What Is Health Insurance Pre-Authorization and How It Works
The Qualigenix Editorial Team consists of certified billing and coding experts with over 40 years of experience across 38+ medical specialties. Our content is rigorously researched against CMS, AMA, and payer-specific guidelines to ensure total compliance and accuracy. We apply the same elite standards to our resources as we do our client work, consistently delivering high claim accuracy and significant reductions in AR days.
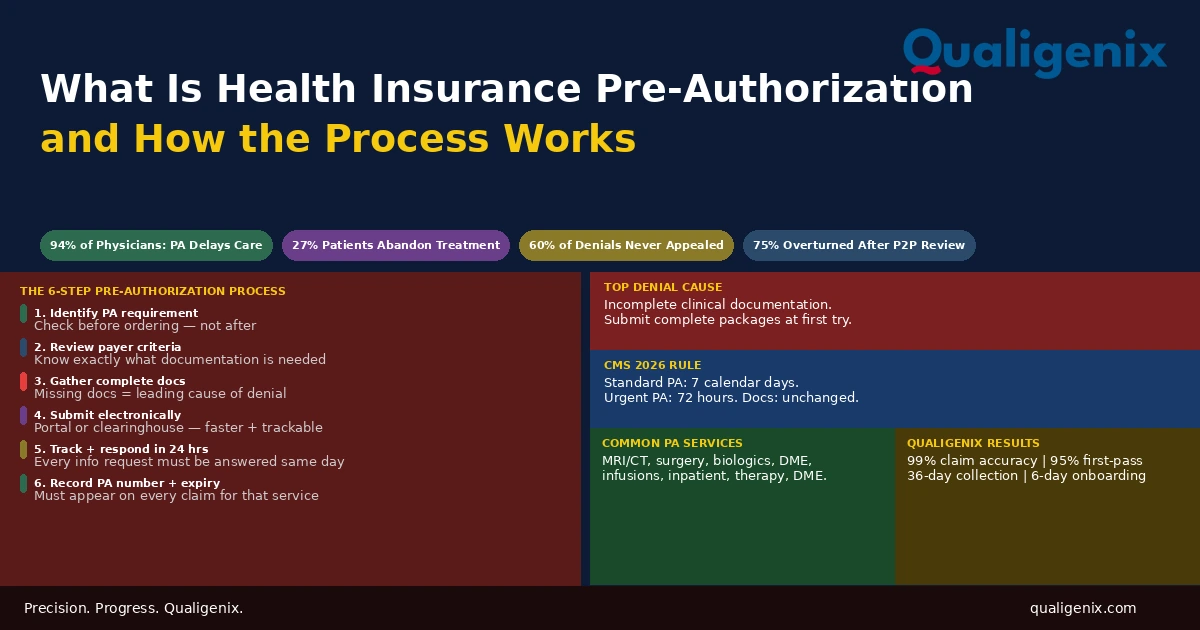
Health insurance pre-authorization is the approval step that sits between a physician’s clinical decision and a patient’s access to a covered service. When it’s required and obtained before the service is delivered, the insurer pays. When it’s required and not obtained, the insurer doesn’t, and the financial consequence falls on either the patient or the practice. The process has grown more complex as payers have expanded the list of services requiring PA, increased clinical criteria requirements, and maintained systems that require active management to navigate. Understanding how pre-authorization works from identification through approval, denial, and appeal. It is now a core competency for every practice that wants to get paid for the care it delivers.
A physician decides a patient needs an MRI. The clinical rationale is clear. The order is written. The scheduling team contacts the imaging center. And then the pause: does this require prior authorization? If yes, which payer, which plan, which clinical criteria apply? Is the patient in a plan that processes PA through a separate radiology benefits manager? Has anything in the patient’s coverage changed since their last visit?
