency department), POS 24 (ambulatory surgery center), and others each have specific rate and billing rule implications.
Wrong place-of-service code is the most common charge entry error in practices where providers work in multiple settings. A hospitalist who sees patients in the hospital and occasionally in the clinic, or a surgeon who has both office visits and inpatient rounding, must have the correct POS code applied to each encounter based on where it actually occurred. POS 11 on a hospital encounter is an overpayment at the non-facility rate. POS 21 on an office encounter is an underpayment at the facility rate. Both are charge entry errors with revenue consequences in opposite directions.
Rendering Provider NPI
The rendering provider NPI identifies which physician performed the service. In group practices where multiple providers see patients, charge entry must accurately attribute each charge to the correct rendering provider. The rendering provider must be enrolled with the patient’s payer — a charge entered under a provider whose enrollment is pending or lapsed generates an automatic denial regardless of how accurately everything else was entered. In practices with residents or fellows under supervision, the attending’s NPI may be required rather than the trainee’s, depending on the payer’s supervision billing rules.
CPT Codes and Modifiers
The CPT code entered at charge entry is the procedure code that the payer will reimburse based on its fee schedule. The modifier entered alongside it provides context about how the service was performed. Both must be accurate and complete. A CPT code entered without a required modifier produces a bundling denial or a reduced payment. A modifier entered incorrectly misrepresents the clinical circumstances of the service. In high-volume practices where charge entry is performed quickly, modifier errors are among the most common quality gaps — the code is entered correctly but the modifier step is skipped or applied from a default that doesn’t match the actual service circumstances.
ICD-10 Diagnosis Codes and Linkage
The ICD-10 codes entered at charge entry identify the patient’s diagnoses and establish medical necessity for the CPT codes billed. Each CPT code must be linked to a diagnosis code that supports its clinical necessity. Incorrect diagnosis codes, unspecified codes where specific ones are available, or diagnosis-to-procedure linkage that doesn’t match the clinical relationship between the condition and the service all produce medical necessity denials or ICD-10 specificity failures. Related: What Is Healthcare Coding and How It Works
Units of Service
Units represent the quantity associated with the CPT code. For standard single-service CPT codes, the unit is 1. For time-based add-on codes — such as prolonged services, critical care beyond the initial time increment, or psychotherapy add-ons — units represent the number of qualifying time periods. For drug administration HCPCS codes, units represent the quantity of drug administered in the billing unit defined for that J-code. Entering the wrong units produces either an underpayment (too few units) or a denial for excessive quantity (too many units).
Billed Charge
The billed charge is the practice’s standard fee for the service. It should be set from a fee schedule that reflects market rates — typically two to three times Medicare fee schedule rates — that allows for payer contractual adjustments while leaving room above the contracted rate. The billed charge is not what the practice expects to collect; it is the gross amount from which contractual adjustments are calculated. A billed charge lower than the payer’s allowed amount results in the practice collecting less than the allowed amount, since payers pay the lesser of the billed charge or the allowed amount.
Authorization Number
When a service required prior authorization, the authorization number must be included in the charge entry record and transmitted on the claim. A claim submitted without the authorization number for a service that required it denies for missing authorization regardless of whether the authorization was legitimately obtained. The charge entry step is where the authorization number is attached to the claim record — if it isn’t entered here, it won’t be on the claim. Related: What Is Health Insurance Pre-Authorization
Charge Capture vs Charge Entry: Two Different Problems
Charge capture and charge entry are related but distinct functions, and failures at each produce different types of revenue loss.
Charge capture is the process of identifying all services delivered during an encounter and ensuring they are recorded for billing. It answers the question: what was done? Charge capture happens at the clinical level. The physician closes the encounter in the EHR, completes a charge sheet or superbill, or dictates charges as part of the documentation process. A charge capture failure means a service was delivered but never recorded for billing. The charge entry step never receives it because the capture step missed it.
