Prior Auth for Medication in Specialty Practices: What Changes for High-Cost and Specialty Drugs
The Qualigenix Editorial Team consists of certified billing and coding experts with over 40 years of experience across 38+ medical specialties. Our content is rigorously researched against CMS, AMA, and payer-specific guidelines to ensure total compliance and accuracy. We apply the same elite standards to our resources as we do our client work, consistently delivering high claim accuracy and significant reductions in AR days.
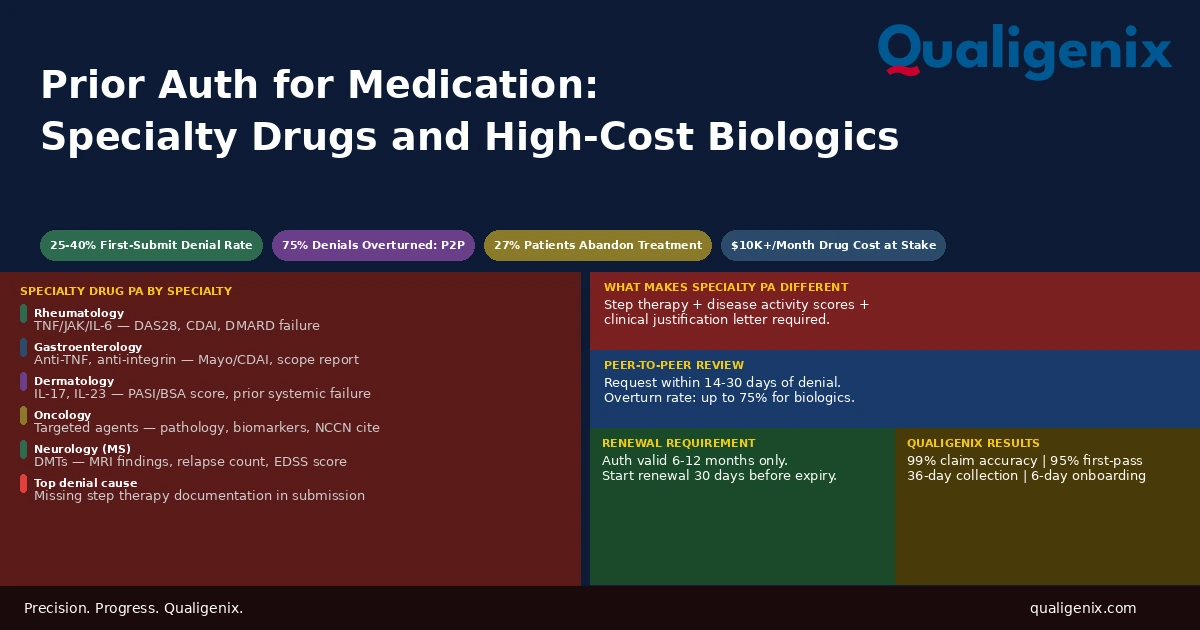
Prior authorization for standard medications is demanding. Prior auth for specialty medications is a different process entirely. Biologics, disease-modifying agents, and high-cost oncology drugs face stricter clinical criteria, mandatory step therapy documentation, higher first-submission denial rates of 25% to 40%, and appeals that require physician-level clinical involvement. Specialty practices that don’t build a dedicated PA workflow for these drugs will see treatment delays, abandoned prescriptions, and denied claims that cost far more to recover than they would have to prevent.
A prior authorization request for a routine medication and a prior authorization request for a biologic are submitted through the same payer portal. They look like the same process from the outside. Inside the payer’s review system, they are handled completely differently, reviewed against different clinical criteria, assigned to different reviewers, and denied for different reasons at different rates.
Specialty practices like rheumatology, gastroenterology, dermatology, oncology, neurology prescribe medications where the monthly cost routinely runs from $600 to $10,000 or more. Payers scrutinize these requests heavily. Step therapy requirements, formulary restrictions, diagnosis-specific coverage criteria, and specialty pharmacy channel requirements all apply simultaneously. The documentation burden is substantially higher than standard drug authorizations, and the consequence of getting it wrong isn’t just a delayed prescription. It’s a patient who can’t start a treatment that may have taken months to reach, and a practice that has to absorb the cost of reworking a denial that should have been approved on the first submission.