This is the pre-authorization reality for most practices today. According to AMA surveys, physicians and their staff spend an average of 13 or more hours per week managing prior authorization requests across all service types. Ninety-four percent of physicians report that PA causes delays in patient care. Twenty-seven percent of patients abandon recommended treatment entirely when PA creates extended access barriers. And approximately 60% of denied PA requests are never appealed, meaning practices absorb the cost of uncompensated services that payers would often have paid if the denial had been challenged.
This blog explains what health insurance pre-authorization is, which services require it, how the approval process works from start to finish, what happens when authorization is skipped or denied, and what the 2026 regulatory changes mean for how practices manage it.
Health insurance pre-authorization is the process by which a provider obtains insurer approval before delivering a specific service, procedure, or medication. The insurer reviews clinical documentation to confirm the service meets their medical necessity criteria and coverage policies. Without an approved pre-authorization for services that require one, the insurer will not cover the cost. The process requires identifying the PA requirement before the service, gathering complete clinical documentation, submitting the request electronically, tracking it to decision, and recording the authorization number for use on the claim.
Health Insurance Pre-Authorization: Key Numbers
| Metric | Data Point | Source |
|---|---|---|
| Average PA requests per physician per week | 45 across all service types | AMA prior authorization survey 2024 |
| Physicians reporting PA causes care delays | 94% | AMA prior authorization survey 2024 |
| Patients abandoning treatment due to PA delays | Up to 27% | AMA patient impact data |
| CMS 2026 standard PA response time requirement | 7 calendar days | CMS prior authorization final rule |
| CMS 2026 urgent PA response time requirement | 72 hours | CMS prior authorization final rule |
| PA denials overturned after peer-to-peer review | Up to 75% | AMA PA reversal data |
| PA requests requiring additional information | Up to 40% of submitted requests | Payer PA processing data |
| Staff hours per physician per week on PA | 13+ hours for 35% of physicians | AMA prior authorization survey 2024 |
| PA denials never appealed by practices | Approximately 60% | Healthcare billing industry data |
| Leading cause of PA denial | Incomplete clinical documentation | Payer denial analysis |
| Qualigenix first-pass acceptance rate | 95% | Qualigenix performance data |
| Qualigenix claim accuracy rate | 99% | Qualigenix performance data |
| Qualigenix average collection cycle | 36 days | Qualigenix performance data |
| Qualigenix client onboarding time | 6 days | Qualigenix operations data |
What Health Insurance Pre-Authorization Actually Is
Health insurance pre-authorization also called prior authorization, PA, or pre-cert is a utilization management tool payers use to review the clinical appropriateness of a service before they commit to covering it. The payer is not questioning the physician’s clinical judgment outright. They are applying their own coverage criteria to confirm the service falls within what their plan covers, is medically necessary under their definition of that term, and is the appropriate treatment given the patient’s documented clinical situation.
From the payer’s perspective, pre-authorization reduces spending on services that are elective, duplicative, or could be addressed with a less costly alternative. From the practice’s perspective, it is an administrative requirement that must be satisfied before a service is delivered — or before the payer will pay for it. From the patient’s perspective, it is often an invisible process they are unaware of until a denial creates a barrier to care they expected to receive.
Pre-authorization is not a guarantee that the service is the right clinical choice. It is not an endorsement of the physician’s treatment plan. It is an administrative confirmation that the service, as described in the documentation submitted, meets the payer’s criteria for coverage under the patient’s specific plan on the date of the request. Any change between the authorization and the service — a different provider, a different site, a different CPT code — can invalidate the authorization even if the service itself was appropriate.
The list of services requiring pre-authorization has expanded significantly over the past decade. Payers have added imaging, surgical procedures, durable medical equipment, outpatient infusions, behavioral health services, and a growing number of prescription medications to their PA requirements. The expansion reflects payers’ interest in managing utilization and cost. It also means that practices that were managing 10 or 15 PA requests per physician per week a decade ago may now be managing 30 to 50, without proportional increases in administrative staff.