Charge entry is the process of recording captured charges into the billing system. It answers the question: is what was captured now in the billing system accurately and completely? A charge entry failure means a captured charge was entered incorrectly, incompletely, or not at all. The charge capture step identified the service correctly; the charge entry step recorded it wrong.
Both types of failures produce missing or incorrect revenue. Charge capture failures is services delivered but never captured and are the harder failure to detect because there is no record of the uncaptured service in the billing system to alert anyone that something is missing. Charge reconciliation is the process that catches capture failures by comparing what the billing system contains against an independent record of services delivered, such as the appointment schedule or the EHR encounter list.
Warning: Charge capture failures are invisible to the billing team because there is nothing in the billing queue to work. A service that wasn’t captured doesn’t appear as a missing claim, a pending charge, or a denial. It simply doesn’t exist in the system. The only way to identify charge capture failures is a reconciliation process that compares services rendered against charges entered. Practices without a formal charge reconciliation process have no way of knowing how much revenue is lost to uncaptured services research suggests this can represent up to 5% of potential revenue in practices with manual capture processes and no reconciliation workflow.
Charge Lag: How Delayed Entry Compounds Into AR Problems
Charge lag is the elapsed time between when a service is delivered and when the charge for that service enters the billing system. The arithmetic relationship between charge lag and days in AR is direct: every day of charge lag adds one day to the time between service delivery and claim submission, which adds one day to the time between service delivery and payment receipt.
At individual encounter level, a three-day charge lag is modest. At practice level with 2,000 claims per month, a consistent three-day charge lag means every claim in the billing pipeline is three days older than it needs to be at submission. If the average allowed amount per claim is $150, the practice is carrying $300,000 in claims that are three days further from payment than optimal. The cash flow difference compounds across every month the lag persists.
Charge lag also creates timely filing exposure. Medicare’s 12-month window is long enough that normal charge lag doesn’t create timely filing risk. Commercial payers with 90-day filing windows present a real risk when charge lag is combined with any additional processing delays. A charge entered seven days after service at a payer with a 90-day window has 83 days of effective filing time remaining, less than the nominal window and less than a practice might assume when planning its billing workflow. If that charge then sits in a coding queue for five more days before the claim submits, the effective window is 78 days.
Beyond the filing window concern, charge lag introduces memory-based coding risk. When a physician completes a note and the coder reviews it the same day, the documentation review is immediate and fresh. When the same note is reviewed five days later because the charge was delayed, the coder may not have access to the physician to resolve documentation questions quickly, the physician’s memory of the specific encounter may be less reliable for addendum purposes, and the clinical context that would have prompted a query is less accessible. Charge lag makes documentation review less effective for the same reason that any review delayed from its source event produces less reliable results.
The Superbill: What It Is and When It’s Still Used
The superbill is a charge capture form originally paper, now often electronic that lists the CPT and ICD-10 codes most commonly used by a specific practice, allowing clinical staff to check off or select the services delivered during an encounter. The checked superbill becomes the input document for charge entry: the billing staff enters the checked items into the billing system.
In practices with fully integrated EHR and practice management systems, the superbill function has largely been replaced by encounter close workflows within the EHR, the physician selects diagnoses and procedures within the clinical documentation interface, and those selections flow directly to the billing system without a separate manual entry step. This integration eliminates the transcription errors that occur when a charge entry staff member reads a paper superbill and enters the data manually, and it reduces charge lag by removing the manual handoff step.
In practices that still use paper superbills or non-integrated EHR and billing systems, manual charge entry from the superbill or documentation remains the standard. Manual entry is slower, more error-prone, and more dependent on the accuracy and legibility of the source document than EHR-integrated entry. The common errors in manual entry are CPT code transcription (entering a code that looks similar to the correct one but describes a different service), ICD-10 code errors (entering an outdated code or a non-specific code from the superbill when the documentation would support a more specific one), and missing fields that aren’t on the superbill template.