This blog covers what actually changes when prior auth for medication crosses into specialty drug territory, what payers require and why, and what a specialty practice’s PA workflow needs to look like to get approvals faster and keep denials lower.
Prior auth for medication in specialty practices requires clinical documentation beyond what standard drug authorizations need: step therapy compliance with documented failure of alternatives, disease activity scores and lab results specific to the drug’s indication, a clinical justification narrative addressing each element of the payer’s medical necessity criteria, and often specialist credentialing confirmation. Specialty drug prior auth denial rates of 25% to 40% on first submission are significantly higher than the 10% to 15% seen for standard medications.
Specialty Drug Prior Authorization: Key Numbers
| Metric | Data Point | Source |
|---|---|---|
| Specialty drug PA denial rate on first submission | 25% to 40% | AMA PA physician survey data |
| Standard medication PA turnaround (CMS 2026 rule) | 7 calendar days for non-urgent | CMS prior authorization final rule |
| Urgent PA turnaround requirement | 72 hours | CMS prior authorization final rule |
| Specialty drug PA processing time in practice | 5 to 14 business days | Specialty pharmacy industry data |
| PA denials overturned after peer-to-peer review | Up to 75% for specialty drugs | AMA prior authorization data |
| Physicians spending 13+ hours per week on PA | 35% of physicians surveyed | AMA 2024 PA survey |
| Patients who abandon treatment due to PA delays | Up to 27% | AMA patient impact survey |
| Average specialty drug monthly cost requiring PA | $600 to $10,000+ per month | Specialty pharmacy pricing data |
| Leading cause of specialty drug PA denial | Missing step therapy documentation | Payer denial code analysis |
| PA requests requiring additional clinical information | Up to 45% of specialty drug requests | Specialty PA processing data |
| Qualigenix first-pass acceptance rate | 95% | Qualigenix performance data |
| Qualigenix claim accuracy rate | 99% | Qualigenix performance data |
| Qualigenix average collection cycle | 36 days | Qualigenix performance data |
| Qualigenix client onboarding time | 6 days | Qualigenix operations data |
What Makes Specialty Drug Prior Auth Different from Standard Medication PA
Every prior authorization for medication involves the same basic elements: the drug name, the patient’s diagnosis, the prescribing provider’s information, and some form of clinical justification. For a standard medication, a short statement that the drug is indicated for the patient’s condition and that the physician recommends it is often sufficient.
For a specialty drug, that’s the starting point, not the finish line. Payers apply detailed clinical criteria developed specifically for each specialty drug category, often drawing on specialty society treatment guidelines, FDA-approved indications, and the payer’s own internal coverage policies. Meeting those criteria requires specific documentation that most practices don’t generate automatically in the course of a routine clinical visit.
The core difference is this: standard drug PA asks whether the medication is appropriate for the patient’s diagnosis. Specialty drug PA asks whether this specific medication is appropriate for this specific patient at this specific point in their treatment history, given what they’ve already tried, what happened when they tried it, and what their current disease activity shows. The documentation requirement reflects that higher bar.
Payers invest heavily in managing specialty drug costs because these medications represent a disproportionate share of pharmacy spend. A single patient on a biologic may cost a payer $30,000 to $100,000 per year. The prior authorization process for specialty drugs is, from the payer’s perspective, a cost management mechanism. From the practice’s perspective, it’s a clinical and administrative burden that sits between a patient and their treatment.
The Specialties Most Affected by Specialty Drug Prior Authorization
Not every specialty manages the same volume of specialty drug PA. The practices that spend the most administrative time on medication prior authorization are those whose standard of care relies on high-cost, complex medications that payers scrutinize most heavily.
Rheumatology
Rheumatology practices prescribe more specialty drug authorizations per provider than almost any other specialty. Biologics for rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis, and lupus include TNF inhibitors, IL-6 inhibitors, JAK inhibitors, and B-cell depleting agents. Every one requires prior authorization with step therapy documentation, disease activity scores, and in many cases specialist confirmation that conventional DMARDs have been tried and failed.
A single rheumatology practice with four physicians may manage 50 to 100 active specialty drug PA requests at any given time, each on a different approval cycle, each requiring renewal every 6 to 12 months. The administrative burden is continuous, not episodic.