Which Services Commonly Require Pre-Authorization
PA requirements vary by payer, plan type, and patient benefit design. There is no universal list. What requires PA under one commercial plan may not require it under another. A service that Medicare covers without PA may require PA under a Medicare Advantage plan. The safest approach is to verify PA requirements for each specific service under each specific patient’s plan before scheduling or ordering.
That said, predictable patterns exist across most commercial and government plan types.
| Service Category | Common PA Requirement | Key Documentation Typically Needed |
|---|---|---|
| Advanced imaging (MRI, CT, PET) | Most commercial and Medicare Advantage plans | Diagnosis, clinical indication, prior imaging results |
| Elective surgeries and procedures | Most commercial plans for major procedures | Diagnosis, conservative treatment failure, surgical necessity |
| Specialty medications and biologics | Nearly universal across all plan types | Diagnosis, step therapy compliance, disease activity scores |
| Inpatient hospital admissions (non-emergency) | Most commercial plans for planned admissions | Diagnosis, medical necessity, admission criteria met |
| Physical, occupational, speech therapy | Often after defined visit threshold | Functional baseline, treatment plan, progress documentation |
| Durable medical equipment (DME) | Most plans for higher-cost equipment | Diagnosis, functional need, physician order |
| Home health services | Most plans for ongoing home health | Homebound status, plan of care, clinical need |
| Mental health inpatient admissions | Most commercial and Medicaid plans | Clinical assessment, level of care criteria, safety assessment |
| Outpatient infusion therapy | Many commercial and Medicare Advantage plans | Diagnosis, drug PA, site of care appropriateness |
| Genetic testing | Increasingly required across payer types | Clinical indication, family history, specialist involvement |
The Pre-Authorization Process: Step by Step
A pre-authorization request that moves smoothly from submission to approval follows a defined sequence. Failures at any stage extend the timeline, delay patient access to care, and risk an expired window by the time approval arrives. Understanding what each stage requires allows practices to build a PA workflow that consistently clears the process without avoidable delays.
Step 1: Identify the PA Requirement Before the Service Is Scheduled
The most important moment in the PA process is the earliest one: confirming that PA is required before the service is ordered, not after. Practices that check PA requirements at the point of scheduling rather than after the fact avoid the most common and most costly PA failure — delivering a service without authorization because no one checked whether one was needed.
Most payers provide PA requirement checks through their provider portals or through clearinghouse eligibility tools that include benefit detail responses. Real-time benefit check tools integrated with electronic prescribing and scheduling systems can surface PA requirements at the point of ordering. The check must be done for each specific service, specific CPT code, and specific patient’s plan, not from memory of what required PA last month or last year.
Step 2: Review the Payer’s Clinical Criteria
Once a PA requirement is confirmed, the next step is understanding exactly what the payer needs to approve the request. Payers publish clinical coverage criteria for services requiring PA. These criteria specify the diagnosis codes required, any step therapy or prior treatment that must be documented, clinical data or scoring tools required, and the medical necessity standard the request must meet.
Reviewing criteria before gathering documentation prevents submitting incomplete requests. A practice that submits an MRI authorization request with a diagnosis code and a brief note may receive an additional information request from the payer asking for documentation of conservative treatment that was tried first. That follow-up adds days to the timeline. Reviewing the criteria upfront allows all required documentation to be gathered before the first submission.
Step 3: Gather Complete Clinical Documentation
Incomplete clinical documentation is the leading cause of PA delays and denials. Complete documentation for a PA request means every element the payer’s criteria require is present in the submission. Not some of them. All of them.
For a standard imaging PA, this typically includes the patient’s diagnosis with ICD-10 codes, clinical indication in the physician’s language, results of any prior conservative treatment, and relevant prior test results. For a specialty medication PA, it includes all of the above plus step therapy compliance documentation, disease activity scores, relevant lab results, and in many cases a clinical justification letter from the prescribing physician addressing each criterion the payer evaluates.
