Outpatient Coding for High-Volume Practices: Keeping Accuracy at Scale
The Qualigenix Editorial Team consists of certified billing and coding experts with over 40 years of experience across 38+ medical specialties. Our content is rigorously researched against CMS, AMA, and payer-specific guidelines to ensure total compliance and accuracy. We apply the same elite standards to our resources as we do our client work, consistently delivering high claim accuracy and significant reductions in AR days.
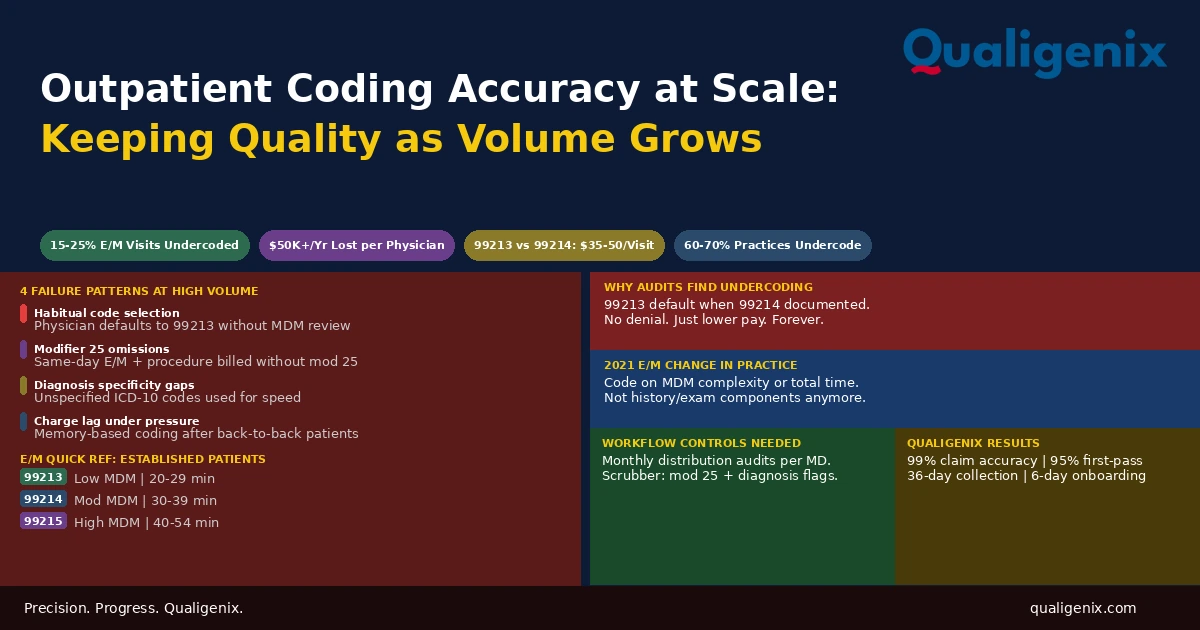
Outpatient coding accuracy is manageable when a physician sees 10 patients a day. It degrades predictably when they see 20 or 25. The degradation isn’t random. It follows specific patterns: physicians default to habitual code levels instead of reviewing complexity, documentation becomes templated and less specific, modifiers get missed on same-day procedure and E/M combinations, and diagnosis codes stay at unspecified levels because no one is checking. Each pattern produces revenue loss that doesn’t show up as a denial. It shows up as a permanently lower reimbursement on every affected claim, compounding across months and years without triggering any alert.
A physician finishing their 22nd patient of the day is not reviewing the MDM complexity of each encounter before selecting an E/M code. They’re selecting the code they’ve selected hundreds of times before and moving to the next note. Most of the time, that code is accurate enough. Some of the time it isn’t. And the gap between what was billed and what the documentation actually supported is revenue that is gone the moment the claim submits.
This is the core problem with outpatient coding at volume. The accuracy standard doesn’t change as volume increases. The process to meet it does. A practice that coded accurately at 12 patients per day and added six more patients per day without changing any of its coding workflows is coding less accurately than it was before, whether or not anyone has measured it yet.
This blog covers how outpatient coding works, why it degrades at scale, what the specific failure patterns look like, and what the workflow controls are that prevent quality from deteriorating as a high-volume practice grows.