Gastroenterology
Gastroenterology practices managing inflammatory bowel disease prescribe biologics and small molecule agents including anti-TNF therapies, integrin inhibitors, and IL-12/23 inhibitors. Step therapy requirements for these drugs are among the most detailed in any specialty, often requiring documented trials of corticosteroids and immunomodulators before the payer will consider a biologic. Endoscopic or imaging evidence of disease activity is frequently required alongside clinical documentation.
Dermatology
Biologics for moderate to severe psoriasis, atopic dermatitis, and hidradenitis suppurativa are among the fastest-growing categories of specialty drug PA in dermatology. Payers typically require a documented body surface area score or validated severity index (such as PASI or IGA), prior treatment with topical agents and conventional systemic therapies, and in some cases phototherapy trials before authorizing a biologic. The documentation requirements are highly specific and differ by both payer and drug.
Oncology
Oncology PA is structurally different from other specialty drug PA because treatment decisions are often time-sensitive and the clinical criteria are based on tumor type, biomarker status, and treatment line rather than step therapy with non-oncology alternatives. Payers require pathology reports, molecular testing results, staging documentation, and NCCN guideline citations. Delays in oncology PA authorization have direct patient safety implications that practices must address through urgent review processes.
Neurology
Neurology practices managing multiple sclerosis, spinal muscular atrophy, and other neurological conditions prescribe some of the highest-cost medications in any specialty. PA requests for disease-modifying therapies for MS require MRI findings, relapse documentation, disability assessment scores, and prior treatment history. Step therapy requirements vary significantly by payer and by MS subtype.
Step Therapy: The Single Biggest Cause of Specialty Drug PA Denials
Step therapy is the requirement that a patient try and fail at least one, and often two or more, preferred or lower-cost medications before the payer will authorize the medication originally prescribed. For specialty drugs, step therapy requirements are detailed, payer-specific, and frequently updated. What one payer requires as a step therapy prerequisite for a biologic may differ entirely from what another payer requires for the same drug in the same indication.
Missing or incomplete step therapy documentation is consistently the top reason specialty drug PA requests are denied on first submission. Practices that submit a PA request for a biologic without fully documenting previous therapy trials in the clinical submission invite an automatic denial even when the patient’s chart clearly shows the treatment history.
Warning: Step therapy documentation in the patient’s chart and step therapy documentation in the PA request are two different things. A patient’s history of failing methotrexate before a biologic may be thoroughly documented across multiple chart notes. If the PA submission doesn’t explicitly extract and present that history in a format that maps to the payer’s step therapy criteria, the payer’s reviewer may not find it or may not count it as meeting the requirement. Specialty drug PA requires active documentation translation, not just a chart reference.
What Complete Step Therapy Documentation Includes
For each prior therapy in the step sequence, the PA submission must show the name of the medication, the dose and duration of the trial, the patient’s clinical response during the trial, the specific reason the therapy was inadequate (insufficient response, adverse reaction, contraindication), and the dates of the trial. Vague statements such as “patient failed prior therapy” without specifics are the most common step therapy documentation failure.
Some payers also require a minimum duration for each step therapy trial before they’ll accept it as a documented failure. A two-week trial of a medication that requires 12 weeks to assess clinical response won’t satisfy a step therapy requirement regardless of how well documented the short trial is. Practices need to know each payer’s minimum trial duration requirements before prescribing the step therapy sequence.
Disease Activity Documentation: What Payers Are Actually Looking For
Beyond step therapy, most specialty drug PA requests require objective evidence of disease activity at the time of the PA request. Payers use this documentation to confirm the patient meets the clinical threshold for the requested medication. The specific measures required vary by specialty and by drug but follow predictable patterns.
