Orthopedic Billing: Complete Guide 2026
The Qualigenix Editorial Team consists of certified billing and coding experts with over 40 years of experience across 38+ medical specialties. Our content is rigorously researched against CMS, AMA, and payer-specific guidelines to ensure total compliance and accuracy. We apply the same elite standards to our resources as we do our client work, consistently delivering high claim accuracy and significant reductions in AR days.
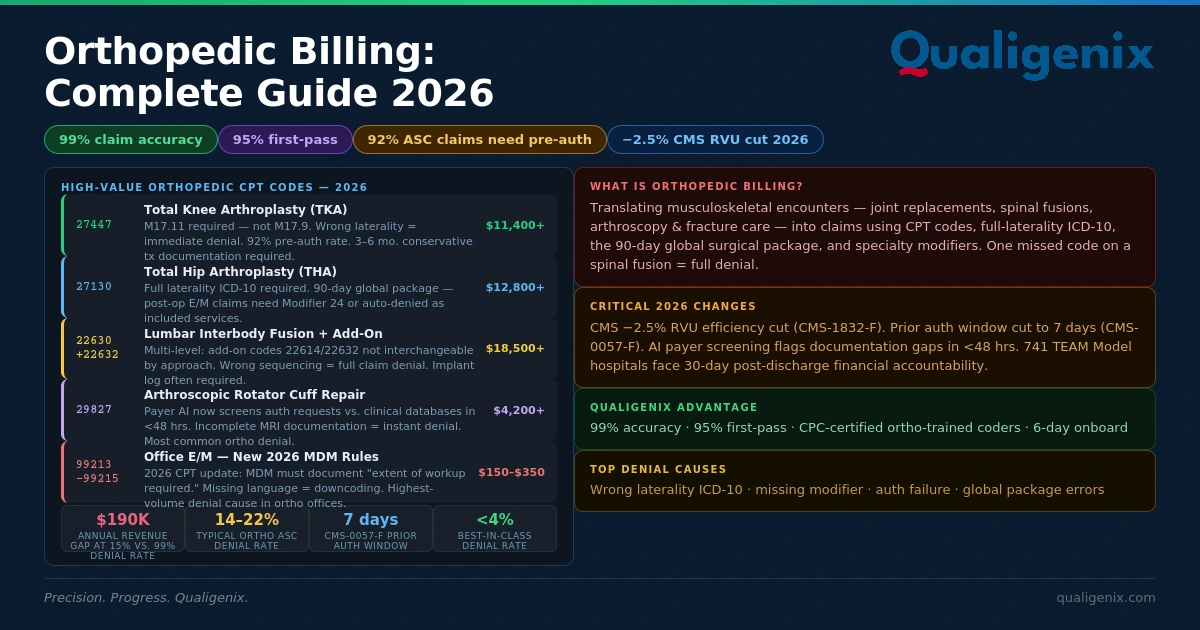
Orthopedic billing is unforgiving. A total knee replacement claim (CPT 27447) worth $11,400 or more can be denied outright because someone coded M17.9 instead of M17.11. In 2026, 92% of orthopedic ASC claims require pre-authorization, payers now use AI to flag documentation gaps in under 48 hours, and the CMS −2.5% work RVU cut means every denial costs more than it did last year. Practices maintaining orthopedic claim denial rates below 5% collect $190,000 more annually on identical procedure volume than those running at 10–15%.
Here’s the number that should be on every orthopedic practice administrator’s radar right now: $190,000. That’s the annual revenue difference between an orthopedic practice operating at a 99% first-pass clean claim rate and one running at a typical 10–15% denial rate – on the exact same procedure volume (ADS, 2026). Not one additional patient. Not one additional surgery. The same OR schedule, the same providers, the same payer mix – just dramatically different billing performance. That gap isn’t driven by luck or payer favoritism. It’s entirely driven by coding accuracy, documentation quality, and billing process discipline.
Orthopedic billing sits at the intersection of high complexity and high stakes. A single spinal fusion case might require five or six separate CPT codes – the primary procedure, multiple add-on codes for additional levels, modifier applications for approach type and laterality, and an implant cost report that some payers require alongside the claim. Miss one code, misapply one modifier, or document the operative note without the specific anatomical detail the payer’s medical necessity criteria require, and that claim denies. The denial-to-collection cycle in orthopedics averages 45–60 days with a recovery rate of only 70% (ADS, 2026). What doesn’t get recovered gets written off – quietly, month after month.