Warning: The most dangerous approach to PA documentation is submitting what the practice believes should be sufficient and waiting to see what the payer requests. Each round of additional information requests adds days to the authorization timeline. For elective procedures scheduled weeks out, this may be manageable. For services a patient needs promptly, each delay has a clinical cost. Building documentation templates that map directly to each payer’s PA criteria for commonly requested services is the process change that eliminates most additional information requests from the workflow.
Step 4: Submit the PA Request Electronically
Electronic submission through the payer’s portal or a clearinghouse is faster, more trackable, and generates confirmation of receipt. The CMS 2026 prior authorization rule requires Medicare Advantage, Medicaid managed care, and ACA marketplace plans to support electronic PA through FHIR-based APIs. This is pushing the industry toward standardized electronic submission even for plans that previously required fax or phone PA requests.
Electronic submission allows the practice to confirm the request was received, track its status without a phone call, receive electronic notification when a decision is made, and respond to additional information requests through the same system. Fax-based PA submission produces none of these advantages and creates a higher risk that the request is lost, incomplete, or duplicated.
Step 5: Track the Request and Respond to Information Requests Promptly
After submission, active tracking is the difference between a PA that resolves before the patient’s scheduled service date and one that doesn’t. PA requests don’t process themselves. Payers have review queues. Additional information requests sit unanswered until someone at the practice responds. Approvals are issued but never retrieved because no one logged in to check.
A PA tracking system whether a dedicated software module, a spreadsheet, or a field in the practice management system — shows every open PA request, the submission date, the expected decision date, and any open information requests. Status is checked every one to two business days on any PA approaching the patient’s service date. Information requests are responded to within 24 hours. Approved PAs are retrieved, the authorization number is recorded, and the service is confirmed as schedulable.
Step 6: Record the Authorization Number and Use It on Every Claim
When a PA is approved, the insurer assigns a unique authorization number. This number is the administrative link between the clinical approval and the billing claim. It must appear on every claim submitted for the authorized service during the authorization period.
A claim submitted without the PA number even for a service with a legitimately active authorization — will deny. The denial is not a clinical rejection. It is an administrative one: the claim didn’t include the proof that authorization was obtained. Correcting it requires resubmission with the number added, which takes days. Recording the authorization number, its effective date, and its expiration date in a central PA log at the time of approval, and linking it to the billing workflow for that patient and service, prevents this purely administrative denial category entirely.
When Pre-Authorization Is Denied: The Appeal Pathway
A PA denial is not the end of the road. It is the beginning of an appeal process that, when executed correctly, overturns a substantial portion of initial denials. The failure mode in most practices is not that the appeal process is unsuccessful. It is that approximately 60% of denied PA requests are never appealed at all. The denial arrives, the service is delayed or cancelled, and the practice absorbs the cost without ever presenting the case that would have changed the outcome.
Peer-to-Peer Review: The Fastest Appeal Tool
A peer-to-peer review is a direct conversation between the treating physician and the payer’s medical reviewer. The physician presents the clinical case, addresses the specific denial reason, and provides any additional clinical context that wasn’t captured in the written submission. Peer-to-peer reviews overturn PA denials at rates as high as 75% for services where the clinical necessity is strong and the physician is prepared with the denial rationale and supporting data.
Most payers allow peer-to-peer review requests within 14 to 30 days of the denial notice. Missing this window eliminates the fastest and most effective appeal tool. Every practice should have a protocol that triggers an immediate peer-to-peer review request on receipt of any PA denial, not as a last resort after other options fail.
Formal Written Appeal
When peer-to-peer review is not available or doesn’t resolve the denial, a formal written appeal is the next step. The appeal must address the specific denial reason with new or additional documentation. An appeal that restates the original submission without adding new information rarely succeeds. The appeal letter must identify what the payer said was missing or insufficient and provide documentation that directly addresses that gap.
External Review
If internal appeals fail, most states provide a mechanism for external independent review of PA denials by a neutral clinical reviewer not affiliated with the payer. External review is particularly available for denials based on medical necessity determinations. Many external reviews find in favor of the patient and provider, but the process takes time and is best reserved for high-value services where the clinical case is strong.