| Specialty | Common Drug Categories | Typical Disease Activity Documentation Required |
|---|---|---|
| Rheumatology (RA) | TNF inhibitors, JAK inhibitors, IL-6 inhibitors | DAS28 or CDAI score, tender/swollen joint count, CRP/ESR labs, DMARD failure history |
| Gastroenterology (IBD) | Anti-TNF, anti-integrin, IL-12/23 inhibitors | Endoscopy or imaging report, Mayo or CDAI score, prior steroid/immunomodulator failure |
| Dermatology (Psoriasis) | IL-17, IL-23, IL-12/23 inhibitors | PASI or BSA score, IGA rating, phototherapy and systemic therapy failure documentation |
| Dermatology (Atopic Derm) | IL-4/13 inhibitors, JAK inhibitors | EASI or IGA score, topical corticosteroid failure, prior systemic therapy history |
| Oncology | Targeted agents, immunotherapy, CDK inhibitors | Pathology report, molecular biomarker results, staging, NCCN guideline citation, line of therapy |
| Neurology (MS) | Disease-modifying therapies | MRI findings, relapse count and dates, EDSS score, prior DMT history |
Practices that routinely prescribe specialty drugs need to build the collection of this documentation into their clinical workflow before the PA is submitted, not after the denial arrives requesting additional information. Waiting for a payer to request labs or scoring tools after submission adds 5 to 10 business days to the approval timeline and extends the patient’s treatment delay.
The Clinical Justification Letter: What It Must Address
Most specialty drug PA requests benefit from or require a clinical justification letter written by the prescribing physician. This isn’t a form field. It’s a clinical narrative that maps the patient’s history directly to the payer’s medical necessity criteria for the specific drug.
A strong clinical justification letter for a specialty drug covers four things. First, it states the patient’s diagnosis clearly with supporting evidence, including relevant lab values, imaging findings, or objective clinical measures. Second, it documents the step therapy history, naming each prior therapy, the duration and dose, and the specific outcome that makes the next step medically necessary. Third, it addresses any contraindications to formulary alternatives that the payer may raise as a reason the patient should try a different drug first. Fourth, it explains why the specific medication being requested is the clinically appropriate choice for this patient at this point in their treatment.
Letters that simply state “patient requires biologic therapy” without addressing these specific criteria are the clinical justification equivalent of no letter at all. Payers reviewing specialty drug PA requests are looking for specific criterion-level documentation, not general clinical endorsement.
Peer-to-Peer Review: The Most Effective Recovery Tool After a Denial
When a specialty drug PA is denied, a peer-to-peer review is the most effective and fastest path to overturning the decision. A peer-to-peer is a direct conversation between the prescribing physician and the payer’s medical reviewer, usually a physician in the same or related specialty, where the prescriber can present the clinical case in real time.
The data on peer-to-peer effectiveness for specialty drug denials is striking. Studies and physician surveys consistently show overturn rates of 50% to 75% when peer-to-peer reviews are requested and conducted promptly. That means a physician who invests 20 to 30 minutes in a peer-to-peer call can overturn a denial that would otherwise require a full formal appeal taking two to four weeks.
Most payers allow peer-to-peer review requests within a defined window after the denial, typically 14 to 30 days. Practices that don’t request peer-to-peer reviews promptly, or that assign this task to staff who can’t discuss clinical criteria with a payer’s physician reviewer, lose the most effective tool available for reversing specialty drug denials. The prescribing physician must be available and willing to participate.
Preparing for a peer-to-peer requires the prescribing physician to know the payer’s specific denial reason, the criteria that weren’t met according to the payer, and what additional clinical evidence can address those criteria in the conversation. Walking into a peer-to-peer without this preparation converts a high-overturn-rate opportunity into a confirmation of the denial.
Specialty Pharmacy Channel: The Layer Most Practices Forget
Obtaining prior authorization for a specialty drug doesn’t guarantee the patient can access it. Many payers require specialty drugs to be dispensed through a payer-designated specialty pharmacy rather than a retail pharmacy. This is a separate coordination step from the medical prior authorization, and missing it is one of the most common reasons a patient successfully gets a PA approved but still can’t get their medication.
The specialty pharmacy designation varies by payer and by drug. A payer may require biologic medications for rheumatoid arthritis to go through one specific specialty pharmacy network but allow another drug in the same class to go through a broader network. The practice must confirm the dispensing channel requirement at the same time it confirms the PA requirement, not after the PA is approved.
For medications administered in-office rather than dispensed to the patient, a buy-and-bill model applies. The practice purchases the medication, administers it, and bills the medical benefit rather than the pharmacy benefit. Buy-and-bill medications still require prior authorization, but the process runs through the medical PA system rather than the pharmacy benefit manager, and the reimbursement depends on the practice’s negotiated rate for the drug under their payer contracts.