Outpatient coding is the assignment of CPT codes, ICD-10 diagnosis codes, and modifiers to physician services in outpatient settings. For most practices, it centers on Evaluation and Management codes selected based on medical decision making complexity or total time under the 2021 AMA guidelines. As patient volume increases, coding accuracy degrades through predictable patterns: E/M undercoding, modifier omissions, diagnosis specificity failures, and charge lag. The revenue impact is invisible in denial reports because undercoded claims pay — they just pay less than they should.
Outpatient Coding at Scale: Key Numbers
| Metric | Data Point | Source |
|---|---|---|
| E/M visits billed below documented complexity level | 15% to 25% of outpatient encounters | Coding audit benchmarks |
| Annual revenue lost to undercoding per physician | $10,000 to $50,000+ depending on specialty | Physician revenue analysis |
| Medicare reimbursement difference: 99213 vs. 99214 | $35 to $50 per visit | CMS Physician Fee Schedule |
| Medicare reimbursement difference: 99214 vs. 99215 | $55 to $75 per visit | CMS Physician Fee Schedule |
| Modifier 25 missing denial rate on same-day claims | Up to 12% of affected encounters | Outpatient billing denial analysis |
| Practices with systematic undercoding identified in audits | Estimated 60% to 70% of multi-physician practices | Medical coding audit surveys |
| Recommended code distribution audit frequency | Monthly per provider | Coding compliance best practices |
| Recommended chart audit sample per physician | 10 to 15 encounters per quarter | OIG compliance guidance |
| Revenue recovery potential from code distribution correction | 15% to 30% of undercoded visit revenue | Post-audit recovery data |
| Qualigenix first-pass acceptance rate | 95% | Qualigenix performance data |
| Qualigenix claim accuracy rate | 99% | Qualigenix performance data |
| Qualigenix average collection cycle | 36 days | Qualigenix performance data |
| Qualigenix client onboarding time | 6 days | Qualigenix operations data |
What Outpatient Coding Covers
Outpatient coding translates a physician’s clinical documentation into the standardized codes that drive billing. CPT codes describe what the physician did during an encounter. ICD-10 diagnosis codes identify the conditions that made the service medically necessary. Modifiers provide additional context about how a service was performed that affects how the payer adjudicates the claim.
For the majority of physician office encounters, the dominant coding category is Evaluation and Management. E/M codes represent the intellectual and clinical work of the physician visit: obtaining history, examining the patient, reviewing data, making decisions, and counseling the patient or coordinating care. The code level selected should reflect the actual complexity of that work as documented in the medical record.
The 2021 AMA revision to E/M coding guidelines changed how that complexity is measured for most outpatient visits. The prior system required counting history and physical examination components. The current system bases code selection on either medical decision making complexity or total time spent on the date of service. This was designed to reduce documentation burden. It also changed what coders and physicians need to know to select accurate code levels, and practices that haven’t fully internalized the new criteria are operating with a mismatch between what they think justifies a code level and what the guidelines actually require.
The Outpatient E/M Code Structure
Understanding which code is appropriate for which encounter requires knowing what the current guidelines require for each level. The table below covers the established patient codes that most outpatient practices use most frequently.
| Code | MDM Level | Time (Total on DOS) | Typical Patient Scenario |
|---|---|---|---|
| 99212 | Straightforward | 10-19 minutes | Single self-limited or minor problem |
| 99213 | Low | 20-29 minutes | 2+ self-limited problems or 1 stable chronic condition |
| 99214 | Moderate | 30-39 minutes | 1+ chronic illness with exacerbation, new problem with workup, or prescription drug management |
| 99215 | High | 40-54 minutes | 1+ chronic illness with severe exacerbation, threat to life, or drug therapy requiring monitoring for toxicity |
The distinction between 99213 and 99214 is where the most revenue loss occurs in high-volume practices. A patient with two or more chronic conditions being actively managed, a patient requiring prescription drug management, or a patient presenting with a new problem requiring additional workup all meet the criteria for 99214 under moderate MDM. Many physicians bill these encounters at 99213 because that’s the code they’ve associated with a “standard visit” in their mental model of coding.
Why Coding Accuracy Degrades at Volume: The Four Failure Patterns
The degradation of outpatient coding accuracy at high volume isn’t mysterious. It follows four specific and predictable failure patterns. Understanding them allows a practice to design the workflow controls that prevent each one before it compounds into significant revenue loss.