EHR Integration and Its Impact on Charge Entry Quality
The quality and depth of the integration between the practice’s EHR and billing system is one of the strongest determinants of charge entry accuracy and timeliness. A well-configured, reliable integration between the two systems eliminates the manual data transfer step that produces most charge entry errors and most of the charge lag in practices that still manage this handoff manually.
When an EHR-billing integration works correctly, the physician closes an encounter in the EHR with diagnoses and procedures selected, and that encounter data flows to the billing system automatically, typically within minutes. The charge entry staff reviews the auto-populated charge record for completeness and accuracy rather than building it from scratch, catching exceptions rather than entering every field. This reduces both the time required for charge entry and the error rate by shifting the staff’s role from data entry to quality control.
When the integration doesn’t work, when it breaks during an EHR or billing system update, when the field mapping between the two systems is incomplete, or when encounter data transfers with errors in specific field types. The impact on charge entry quality is immediate and often not noticed until denial patterns appear in the billing queue. An integration that is intermittently unreliable creates the worst charge entry quality profile: sometimes accurate and immediate, sometimes incomplete or delayed, with no reliable indicator of which encounters flowed correctly and which didn’t without a charge reconciliation process that checks every encounter.
Related: Medical Billing Software: What to Look For
Common Charge Entry Errors and Their Billing Consequences
Each charge entry error type produces a specific and predictable billing consequence. Understanding the mapping allows billing teams to trace denial patterns back to their charge entry origin.
| Charge Entry Error | Billing Consequence | Resolution |
|---|---|---|
| Wrong place-of-service code | Incorrect fee schedule rate applied or reimbursement error | Corrected claim with correct POS code |
| Missing modifier 25 | E/M bundled into procedure — E/M denied | Add modifier and resubmit |
| Wrong units for time-based code | Underpayment or excessive units denial | Corrected claim with accurate units |
| Missing authorization number | Authorization denial even with valid auth | Add auth number and resubmit |
| Wrong date of service | Auth date mismatch or timely filing error | Corrected claim with correct DOS |
| Wrong rendering provider NPI | Provider not recognized denial | Corrected claim with correct NPI |
| ICD-10 not linked to CPT | Medical necessity denial | Correct linkage and resubmit |
| Duplicate charge entry | Duplicate claim denial on second submission | Void duplicate charge before submission |
| Missing charge (not entered) | No claim generated — revenue lost unless caught by reconciliation | Enter missed charge if within filing window |
| Billed charge below allowed amount | Practice collects less than allowed — permanent unless billed charge corrected | Update fee schedule and correct future charges |
Charge Reconciliation: Catching What Charge Entry Misses
Charge reconciliation is the process of verifying that every service delivered during a period has a corresponding charge in the billing system. It is the quality control step that catches both charge capture failures (services never recorded for billing) and charge entry gaps (charges captured but not entered into the system).
A basic charge reconciliation process compares two lists: the encounters scheduled and completed in the appointment system or EHR, and the charges entered in the billing system for the same period. Any encounter with a completed visit that has no corresponding charge is flagged for investigation. The investigation determines whether the encounter generated a charge that wasn’t entered (an entry failure) or whether the encounter was a no-show or cancellation that legitimately has no charge.
For practices with high procedure volumes surgical practices, infusion practices, diagnostic practices. Charge reconciliation is particularly important because procedures generate higher-value charges than E/M visits. A missing surgical charge or a missed infusion administration code represents a significantly larger revenue loss per incident than a missing office visit charge. Reconciliation frequency should match the value density of the practice’s encounter mix: daily reconciliation for procedure-heavy practices, at minimum weekly for lower-volume practices.
Charge Entry in Different Practice Settings
Charge entry requirements and common error patterns differ by practice setting and specialty. Understanding the specific charge entry challenges of each setting helps billing teams target their quality control where it matters most.