Renewal: The Part of Specialty Drug PA That Never Ends
Initial specialty drug PA approval is not permanent. Most payers issue specialty drug authorizations for 6 to 12 months and require a renewal submission before the current authorization expires. Renewal submissions require updated clinical documentation showing the patient is responding to the therapy, current labs, and continued medical necessity.
For a specialty practice managing 80 active patients on biologics, this means a continuous renewal workload running alongside new PA submissions. A practice with no tracking system for authorization expiration dates will discover lapsed authorizations when patients show up for infusions or injections and the payer won’t cover them.
Renewal PA submissions should be started 30 days before the current authorization expires. Starting earlier is fine. Starting at the expiration date creates a gap in coverage that may interrupt the patient’s treatment. For patients on continuous biologic therapy, a treatment gap caused by an administrative lapse can have clinical consequences beyond the billing implications.
How Credentialing Affects Medication Prior Authorization
A prescribing provider must be credentialed and enrolled with the patient’s payer to submit a valid prior authorization request. Prior auth requests submitted under a provider not enrolled with the payer are rejected or denied because the payer cannot verify the prescriber’s network status. For specialty drug authorizations, the payer may additionally require that the prescribing provider be a specialist in the relevant field, which is tied directly to their credentialing record.
This creates a specific risk for growing specialty practices. A new rheumatologist joins the practice and begins seeing patients before their enrollment with all payers is complete. The practice submits PA requests for specialty medications under that physician’s NPI. The payers where enrollment is still pending reject the requests. The patient can’t get their biologic. The physician’s credentialing gap created a patient care problem, not just a billing problem.
Related: Provider Credentialing Services | Payer Enrollment Services | Insurance Credentialing for Multi-Provider Practices
Building a Specialty Drug PA Workflow That Reduces Denials
The practices that manage specialty drug PA most effectively share the same operational characteristics. They treat PA as a clinical-administrative function built into the prescribing workflow, not a billing function that happens after the clinical decision.
Pre-Prescription PA Check
Before prescribing a specialty drug, confirm the patient’s payer requires PA, identify the specific clinical criteria the payer applies to that drug, and confirm which step therapy drugs must be documented as tried and failed. This 10-minute check before the prescription is written prevents the most common denial causes from being built into the request from the start.
Criteria-Matched Documentation Templates
Create clinical documentation templates for the specialty drugs your practice prescribes most frequently. Each template prompts collection of the specific data elements the relevant payers require: the disease activity score, the step therapy medications with dates and outcomes, the relevant lab values. Using a template ensures the documentation matches payer criteria rather than general clinical documentation standards.
PA Tracking by Patient and Drug
Maintain a live PA tracker showing every active authorization by patient, including the authorization number, the payer, the drug and dose authorized, the approval date, the expiration date, and the renewal initiation date. Any authorization within 30 days of expiration is flagged for immediate renewal submission.
Dedicated PA Staff with Escalation to Physicians
Administrative staff can manage the submission, follow-up, and tracking functions of specialty drug PA. Clinical escalation to the prescribing physician must happen immediately when a denial arrives or when a peer-to-peer review window opens. Practices that process denials through administrative staff alone without physician involvement lose the peer-to-peer overturn opportunity at high rates.
How Qualigenix Supports Specialty Practices on Prior Authorization
At Qualigenix, we work with specialty practices across 38+ specialties on the full revenue cycle, including the credentialing and enrollment infrastructure that makes prior authorization requests valid and the billing process that follows authorization approval. We ensure that every prescribing provider is enrolled with the relevant payers before PA requests are submitted under their NPI, eliminating the credentialing-related PA rejections that delay patient care.
Our payer enrollment and credentialing team manages the provider-side of the equation so that when a specialty practice submits a PA request, the prescribing provider’s credentials are never the reason it fails. We track enrollment status across all payers, manage CAQH profile maintenance, and handle revalidation cycles so that no credentialing lapse creates a downstream PA problem.