What the 2026 CMS Electronic PA Rule Changes
The CMS prior authorization final rule that began taking effect in 2026 is the most significant federal action on pre-authorization administration in years. It requires Medicare Advantage plans, Medicaid managed care organizations, and ACA marketplace plans to implement FHIR-based electronic PA APIs, respond to standard PA requests within 7 calendar days, respond to urgent requests within 72 hours, provide specific denial reasons rather than generic ones, and publicly report their PA approval and denial rates.
For practices, the most immediately useful changes are the response time requirements and the mandatory specific denial reason. A payer that previously took 14 days to respond to a standard PA request is now required to respond within 7 calendar days for applicable plan types. A denial that previously came back with a generic “not medically necessary” code must now include the specific clinical criterion that wasn’t met. Both changes make the PA process faster and the appeals process more targeted.
What the rule does not change is the clinical documentation burden. The requirement for complete, criteria-matching documentation remains entirely the provider’s responsibility. Electronic PA tools speed the submission. They don’t generate the clinical evidence that supports the request. The practice still needs to review payer criteria, gather appropriate documentation, and submit a complete package. The rule just means the payer must review it and respond faster.
Pre-Authorization and Provider Credentialing: The Connection Most Practices Miss
A PA request submitted under a provider not enrolled with the patient’s payer is rejected before clinical review. The payer cannot verify the requesting provider’s credentials or network status, so the request is invalid regardless of how complete the clinical documentation is. For practices adding new providers, PA requests submitted under their NPI before payer enrollment is complete will fail at the administrative gate before any clinical reviewer sees them.
This is a specific and common problem in growing practices where new providers begin seeing patients before their commercial payer credentialing is finished. The clinical team is seeing patients and ordering services. The administrative team is submitting PA requests. The credentialing team is still working through the enrollment applications that take 90 to 120 days to process. PA requests fail not because of clinical documentation gaps but because the provider isn’t yet in the payer’s system.
Related: Provider Credentialing Services |
Building a Pre-Authorization Workflow That Works
Practices that manage PA well treat it as a front-end clinical-administrative function, not a back-end billing reaction. The distinction matters because PA that is managed at the front end — before the service is scheduled prevents the entire category of uncompensated care that results from services delivered without authorization. PA managed reactively, after a service is delivered or after a claim denies, can recover some of that revenue through appeals, but never all of it and always at higher administrative cost.
PA Check at Point of Ordering
The first process control is a PA verification step at the point of ordering or prescribing. Before a surgery is scheduled, before an imaging order is finalized, before a specialty medication is prescribed: does this service require PA for this patient’s specific plan? If yes, initiate the process immediately. If no, document the verification and proceed. This single step prevents the vast majority of no-authorization claim denials.
Criteria-Matched Documentation Templates
For the services your practice requests PA for most frequently, build documentation templates that are mapped to each relevant payer’s clinical criteria. A template for MRI PA includes a prompt for conservative treatment documentation. A template for biologic PA includes step therapy fields with space for each prior drug, dose, duration, and outcome. Templates ensure the submission is complete at first submission rather than triggering follow-up requests.
Centralized PA Tracking
Every open PA request must be visible in a central tracker showing the patient, the service, the payer, the submission date, the expected decision date, any open information requests, and the authorization number and expiration date once approved. The tracker is reviewed daily for any PA approaching the patient’s service date without a decision. It is reviewed monthly for any approved PA approaching expiration.
Denial Response Protocol
Every PA denial triggers an immediate review: can a peer-to-peer review be requested within the payer’s window? If yes, request it the same day the denial is received. If not, initiate a written appeal within the next business day. Assign named accountability for denial follow-through. Denials that sit in a queue waiting for someone to act on them are the 60% that never get appealed.
How Qualigenix Supports Pre-Authorization Management
At Qualigenix, pre-authorization management is integrated into the revenue cycle workflow we manage for practices across 38+ specialties. We maintain the credentialing and enrollment infrastructure that ensures PA requests submitted under our clients’ providers are valid from the start. We track authorization numbers, effective dates, and expiration dates in a centralized system and ensure every claim for an authorized service includes the correct PA number.