Office-Based Practices
Office-based practices primarily enter E/M codes with associated diagnosis codes. The most common charge entry issues are place-of-service code errors when physicians also see patients in hospital settings, missing modifier 25 when procedures and E/M visits occur on the same day, and charge lag from physicians who complete notes in batches rather than same-day. Related: Outpatient Coding Accuracy at Scale
Surgical Practices
Surgical practices have complex charge entry requirements: the surgical procedure code, anesthesia notification, assistant surgeon codes when applicable, and separate charges for supplies that are billed outside the procedure’s global package. The most common charge entry issues are global period violations (charges entered for services included in the surgical global fee), wrong surgical CPT code (a code that describes a similar but different procedure), and missing assistant surgeon modifier when the assistant is separately billable. Related: Charge Capture for High-Volume Specialties
Hospital-Based Practices
Hospital-based practices — hospitalists, intensivists, emergency physicians deal with the specific charge entry complexity of the inpatient code set: initial hospital care, subsequent care, and discharge codes that each require different documentation and have different entry rules. The most common error is entering the same subsequent care code for every daily visit regardless of clinical complexity, resulting in systematic under coding that is visible only through a code distribution audit. Related: Inpatient Coding for Physicians: What Changes
Infusion and Specialty Drug Practices
Practices that administer infusions and specialty drugs face the most complex charge entry requirements in outpatient settings. Drug administration requires both the infusion administration CPT code and the drug J-code entered with accurate units. The units for most J-codes represent specific quantities per billing unit — a drug dosed at 100mg with a J-code unit of 10mg requires 10 units on the charge entry. Entering 1 unit instead of 10 results in the practice billing for one-tenth of the drug cost. Entering 100 units produces an excessive quantity denial. The correct units calculation requires knowing the specific J-code’s billing unit, the dose administered, and the arithmetic conversion — a charge entry step that is more technically demanding than standard CPT-based charge entry.
How Qualigenix Manages Charge Entry
At Qualigenix, charge entry is a same-day-standard function integrated with coding and billing into a unified revenue cycle workflow. We enter charges within 24 hours of receiving complete clinical documentation for every encounter, with a charge reconciliation process that compares entered charges against the schedule or encounter list daily to catch any missed entries before they age past the timely filing window.
Our charge entry team applies place-of-service codes from the documented service location rather than from a system default. We maintain a modifier review step that checks every charge for modifier 25 on same-day E/M and procedure combinations, modifier completeness for surgical charges, and unit accuracy for time-based and drug administration codes. Authorization numbers are linked to charges at entry from our authorization tracking system rather than relying on manual entry at submission.
Our charge entry quality is monitored through weekly charge lag reports that track average time from documentation receipt to charge entry, and monthly error rate reports that identify any charge entry error patterns by field type and by practice. When a charge entry error pattern appears, we trace it to the source typically a system configuration issue, a training gap, or a documentation workflow problem and implement the fix before the pattern compounds into a denial category.
Related: What Is RCM in Medical Billing | What Is Claim Submission in Medical Billing | What Is Aging Accounts Receivable
Charge Entry Accuracy Checklist
- Charge entry standard of 24 hours from documentation receipt enforced
- Average charge lag calculated weekly — above 48 hours triggers root cause review
- Place-of-service code verified from documented service location — not from system default
- Rendering provider NPI confirmed as enrolled with patient’s payer before entry
- Modifier 25 applied for same-day E/M and procedure combinations
- Units verified for time-based codes and drug administration J-codes
- ICD-10 diagnosis codes linked to each CPT code they support
- Authorization number included for all services requiring prior authorization
- Billed charge verified against current fee schedule — not below allowed amount
- Duplicate charge check before submission — same date, same patient, same code
- Daily charge reconciliation comparing entered charges to completed encounters
- EHR-billing integration reliability monitored — break alerts configured and tracked
Frequently Asked Questions: Charge Entry in Medical Billing
What is charge entry in medical billing?