We also manage the full billing cycle that follows authorization approval: claim submission, payment posting, denial management, and AR follow-up, with a 99% claim accuracy rate, 95% first-pass acceptance rate, and 36-day average collection cycle. For specialty practices where authorized high-cost medications represent significant per-claim revenue, our billing accuracy directly protects the investment the practice and patient made in getting the authorization approved.
Related: What Is RCM in Medical Billing | CAQH Profile Management
Prior Auth for Medication: Specialty Drug PA Checklist
- PA requirement and clinical criteria confirmed for specific drug, dose, and payer before prescribing
- Step therapy sequence documented with drug names, doses, durations, and specific failure or adverse reaction outcomes
- Current disease activity score or objective clinical measure collected and included in PA submission
- Relevant lab results current within payer-required timeframe attached to submission
- Clinical justification letter written by prescribing physician addressing each payer medical necessity criterion
- Specialty pharmacy dispensing channel confirmed before PA submission
- PA submitted electronically with confirmation of receipt
- PA status followed up every 2 to 3 business days post-submission
- Peer-to-peer review requested within payer window on any denial
- Renewal submissions initiated 30 days before current authorization expiration
- Prescribing physician confirmed enrolled with patient’s payer before PA submission
Frequently Asked Questions: Prior Auth for Medication
What is prior authorization for medication?
Prior authorization for medication is payer approval obtained before a drug is dispensed or administered, confirming the medication meets coverage criteria and medical necessity standards. Without approval, the payer will not reimburse the drug. For specialty drugs, the process involves more detailed clinical documentation, step therapy requirements, and clinical criteria review than standard medication PA, with denial rates of 25% to 40% on first submission.
What is a specialty drug prior authorization?
Specialty drug prior authorization is the PA process for high-cost biologics, disease-modifying agents, oncology drugs, and other complex therapies typically costing more than $600 per month. It requires detailed clinical documentation including step therapy compliance, disease activity scores, current lab results, and a physician clinical justification narrative. The clinical criteria are drug-specific, payer-specific, and significantly more demanding than standard drug PA requirements.
Why is prior auth for specialty medication denied more often?
Specialty drug PA denies more often because payers apply strict clinical criteria, step therapy requirements, and formulary restrictions that require specific documentation most practices don’t automatically generate. Missing step therapy documentation is the single most common denial reason. Incomplete disease activity scores, diagnosis codes that don’t match the approved indication, and absent clinical justification letters account for most of the rest. All are preventable with a criteria-matched documentation workflow.
What is step therapy in medication prior authorization?
Step therapy requires a patient to try and fail one or more preferred or lower-cost medications before a payer will authorize a more expensive alternative. For specialty drugs, step therapy documentation must name each prior therapy, the dose, the duration, and the specific inadequate outcome. Vague documentation of prior treatment failure without these specifics is treated by payers as incomplete and results in denial even when the patient’s chart clearly shows the treatment history.
How long does prior authorization for specialty medication take?
Specialty drug PA takes 5 to 14 business days in practice, compared to the 7-calendar-day standard set by CMS 2026 rules for non-urgent requests. Delays are most common when clinical documentation is incomplete, when step therapy requirements aren’t addressed, or when the payer routes the request for specialist clinical review. Submitting complete documentation with the initial request and following up every 2 to 3 days reduces the timeline significantly.
What documentation is required for specialty drug prior authorization?
Specialty drug PA requires confirmed diagnosis with ICD-10 codes, step therapy documentation with outcomes, current disease activity scores and relevant labs, a physician clinical justification letter addressing payer medical necessity criteria, and evidence of prior treatment failure or contraindication to alternatives. Biologics often additionally require serology results, genetic markers, or specialty society guideline citations. Requirements vary by drug and by payer and must be verified for each submission.
What is a peer-to-peer review in medication prior authorization?
A peer-to-peer review is a direct conversation between the prescribing physician and the payer’s medical reviewer used to appeal a PA denial, with specialty drug overturn rates of up to 75%. The prescribing physician presents the clinical case in real time, addressing the specific denial reason. Most payers allow peer-to-peer requests within 14 to 30 days of the denial notice. Missing this window converts one of the most effective denial reversal tools into a missed opportunity.
What happens when a prior auth for medication is denied?