Failure Pattern 1: Habitual Code Selection
The most pervasive outpatient coding accuracy problem in high-volume practices is habitual code selection. A physician who sees 22 patients in a day is not conducting a deliberate MDM complexity review for each one. They are moving through the note completion process as efficiently as possible and selecting the code that most of their visits have historically received.
If a physician’s “default” code is 99213 for established patients, that default will be applied even to visits that clearly document moderate MDM: two active chronic conditions managed together, a prescription change with monitoring, a new problem requiring labs or imaging ordered. The documentation supports 99214. The physician bills 99213 because they didn’t stop to assess whether this specific visit crossed the complexity threshold.
Habitual code selection is not intentional undercoding. It is the natural consequence of high volume without a coding review mechanism that triggers at the point of code assignment. The fix is not to slow the physician down. It is to build a feedback loop that surfaces the pattern: monthly code distribution reports that show the physician their own distribution against specialty benchmarks and flag visits where documentation patterns suggest higher complexity than the code assigned.
A 5-physician primary care practice where each physician bills 20% of their established patient visits at 99213 when the documentation supports 99214 loses approximately $70 to $100 per affected encounter in Medicare revenue, and more with higher-paying commercial payers. At 15 affected visits per physician per week, that’s roughly $3,500 to $5,000 in weekly undercollection across the group — over $175,000 annually from a single correction opportunity that produces no denial, no audit flag, and no billing report line item.
Failure Pattern 2: Modifier 25 Omissions on Same-Day Services
When a physician performs both an E/M service and a procedure on the same date of service, modifier 25 must be appended to the E/M code to tell the payer that the E/M was a separate and significant service beyond the pre- and post-work included in the procedure’s global package. Without modifier 25, the payer bundles the E/M into the procedure payment and denies the E/M as a component of the procedure.
In high-volume practices where same-day E/M and procedure combinations are frequent, modifier 25 omissions accumulate fast. A dermatologist who performs a skin biopsy and manages a patient’s psoriasis in the same visit bills a procedure code for the biopsy and an E/M for the psoriasis management. Without modifier 25 on the E/M, the E/M bundles. Across 10 such visits per week, modifier 25 omissions represent a recurring and preventable denial category that billing staff often work individually without identifying the upstream cause.
The fix is a scrubber rule: any claim with both an E/M code and a procedure code on the same date flags for modifier 25 review before submission. This doesn’t require a coder to review every claim manually. It surfaces only the claims where the modifier question is relevant. The coder confirms whether the E/M was separately significant and appends modifier 25 if it was. The claim submits clean rather than generating a denial that requires rework.
Failure Pattern 3: Diagnosis Specificity Failures
ICD-10 requires the most specific diagnosis code available for the patient’s documented condition. General or unspecified codes are appropriate only when the documentation genuinely doesn’t support a more specific one. In practice, unspecified codes appear far more often because they’re faster to assign than looking up the specific code for a laterality qualifier, a stage specification, or a documented etiology.
In high-volume settings, diagnosis coding speed is prioritized over specificity. The result is a pattern of unspecified codes across a coder’s work product that can cause medical necessity denials for procedures with diagnosis-specific coverage criteria, inflate the practice’s reported rate of unspecified diagnoses, reduce clinical data quality for quality reporting, and in post-payment audit scenarios, create documentation gaps between the diagnosis billed and the treatment delivered.
The most common specificity failures in outpatient coding are using unspecified laterality codes when the chart documents right or left, using unspecified encounter type codes when the chart documents initial, subsequent, or sequela, and using unspecified diabetes codes when the chart documents type 1 or type 2 with documented complications. Each of these has a specific code that the documentation supports. Each unspecified code represents a missed opportunity for accurate billing and defensible documentation.
Failure Pattern 4: Charge Lag Under Pressure
At high volume, the time available for note completion and charge entry compresses. Physicians who are seeing patients back to back often complete their notes and enter charges in a batch at the end of the day or the next morning. At peak volume, some practices fall into end-of-week batching, where charges for Monday through Thursday are entered on Friday.
This charge lag creates two coding accuracy problems. First, memory-based coding is less accurate than documentation-based coding. A physician entering charges for a Tuesday patient on Thursday afternoon is coding from a partial memory of the encounter rather than a focused review of the note. The code assigned reflects the general impression of the visit rather than the documented MDM complexity. Second, charge lag creates timely filing exposure for the portion of commercial payers with 90-to-180-day filing windows. It also delays the entire revenue cycle downstream.