Charge entry is the step that records services delivered during a clinical encounter into the billing system — date of service, place of service, CPT codes, ICD-10 codes, modifiers, units, billed charge, and authorization number — creating the billable record from which a claim is built. It sits between clinical documentation and claim submission and is the last point where an error can be caught before it becomes a claim error. Accuracy at this step determines whether the claim will be paid correctly. Timeliness determines when the collection clock starts on the encounter.
What is charge lag and why does it matter?
Charge lag is the elapsed time between when a service is delivered and when its charge is entered into the billing system. The standard is within 24 hours. Beyond 48 hours is meaningful lag that directly increases days in AR by the same number of days the charge was delayed. At high volume, consistent charge lag of two to three days per encounter compounds into a systemic days-in-AR gap that appears as a billing performance problem but traces back to the charge entry step. Charge lag also creates timely filing exposure and introduces memory-based coding risk when documentation isn’t reviewed promptly after the encounter.
What is the difference between charge capture and charge entry?
Charge capture identifies what services were delivered — it happens at the clinical level when the physician closes an encounter and selects services. Charge entry records those captured services into the billing system — it happens at the billing level. A charge capture failure means a service was never identified for billing. A charge entry failure means a captured service was entered incorrectly or not at all. Both produce missing revenue, but capture failures are harder to detect because there’s no record in the billing system to flag them — only a charge reconciliation process that compares services rendered against charges entered can surface them.
What are the most common charge entry errors?
The most common charge entry errors are wrong place-of-service code, missing modifier 25 on same-day E/M and procedure combinations, incorrect units for time-based or drug administration codes, and missing authorization numbers on claims requiring prior auth. Each produces a specific and predictable billing consequence — incorrect reimbursement rate, E/M bundling denial, underpayment or quantity denial, and authorization denial respectively. All are caught by a charge review step or claim scrubber before submission when those quality controls are correctly configured and current.
What is a superbill in charge entry?
A superbill is a structured charge capture form — paper or electronic — listing the CPT and ICD-10 codes most commonly used by the practice, allowing clinical staff to check off services delivered during an encounter. In practices with integrated EHR-billing systems, the superbill function has largely been replaced by encounter close workflows that flow charge data directly to the billing system. When superbills are still used, the charge entry step involves manually entering the checked codes into the billing system — a process more prone to transcription errors and charge lag than automated EHR integration.
How does charge entry affect days in AR?
Charge entry lag directly adds to days in AR because the collection clock doesn’t start until the charge is entered and the claim is submitted. Every day of charge lag is one additional day between service delivery and payment receipt — an arithmetic relationship that compounds across every claim in the pipeline. When days in AR is above benchmark and the denial rate is at or below benchmark, charge lag is a primary suspect. The billing team may be working efficiently on what’s in the queue, but the queue is consistently older than it should be because charges are entering it late.
Related Resources from Qualigenix
- What Is RCM in Medical Billing
- What Is Claim Submission in Medical Billing
- What Is Aging Accounts Receivable
- Charge Capture for High-Volume Specialties
- What Is Healthcare Coding and How It Works
Accurate Charge Entry In. Clean Claims Out. On Time.
Qualigenix manages charge entry as part of the integrated revenue cycle for practices across 38+ specialties — same-day standards, daily reconciliation, place-of-service verification, modifier checks, and authorization linkage — so every service delivered becomes a correctly built claim submitted without delay.
Our team delivers 99% claim accuracy, a 95% first-pass acceptance rate, an average 36-day collection cycle, and a 30% reduction in AR days. We onboard in as few as 6 days.
Precision. Progress. Qualigenix.
What’s Next

Denial Management in 2026: The Top 10 Codes and the Appeal Playbook for Each
Denials cluster around a small set of codes, and each one has a different correct response. Some need a...