Our denial management team processes PA denials with a 72-hour turnaround standard, routing peer-to-peer review opportunities to the physician immediately and initiating formal appeals with documentation directly addressing the denial criteria. We track denial patterns by service type and payer to identify systemic PA issues that require a process change rather than individual claim remediation.
The result is a PA process that catches requirements before the service, submits complete documentation that minimizes additional information requests, and responds to denials fast enough to preserve the appeal options that recover revenue that would otherwise be lost.
Related: Drug Prior Authorization Explained | Prior Auth for Medication in Specialty Practices | What Is Claim Submission in Medical Billing | What Is RCM in Medical Billing
Pre-Authorization Readiness Checklist
- PA requirement verified for each service under each patient’s specific plan before ordering
- Payer clinical criteria reviewed before documentation is gathered for each PA request
- Documentation templates built for frequently requested services mapped to payer criteria
- PA requests submitted electronically with all required fields and documentation
- PA status tracked every 1 to 2 business days until decision received
- Additional information requests responded to within 24 hours
- Authorization number, effective date, and expiration date recorded in PA tracker at approval
- Authorization number included on every claim for the authorized service
- PA renewal initiated before expiration for ongoing or multi-date services
- Peer-to-peer review requested same day on any PA denial within payer’s allowed window
- Written appeal initiated within 1 business day for denials where peer-to-peer is unavailable
- Prescribing or ordering provider confirmed enrolled with patient’s payer before PA submission
Frequently Asked Questions: Health Insurance Pre-Authorization
What is health insurance pre-authorization?
Health insurance pre-authorization is the process of obtaining insurer approval before delivering a specific service, procedure, or medication. The insurer reviews clinical documentation to confirm the service meets their medical necessity criteria and coverage policies. Without approval for services that require it, the insurer will not cover the cost and the financial responsibility falls on the patient or provider. Pre-authorization must be obtained before the service is delivered, not after — retroactive authorization is not available from most payers.
What services commonly require pre-authorization?
Services commonly requiring PA include advanced imaging such as MRI and CT scans, elective surgeries, specialty and high-cost medications, inpatient admissions, durable medical equipment, physical and behavioral health therapy beyond visit limits, outpatient infusions, and genetic testing. Requirements vary by payer and plan. A service that doesn’t require PA under one plan may require it under another. Verifying requirements before each service for each patient’s specific plan is the only reliable approach.
What happens if a service is delivered without pre-authorization?
If a service requiring PA is delivered without one, the insurer will deny the claim regardless of whether the service was clinically appropriate or correctly performed. The denial is administrative, not clinical. The patient may be billed the full cost or the provider may absorb it. Retroactive authorization is possible in limited circumstances but is not a standard payer practice. The cost of delivering a service without authorization — in time, revenue, and patient relationship impact — consistently exceeds the cost of obtaining authorization before the service.
How does the pre-authorization process work?
The PA process starts with identifying the requirement before the service is scheduled, reviewing the payer’s clinical criteria, gathering complete documentation, submitting electronically, tracking to decision, and recording the authorization number for billing. Under CMS 2026 rules, applicable payers must respond to standard requests within 7 calendar days and urgent requests within 72 hours. Incomplete submissions are the leading cause of delays — submitting a complete, criteria-matched package at first submission is the single most effective way to accelerate the process.
Can a pre-authorization denial be appealed?
Yes. PA denials can be appealed through peer-to-peer review, formal written appeal, or external independent review. Peer-to-peer reviews overturn denials at rates up to 75% when the physician presents the clinical case directly. Most payers allow peer-to-peer requests within 14 to 30 days of denial. Approximately 60% of PA denials are never appealed, meaning a majority of recoverable revenue is written off without any attempt at reversal. Every denial should trigger an immediate decision on whether to appeal, not a passive assumption that the denial is final.