Warning: Memory-based charge entry is consistently less accurate than documentation-based entry. The specific elements of MDM that would justify a 99214 — the number of diagnoses managed, the specific data reviewed, the risk level of the decision made — are not well-retained in memory after a full day of patient encounters. A physician coding from memory at the end of a 22-patient day defaults to their habitual code level. A physician coding with the note open in front of them is more likely to review complexity and assign the appropriate level.
The Outpatient E/M Code Distribution Audit: The Fastest Accuracy Signal Available
A code distribution audit doesn’t require reviewing a single chart. It requires pulling one report: the distribution of E/M codes billed by each physician over the prior month, expressed as a percentage of total established and new patient visits.
Compare each physician’s distribution against specialty benchmarks. If a primary care physician’s established patient distribution shows 65% at 99213, 25% at 99214, 5% at 99212, and 5% at 99215, that distribution is below the benchmark for primary care practices managing patients with chronic conditions. The bell curve should be centered at 99214 for a primary care practice treating an adult panel with multiple chronic conditions.
When a physician’s distribution is significantly shifted toward lower codes than the benchmark, it doesn’t prove undercoding. It signals a pattern that requires chart review to confirm. Pull 15 charts from the physician’s 99213 encounters in the prior month. Review each against the 2021 MDM criteria. If 40% of those charts document encounters that meet 99214 criteria — moderate MDM with two active problems or prescription management — the audit has identified a systematic coding gap that, when corrected through physician education and documentation improvement, will produce a measurable revenue improvement on every future affected encounter.
What the 2021 E/M Changes Mean for High-Volume Practices in 2026
The 2021 AMA E/M guideline revision eliminated the requirement to document specific history and exam components for most outpatient E/M code levels. The code is now determined by MDM complexity or total time. This was implemented five years ago. Practices that understood the change at the time and retrained their physicians and coders are billing more accurately and more completely under the new framework. Practices that didn’t have fully updated their habits without updating their criteria.
The most common post-2021 coding gap is physicians who document thorough history and physical exams out of habit but don’t explicitly document the MDM elements that actually determine code level. The documentation is thorough. The problem is that it doesn’t clearly establish the number of diagnoses being managed, the data being reviewed and its complexity, or the risk level of the clinical decision. A coder reviewing the note can make inferences, but without explicit MDM documentation, they default to a lower code to stay defensible.
Practices that want to capture the full value of the 2021 changes in 2026 need one thing: physicians who understand what MDM documentation looks like and include it consistently in their notes. A single element — a sentence in the assessment explicitly identifying the diagnoses managed and the decision made — can shift an encounter from 99213 to 99214 documentation, reflecting the clinical work that was already performed but wasn’t documented in a way that supports the higher code.
Modifier and Linkage Controls That Prevent Silent Revenue Loss
Beyond E/M code level, outpatient coding accuracy depends on modifiers and diagnosis linkage. Both can be controlled through claim scrubber rules that catch errors before submission rather than after a payer denial.
Modifier 25 and 59 Rules
Configure the claim scrubber to flag any claim where an E/M code and a procedure code appear together on the same date without modifier 25. The flag doesn’t deny the claim internally. It routes it to a coder for confirmation that the E/M was separately significant before the modifier is appended. For practices where same-day procedure and E/M combinations are common, this rule prevents a systematic denial category without adding manual review time to every claim.
Modifier 59 (distinct procedural service) requires similar attention. When two procedure codes are billed together that payers would normally bundle, modifier 59 signals they were distinct services on separate anatomical sites or in distinct encounters. Using modifier 59 incorrectly is an unbundling error. Not using it when the services were genuinely distinct produces a bundling denial. Scrubber rules that flag modifier 59 candidates for coder review improve accuracy in both directions.
Diagnosis Linkage Review
Configure the billing system to require explicit diagnosis-to-procedure linkage on every claim. Every procedure line item must have at least one diagnosis code attached that explains its medical necessity. Where possible, build automatic diagnosis linkage suggestions based on prior claims for the same physician and procedure combination. Flag claims where a procedure is linked to an unspecified diagnosis code as a review item before submission, particularly for procedures with diagnosis-specific coverage criteria.