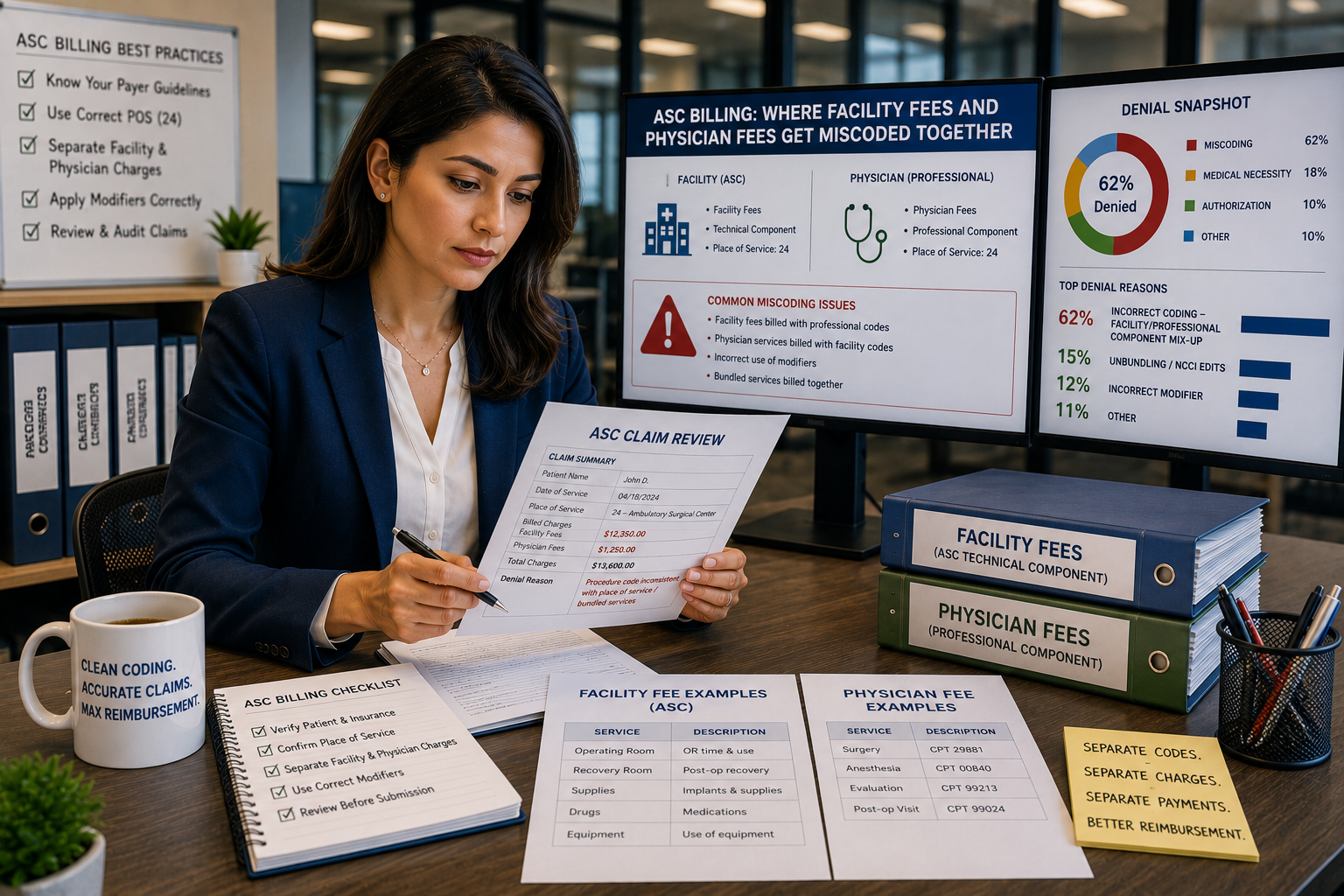
ASC Billing: Where Facility Fees and Physician Fees Get Miscoded Together
ASC facility and physician claims both go out on a CMS-1500 form with the same CPT code and place...