The 2026 environment makes all of this harder, not easier. The CMS Physician Fee Schedule Final Rule (CMS-1832-F) applied a −2.5% efficiency adjustment to orthopedic surgical work RVUs effective January 1, 2026. The CMS-0057-F Prior Authorization Rule cut payer decision windows in half – which sounds helpful until you realize faster decisions also mean faster denials when documentation is incomplete. AI-driven payer review systems now screen authorization requests against clinical databases before a human reviewer sees them, rejecting documentation gaps that a phone call used to smooth over. This guide covers every dimension of orthopedic billing – CPT codes, modifiers, the 90-day global surgical package, prior authorization workflows, ICD-10 specificity requirements, the top denial causes, and how Qualigenix orthopedic billing services achieve 99% claim accuracy and 95% first-pass acceptance across surgical and non-surgical orthopedic practices.
What Is Orthopedic Billing?
Orthopedic billing is the process of translating musculoskeletal clinical encounters — office visits, diagnostic imaging, arthroscopic procedures, joint replacements, spinal surgeries, and fracture care — into accurate insurance claims using CPT procedure codes, ICD-10-CM diagnosis codes with full laterality, and specialty modifiers. It’s one of the most complex billing specialties in US healthcare because it requires mastery of the 90-day global surgical package, multi-code spinal procedures, bilateral procedure rules, strict ICD-10 specificity, and an increasingly demanding prior authorization environment.
What makes orthopedic billing genuinely different from general medical billing isn’t just the complexity of the codes — it’s the density of decisions required on every single claim. Think about what it takes to bill a multi-level lumbar fusion correctly: you need the right primary code for the first level based on approach type, the right add-on codes for each additional level (which are not interchangeable across approaches), the correct modifier for laterality or bilateral involvement, a diagnosis code specific enough to establish medical necessity, documentation of conservative treatment failure if the payer requires it for authorization, and an implant log that some payers want attached directly to the claim. Get any one of those elements wrong and the whole claim denies.
Payer AI systems now evaluate authorization requests against clinical criteria databases automatically — and they’re doing it in hours, not days. Incomplete documentation doesn’t get a phone call anymore. It gets an immediate denial. The 90-day global surgical package, which bundles pre-op and post-op care into one surgical reimbursement, continues to generate significant revenue leakage when practices bill included services separately without the correct modifier. (And yes, this happens in practices that have been running orthopedic billing for years.)
Orthopedic Billing: Key Statistics and Benchmarks 2026
| Metric | Value / Benchmark |
|---|---|
| Revenue difference — 99% vs. 10–15% denial rate (same volume) | ~$190,000 annually (ADS, 2026) |
| Orthopedic ASC claims requiring pre-authorization | 92% — highest pre-auth burden of any surgical specialty |
| Medicare Advantage orthopedic prior auth denial rate (2025) | 7.4% — up from 5.9% in 2023 (Medical Billers and Coders, 2026) |
| Typical orthopedic ASC denial rate | 14–22% (vs. 11.8% industry average) |
| Best-in-class orthopedic denial rate | Under 4% — achievable with specialized orthopedic billing workflows |
| Revenue at risk per denied TKA claim (CPT 27447) | $11,400+ per claim (Medical Billers and Coders, 2026) |
| 2026 CMS PFS RVU adjustment (CMS-1832-F) | −2.5% efficiency adjustment to orthopedic surgical work RVUs (effective Jan 1, 2026) |
| CMS-0057-F prior auth decision window (standard) | 7 calendar days (effective Jan 1, 2026) — down from 14 days |
| CMS-0057-F prior auth decision window (urgent) | 72 hours (effective Jan 1, 2026) |
| Denial-to-collection cycle (orthopedic) | 45–60 days with 70% recovery rate — remainder delayed, reduced, or written off |
| Conservative treatment documentation failure for joint replacement | 3–6 months of documented failure required by most commercial payers before authorization |
| TEAM Model hospitals (active Jan 1, 2026) | 741 acute care hospitals bearing 30-day post-discharge financial accountability (CMS, 2026) |
| Qualigenix claim accuracy rate | 99% — CPC-certified orthopedic-trained coders with specialty-specific workflows |
| Qualigenix first-pass acceptance rate | 95% — across all orthopedic procedures and payer types |
| Qualigenix average onboarding time | 6 days — from engagement to active billing management |
What Are the Major Orthopedic CPT Code Changes for 2026?