Building a Coding Feedback Loop That Works at Volume
The structural challenge of outpatient coding accuracy at scale is that the people generating the documentation (physicians) and the people reviewing it for coding accuracy (coders or billing staff) are working in different contexts and at different speeds. Feedback loops that are too slow, too infrequent, or too abstract don’t change physician behavior. Feedback loops that are specific, timely, and connected to real chart examples do.
A functional coding feedback loop for a high-volume outpatient practice has four components. First, monthly code distribution reports that show each physician their own distribution relative to peers and benchmarks. This should take 10 minutes to review and should be delivered directly to the physician, not filtered through an intermediary. Second, quarterly chart audit results with specific examples: these three charts from your 99213 encounters would have supported 99214 under moderate MDM criteria. Third, a mechanism for coders to flag documentation questions to the physician the same day rather than at a monthly meeting. Fourth, annual group training on current E/M guidelines using real examples from the practice’s own charts.
The practices that maintain outpatient coding accuracy at high volume are not necessarily the ones with the most experienced coders. They are the ones with the most functional feedback loops between clinical documentation and coding review.
How Qualigenix Manages Outpatient Coding Accuracy
At Qualigenix, outpatient coding accuracy is a monitored operational standard, not an assumed output. We run monthly code distribution reports for every physician across every client practice, flagging distributions that deviate from specialty benchmarks and triggering targeted chart reviews for the providers where the pattern suggests systematic undercoding.
Our coders apply the 2021 E/M MDM criteria to every outpatient visit, reviewing documentation for the three MDM elements that determine code level. When the documentation supports a higher code than was initially assigned, we code to the documentation. When the documentation is insufficient to support the apparent complexity of the visit, we route a query to the physician rather than defaulting to a conservative code that leaves revenue behind.
We configure modifier rules and diagnosis linkage checks in every client’s claim scrubber, catching same-day service combinations and unspecified diagnosis issues before submission. Our denial management team traces outpatient coding-related denials to their root cause and feeds the finding back to the coding and documentation process rather than just working the individual denial.
Our results reflect coding that stays accurate as volume scales: 99% claim accuracy rate, 95% first-pass acceptance rate, 36-day average collection cycle, and 30% reduction in AR days. We onboard new clients in as few as 6 days.
Related: What Is Physician Billing | Charge Capture for High-Volume Specialties | What Is RCM in Medical Billing
Outpatient Coding Accuracy Checklist
- Monthly E/M code distribution reports run per physician and compared to specialty benchmarks
- Quarterly chart audits sampling 10 to 15 encounters per physician against 2021 MDM criteria
- Audit findings delivered to each physician with specific chart examples within 2 weeks
- Scrubber rule configured to flag same-date E/M and procedure combinations without modifier 25
- Scrubber rule configured to flag procedure codes linked to unspecified ICD-10 diagnosis codes
- Charge entry standard of 24 hours enforced to prevent memory-based coding from delayed entry
- Coder-to-physician query process in place with same-day or next-day resolution turnaround
- Annual group training on current AMA E/M guidelines using practice’s own chart examples
- New physician onboarding includes E/M coding orientation before first billable patient encounter
- Denial codes related to bundling and medical necessity reviewed monthly for coding root cause patterns
Frequently Asked Questions: Outpatient Coding
What is outpatient coding?
Outpatient coding is the assignment of CPT procedure codes, ICD-10 diagnosis codes, and modifiers to physician services delivered in outpatient settings. For most physician practices, it centers on Evaluation and Management codes selected based on medical decision making complexity or total time under the 2021 AMA guidelines. Code accuracy directly determines the reimbursement received for every outpatient encounter and reflects the integrity of the practice’s clinical documentation.
How does outpatient coding differ from inpatient coding?
Outpatient coding uses CPT codes on the CMS-1500 form under the physician’s NPI, with E/M code selection based on medical decision making or total time. Inpatient coding uses ICD-10-PCS procedure codes on the UB-04 and is primarily a facility coding function. Outpatient E/M codes range from 99202 to 99215 for office visits. Inpatient E/M codes follow different criteria for admission, subsequent visits, and discharge. Documentation requirements and reimbursement structures differ substantially between the two settings.
What is outpatient E/M undercoding and how much does it cost?