Does pre-authorization guarantee payment?
Pre-authorization confirms coverage approval under the patient’s current plan at the time of the request but does not guarantee payment if the patient’s coverage changes, the service billed differs from what was authorized, or the claim contains billing errors. Always verify active coverage on the date of service even with an approved PA. Always confirm the CPT code billed matches the authorized service. Always include the authorization number on the claim. A technically valid authorization that isn’t properly referenced on the claim still produces a denial.
What is the CMS 2026 electronic prior authorization rule?
The CMS 2026 PA rule requires Medicare Advantage, Medicaid managed care, and ACA marketplace plans to implement electronic PA via FHIR APIs, respond to standard requests in 7 days, urgent requests in 72 hours, and provide specific denial reasons. The rule improves turnaround and transparency but does not change the clinical documentation burden — gathering the clinical evidence that supports the request remains entirely the provider’s responsibility. Electronic tools speed submission; they don’t generate the documentation that makes a request approvable.
What is an urgent or expedited pre-authorization?
An urgent PA request is submitted when delaying a service would seriously jeopardize the patient’s health. Payers subject to CMS 2026 rules must respond within 72 hours. The expedited request must include clinical documentation explaining why the standard review timeline creates a risk. Urgent PA is not appropriate for routine services because the standard timeline is clinically acceptable. When the service is genuinely time-sensitive, requesting expedited review with documentation of clinical urgency is both appropriate and required to trigger the faster response.
Related Resources from Qualigenix
- Drug Prior Authorization Explained
- Prior Auth for Medication in Specialty Practices
- What Is Claim Submission in Medical Billing
- What Is RCM in Medical Billing
- Provider Credentialing Services
- Accounts Receivable Medical Billing
- CMS Prior Authorization Final Rule (CMS.gov)
Pre-Authorization Managed Right Is Revenue Protected.
Qualigenix manages the full prior authorization workflow for practices across 38+ specialties — from requirement verification through submission, tracking, approval, and denial appeals — so your clinical decisions translate into collected revenue rather than uncompensated care.
Our team delivers 99% claim accuracy, a 95% first-pass acceptance rate, an average 36-day collection cycle, and a 30% reduction in AR days. We onboard in as few as 6 days.
Precision. Progress. Qualigenix.
What’s Next
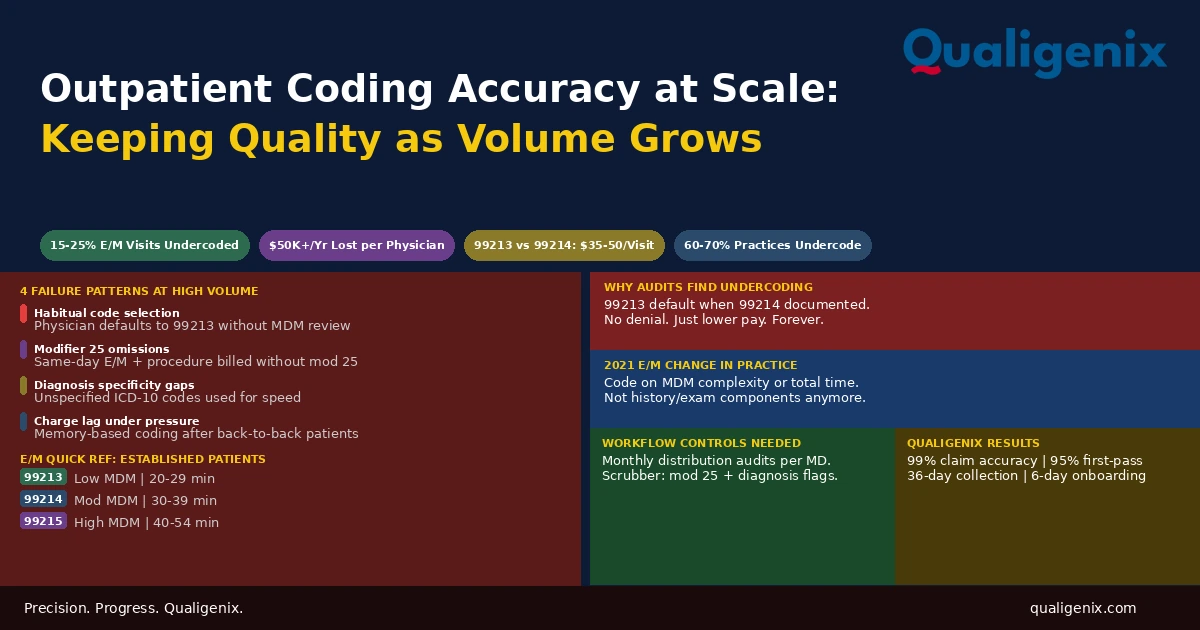
Outpatient Coding for High-Volume Practices: Keeping Accuracy at Scale
Outpatient coding accuracy is manageable when a physician sees 10 patients a day. It degrades predictably when they see...