The 2026 CPT update cycle introduced 418 total changes across all specialties — and musculoskeletal, spine, and remote monitoring services were among the most significantly affected (AMA, 2026). For orthopedic practices, the changes aren’t minor tweaks to code descriptions. They’re structural shifts that affect how multi-level spinal fusion cases are coded, how fracture care revenue is captured, and what your charge master looks like if it hasn’t been updated since December 2025.
Spinal Fusion Coding: Multi-Level Rules Tightened
The 2026 CPT cycle updated coding rules for multi-level spinal fusion with refined guidance on sequencing and add-on code selection. Posterior lumbar interbody fusion (22630) and posterolateral fusion (22612) each have specific add-on codes for additional levels — they’re not interchangeable. Mixing them produces billing errors that some payers pay quietly and others deny outright. Add-on code sequencing also matters: the primary procedure code must be listed first with add-on codes following in sequence. And critically: never apply Modifier 51 to add-on codes. Add-on codes carry the multiple procedure relationship by definition. Applying Modifier 51 triggers an inappropriate additional payment reduction that compounds into significant annual underpayment for high-volume spine practices. Additionally, anterior cervical discectomy and fusion (22551, 22552) use different add-on code structures than lumbar procedures — verify that your charge master reflects the correct level-specific add-ons for each spinal region.
Arthroplasty Revision Coding: Documentation Defines the Code
The 2025–2026 CPT update cycles refined the definitions for arthroplasty revision procedures. Practices billing revision knee arthroplasty (27487) and revision hip arthroplasty (27134, 27137, 27138) must ensure their documentation aligns with the updated definitions — specifically, the criteria distinguishing complete revision from partial revision. Practices performing complete revision arthroplasty without operative note templates that explicitly document which components were exchanged risk being downcoded to partial revision reimbursement. The operative note must document the failure mechanism, the condition of the implants removed, and the clinical rationale for the revision approach. Most commercial payers and Medicare Advantage plans require separate authorization for revision arthroplasty — even when the original procedure was previously authorized. Don’t assume the primary auth carries over.
Fracture Care: Clarified Documentation Thresholds
The 2026 CPT cycle clarified documentation requirements for distinguishing between closed treatment with and without manipulation — a distinction that was frequently disputed by payers under the prior code language. Documentation must describe the manipulation technique, the pre- and post-manipulation alignment, and the immobilization method applied. Vague documentation of “fracture reduced” no longer satisfies 2026 definition requirements. Additionally, injury diagnosis codes require the 7th character at every orthopedic encounter — A (initial), D (subsequent), S (sequela). The initial cast application (A) and the 6-week cast removal visit (D) require different 7th characters on the same ICD-10 code. Distinct codes also exist for displacement status (displaced vs. non-displaced) and treatment method — the fracture description must explicitly address both.
What Are the Essential CPT Codes for Orthopedic Billing?
Orthopedic CPT codes span four categories — evaluation and management, diagnostic procedures, surgical procedures, and physical medicine — each with its own modifier requirements and documentation standards. The table below covers the highest-volume codes across joint replacement, arthroscopy, spine, and fracture care.
| CPT Code | Description | Documentation Required | Key Modifier / Pairing Notes |
|---|---|---|---|
| 27447 | Total knee arthroplasty (TKA) | 3–6 months conservative treatment failure; functional limitation; pre-op XR with OA grading; implant log | RT or LT; bilateral = Mod 50; requires pre-auth from virtually every commercial payer and MA plan |
| 27130 | Total hip arthroplasty (THA) | Conservative treatment failure; functional limitation; pre-op XR; approach documented (posterior, anterior, lateral) | RT or LT; bilateral = Mod 50; implant cost documentation for many payers |
| 27446 | Partial knee replacement (unicompartmental) | Single-compartment OA on XR/MRI; functional limitation; component-specific implant documentation | RT or LT; requires M17.31 or M17.32 — not M17.11 |
| 29881 | Knee arthroscopy with meniscectomy | MRI confirming tear; mechanical symptoms; laterality documented; extent of tear noted | RT or LT; Mod 59 needed if chondroplasty (29877) billed in same session |
| 22612 | Posterolateral lumbar fusion (PLF) — single level | Imaging confirming instability; failed conservative care with dates; level(s) specified | 22614 as add-on per additional level; Mod 51 never on add-on codes |
| 22630 | PLIF — posterior lumbar interbody fusion | Same as PLF; plus documentation of disc pathology and approach rationale | 22632 for each additional level — not interchangeable with 22614 |
| 27487 | Revision total knee — both components | Failure mechanism documented; components exchanged listed; implant removal and replacement log | RT or LT; requires separate pre-auth from primary TKA authorization |
| 99213–99215 | Established patient E/M — orthopedic office visit | MDM complexity or total time documented; chronic condition management note specificity | Mod 25 required when E/M is billed same day as a procedure |
What Is the 90-Day Global Surgical Package and Why Does It Keep Causing Denials?