Outpatient E/M undercoding is selecting a lower-level CPT code than the documentation supports, resulting in lower reimbursement than the practice is entitled to on every affected encounter. Research shows 15% to 25% of outpatient visits are undercoded. The annual revenue impact per physician ranges from $10,000 to $50,000 depending on specialty and volume. Undercoding produces no denial and no audit flag. The claim pays at the lower rate without any signal that revenue was left behind, making it invisible without a code distribution audit.
What is a code distribution audit in outpatient coding?
A code distribution audit analyzes the E/M codes a physician bills over a period, compared to specialty benchmarks for what the distribution should look like. It identifies systematic undercoding patterns without reviewing individual charts. When a physician’s distribution is shifted significantly toward lower codes than peers in the same specialty, the audit flags a subset of charts for review. If those charts show documentation supporting higher code levels, the finding confirms a coding gap that can be corrected prospectively through physician education.
What is modifier 25 and why does it matter for outpatient coding?
Modifier 25 signals that a significant, separately identifiable E/M service was performed on the same day as a procedure by the same physician. Without it, the payer bundles the E/M into the procedure payment and denies the separate E/M charge. In high-volume practices with frequent same-day procedure and visit combinations, missing modifier 25 generates a recurring denial category. A scrubber rule that flags same-date E/M and procedure combinations before submission catches this before it becomes a denial pattern.
How does patient volume affect outpatient coding accuracy?
As volume increases, coding accuracy degrades through habitual code selection, rushed charge entry, modifier omissions, and diagnosis specificity failures — all compounding simultaneously without any of them triggering a denial or alert. A practice that coded accurately at lower volume and increased patient throughput without changing its coding workflow is coding less accurately than before. The degradation is invisible in denial reports because undercoded visits pay. The only way to surface it is a code distribution audit comparing current patterns against benchmarks.
What workflow controls prevent outpatient coding degradation at scale?
The controls that prevent outpatient coding accuracy from degrading at scale are monthly code distribution reports per physician, quarterly chart audits with direct physician feedback, scrubber rules for modifier 25 and diagnosis specificity, a 24-hour charge entry standard, and annual E/M guideline training using the practice’s own charts. None requires adding staff. All require process discipline that most high-volume practices have deprioritized in favor of throughput, and all produce measurable revenue improvement when implemented consistently.
Related Resources from Qualigenix
- Charge Capture for High-Volume Specialties
- What Is RCM in Medical Billing
- What Is Claim Submission in Medical Billing
- Provider Credentialing Services
- Accounts Receivable Medical Billing
- AMA CPT E/M Guidelines (AMA-ASSN.org)
Your Volume Is Growing. Your Coding Accuracy Should Too.
Qualigenix manages outpatient coding accuracy for practices across 38+ specialties, running monthly code distribution audits, applying current E/M MDM criteria, and building the scrubber controls that prevent modifier and diagnosis errors before they become denials or permanent revenue losses.
Our team delivers 99% claim accuracy, a 95% first-pass acceptance rate, an average 36-day collection cycle, and a 30% reduction in AR days. We onboard in as few as 6 days.
Precision. Progress. Qualigenix.