Medicare Physician Fee Schedule 2026: What Every Practice Must Know
The 2026 Medicare Physician Fee Schedule (CMS-1832-F) introduces two separate conversion factors for the first time: $33.57 for qualifying...
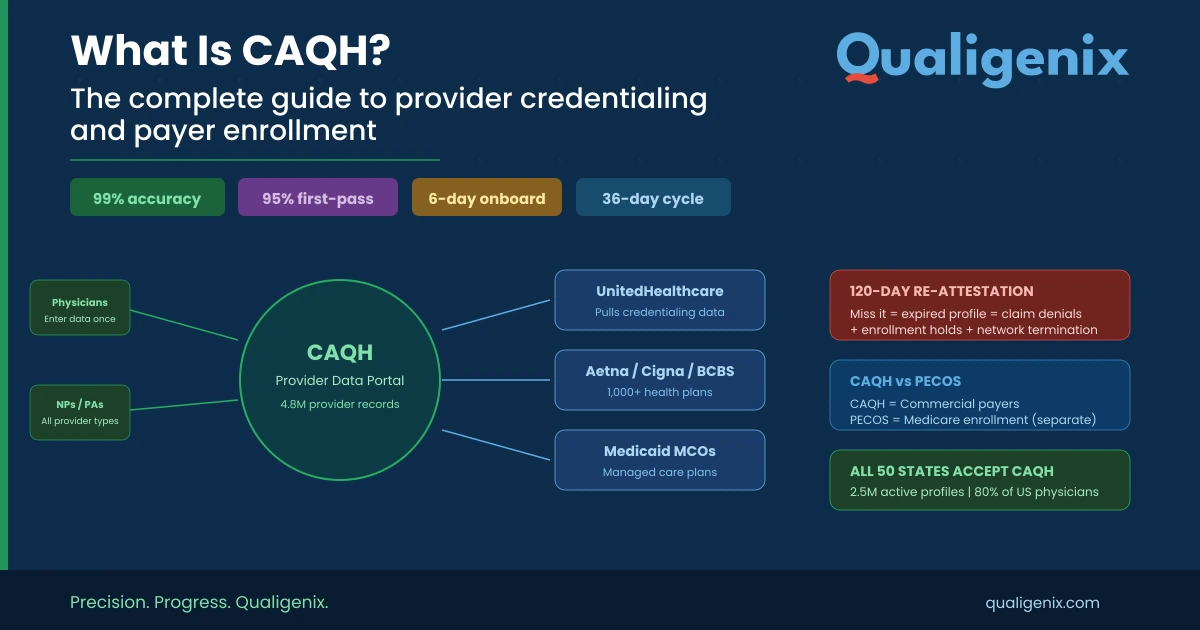
What Is CAQH? The Complete Guide to Provider Credentialing, ProView Setup, and Payer Enrollment
CAQH (Council for Affordable Quality Healthcare) is the centralized credentialing database used by 1,000+ U.S. health plans. Providers register...