The 90-day global surgical package is one of the most misunderstood concepts in orthopedic billing — and that misunderstanding costs practices real money every month. When a surgeon performs a major procedure (defined as any procedure with a 90-day global period), Medicare and most commercial payers bundle together the pre-operative visit one day before surgery, the surgery itself, and all routine post-operative care within 90 days into a single global reimbursement. Billing any of those included services separately — without the right modifier — generates an automatic denial.
What’s Included in the Global Period (and What Isn’t)
Services included in the global payment that you cannot bill separately include: the pre-operative evaluation one day before surgery, the surgical procedure itself, immediate post-op care in the recovery area, routine follow-up visits related to the surgery within 90 days, and management of standard post-operative complications that don’t require a return to the OR. What you can bill separately — with the right modifier — includes: E/M visits for conditions unrelated to the surgery (Modifier 24), return to the OR for a related complication (Modifier 78), and an unrelated surgical procedure performed during the global window (Modifier 79).
The Global Period Revenue Leak Nobody Talks About
The more common problem isn’t billing included services separately — it’s the reverse. Many orthopedic practices lose revenue by failing to use Modifier 24 when they should. A patient comes in six weeks after a knee replacement complaining of a new-onset rash. That’s an unrelated condition. It belongs on a separately billable E/M with Modifier 24. Without the modifier, the claim denies. With it, the practice gets paid for care it legitimately provided. (Most billing managers don’t discover they’ve been leaving this revenue on the table until a coding audit surfaces the pattern.)
📌 Global Period Modifier Quick Reference: Modifier 24 — Unrelated E/M during global period | Modifier 25 — Significant, separate E/M same day as a procedure | Modifier 57 — Decision for surgery made at this visit (90-day global) | Modifier 78 — Return to OR for complication related to original surgery | Modifier 79 — Unrelated surgical procedure during global period
What Modifiers Are Required in Orthopedic Billing?
Modifier errors are one of the two leading drivers of orthopedic billing denials — right alongside ICD-10 unspecified codes. In orthopedics, modifiers aren’t optional documentation details. They’re code-level decisions that determine whether a claim pays the correct amount, pays a reduced amount, or doesn’t pay at all.
Modifier RT & LT — Laterality
Required on all unilateral orthopedic procedure codes. Without laterality on joint procedures, payers cannot distinguish bilateral from unilateral intent and may process at a reduced bilateral rate — or deny entirely pending clarification. Apply RT or LT on every claim — never omit laterality on orthopedic surgical codes.
Modifier 50 — Bilateral Procedure
Use when the identical procedure is performed on both sides in the same surgical session — bilateral knee replacements performed simultaneously, for example. Modifier 50 triggers bilateral pricing rules: typically 150% of the single-side fee schedule amount. Payer policies vary — some accept Modifier 50 on a single line; others require two lines with LT and RT.
Modifier 59 — Distinct Procedural Service
Applied when two procedures performed would normally be bundled by CCI edits, but are legitimately distinct based on different anatomical sites, sessions, or circumstances. For arthroscopic knee cases, Modifier 59 often separates chondroplasty (29877) from meniscectomy (29881) when performed on distinct compartments in the same session.
Modifier 51 — Multiple Procedures (Add-On Code Warning)
Indicates multiple procedures in the same session. Critical rule: never apply Modifier 51 to add-on codes. Add-on codes already embed the multiple procedure relationship. Applying Modifier 51 to add-on codes in spinal surgery creates an inappropriate additional payment reduction that compounds across hundreds of cases per year in high-volume spine practices — silently, as reduced payment rather than denial.