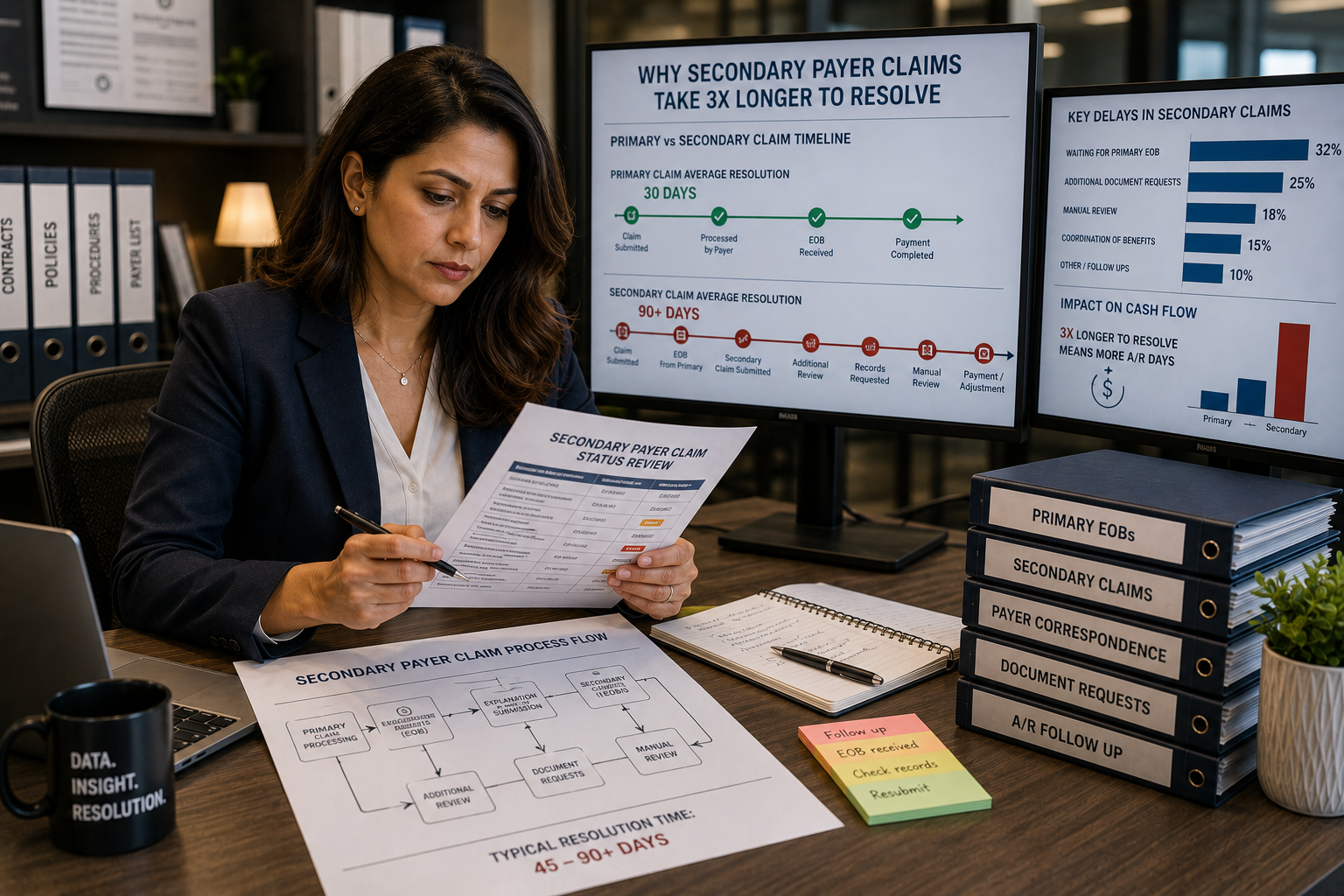
Coordination of benefits errors: why secondary payer claims take 3x longer to resolve
Secondary payer claims stall because coordination of benefits errors, wrong payer order, outdated COB records, and missing primary...