What’s Next
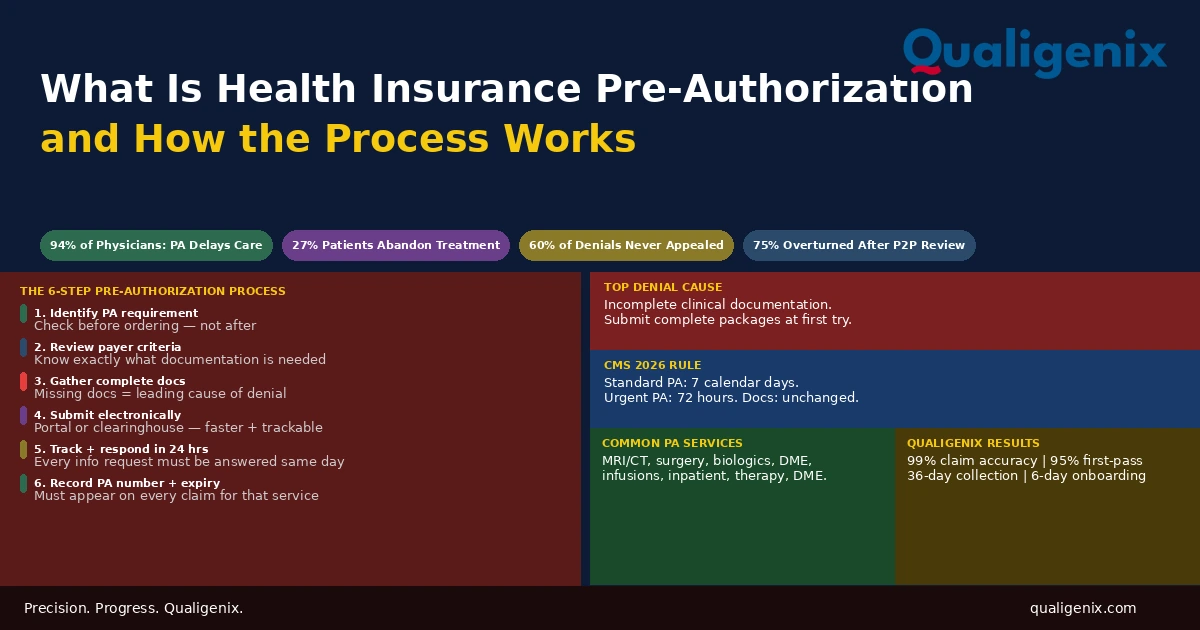
What Is Health Insurance Pre-Authorization and How It Works
Health insurance pre-authorization is the approval step that sits between a physician’s clinical decision and a patient’s access to...
Medicare Physician Fee Schedule 2026: What Every Practice Must Know
The 2026 Medicare Physician Fee Schedule (CMS-1832-F) introduces two separate conversion factors for the first time: $33.57 for qualifying...
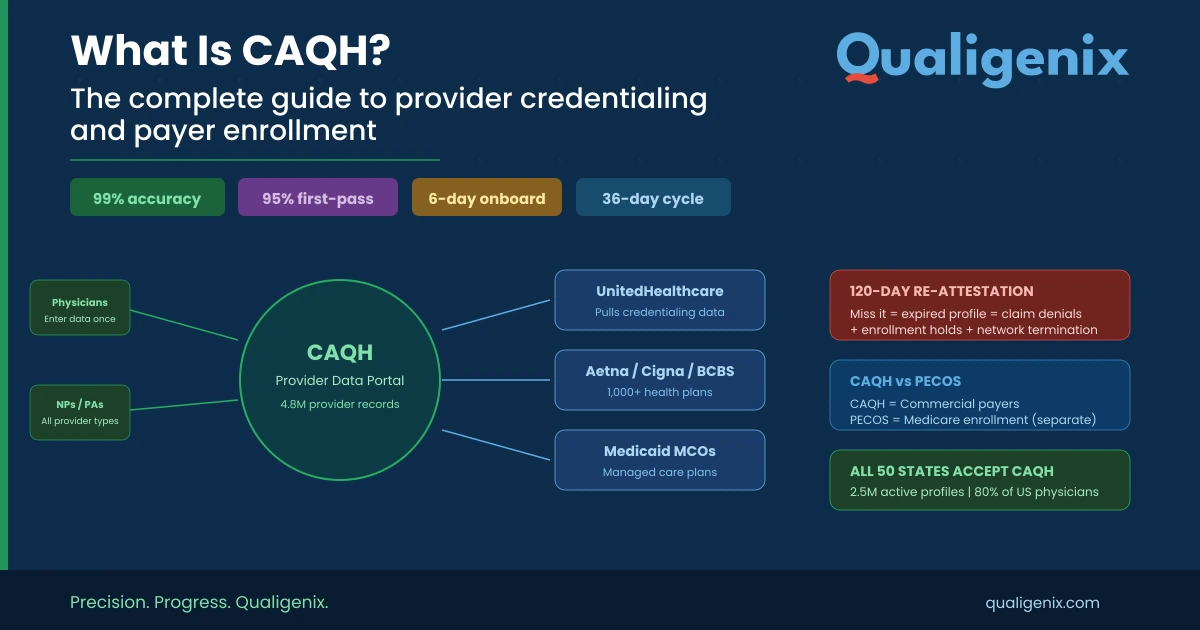
What Is CAQH? The Complete Guide to Provider Credentialing, ProView Setup, and Payer Enrollment
CAQH (Council for Affordable Quality Healthcare) is the centralized credentialing database used by 1,000+ U.S. health plans. Providers register...