When a specialty drug PA is denied, the practice should immediately request a peer-to-peer review within the payer’s allowed window, or submit a formal appeal with additional documentation addressing the specific denial reason. For urgent clinical situations, an expedited reconsideration can be requested. If all payer-level appeals fail, an external independent review may be requested. The fastest path to reversal for most specialty drug denials is the peer-to-peer review, not the formal written appeal.
How does payer credentialing affect medication prior authorization?
A prescribing provider must be credentialed and enrolled with the patient’s payer before a PA request submitted under their NPI is valid. PA requests from non-enrolled providers are rejected before clinical review begins. For specialty practices adding new providers, this means credentialing must be completed with all relevant payers before the new provider begins prescribing specialty medications, or PA rejections will delay patient treatment for the duration of the enrollment gap.
Related Resources from Qualigenix
Specialty Drug PA Denials Start With Credentialing Gaps. We Close Them.
Qualigenix ensures every prescribing provider in your specialty practice is enrolled with the right payers before PA requests go out. We manage credentialing, payer enrollment, and the full billing cycle so authorized specialty medications get claimed, posted, and collected accurately.
Our team delivers 99% claim accuracy, a 95% first-pass acceptance rate, an average 36-day collection cycle, and a 30% reduction in AR days. We onboard in as few as 6 days.
Precision. Progress. Qualigenix.
What’s Next

Medical Coding Errors That Cost Practices the Most (And How to Catch Them Before They Submit)
Medical Coding Errors That Cost Practices the Most (And How to Catch Them Before They Submit) Written by the...
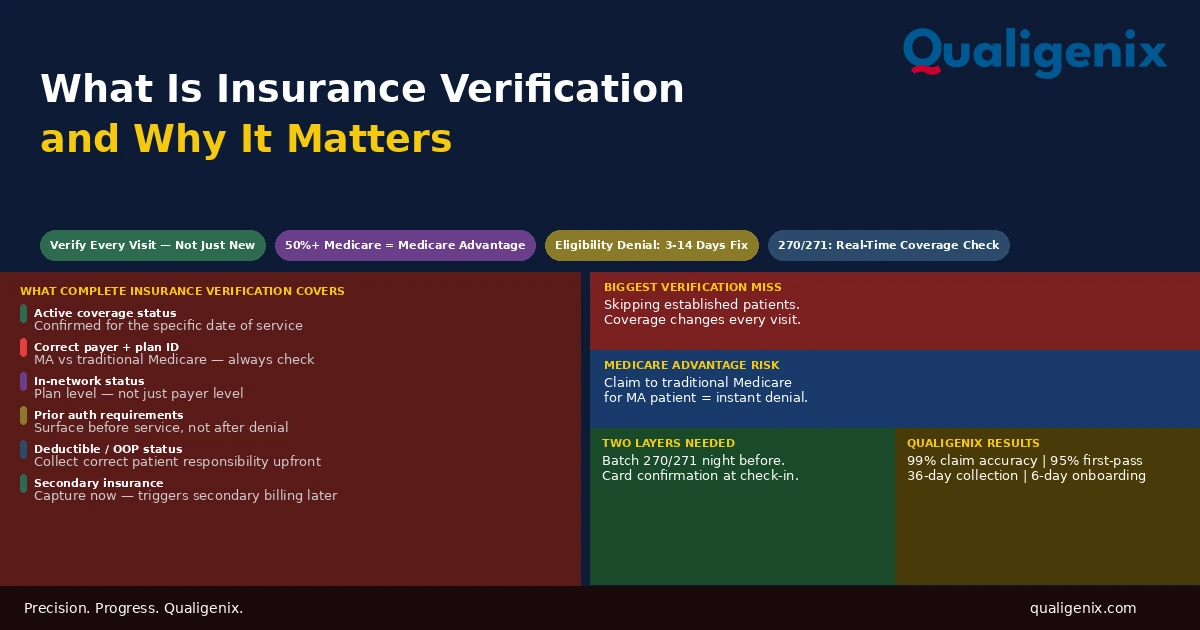
What Is Insurance Verification and Why It Matters
Insurance verification is the front-end process that determines whether a claim will be paid before the patient ever enters...

Insurance Denial Appeals: What Practices Miss
Most insurance denial appeals that fail don’t fail because the clinical case was weak. They fail because the...