Modifiers 78 & 79 — Return to OR
Modifier 78: return to OR for a complication related to the original procedure during the global period. Modifier 79: an unrelated surgical procedure during the global period. Both allow separate reimbursement during the global window. Confusing or omitting these modifiers converts legitimately billable surgical care into unbilled OR time.
How Has the 2026 Prior Authorization Landscape Changed Orthopedic Billing?
Prior authorization has always been burdensome in orthopedics. In 2026, it’s genuinely harder — not because payers added more procedures to the auth list (though they did), but because the speed and automation of the review process changed the stakes of an incomplete submission.
CMS-0057-F: Faster Decisions, Less Room for Incomplete Documentation
The CMS Interoperability and Prior Authorization Final Rule (CMS-0057-F), effective January 1, 2026, requires Medicare Advantage, Medicaid managed care, CHIP, and QHP payers to render standard prior authorization decisions within 7 calendar days and urgent decisions within 72 hours. Faster decisions with incomplete documentation means faster denials. When a total joint authorization request arrives missing three to six months of documented conservative treatment failure, the AI review system flags it and rejects it within hours — not within the 14 days practices previously had to notice the gap and supplement the submission.
AI-Driven Pre-Authorization Review
Payer AI review systems now screen authorization requests against clinical criteria databases automatically before a human reviewer becomes involved. Incomplete submissions get rejected faster than ever. But under CMS-0057-F, payers must now provide a specific denial reason for every rejected authorization — and that specific reason is actually useful. You know exactly what documentation gap triggered the rejection, which means targeted appeals are more efficient than the generic “appeal everything” approach most practices have been using.
WISeR — The Orthopedic-Relevant Medicare Prior Auth Program
CMS’s WISeR (Warranted Interventional Significant and Elective Requested) program currently covers approximately 17 service categories with direct orthopedic implications — including epidural steroid injections, knee arthroscopy for osteoarthritis, cervical fusion, percutaneous vertebral augmentation, and nerve stimulator implants. If your practice performs any of these in the Original Medicare population, WISeR adds a separate prior authorization requirement layer. Notably, there’s no limit on the number of WISeR resubmissions — which means a rejected request isn’t a dead end, it’s a documentation revision task.
⚠ Authorization Number Must Match the Billed CPT Code: One of the most expensive auth-related denial scenarios occurs when an intraoperative decision changes the procedure. Authorization was granted for CPT 27446 (partial knee replacement), but the surgeon determined intraoperatively that a total replacement (27447) was needed. The authorization covers only 27446 — and the claim for 27447 will deny without a retro-auth or separate authorization. Build a protocol for retro-authorization requests before the patient leaves the facility.
What Are the Top Orthopedic Billing Denial Causes in 2026?
Why do orthopedic ASC practices see 14–22% denial rates when best-in-class is under 4%?
The gap between a 4% denial rate and a 20% denial rate in orthopedics almost always traces to three systemic failures: unspecified ICD-10 coding, incomplete authorization documentation, and modifier protocol gaps. These aren’t exotic billing problems — they’re common, preventable, and they cluster around specific high-volume procedure types that orthopedic billing teams touch every single day (Medical Billers and Coders, 2026).
- Unspecified ICD-10 Codes — The Single Biggest Orthopedic Revenue Leak. Payers now enforce ICD-10 coding to the 7th character level for surgical orthopedic claims. Submitting M17.9 (knee OA, unspecified) instead of M17.11 (primary OA, right knee) for a TKA claim triggers immediate medical necessity review — or outright rejection in Medicare Advantage plans. Build ICD-10 cheat sheets by body region and make specificity checking a pre-submission step, not an afterthought.
- Missing or Insufficient Conservative Treatment Documentation for Joint Replacement. Most commercial payers and Medicare Advantage plans require documentation of three to six months of conservative treatment failure before authorizing total joint replacement. The documentation must be specific: which treatments were attempted, the duration and frequency of each, objective evidence of ongoing functional limitation despite treatment, and the clinical findings supporting the surgical decision. “Patient has tried conservative care” consistently fails — dated, modality-specific documentation passes.
- Modifier 51 Applied to Add-On Codes in Spinal Surgery. For high-volume spine practices billing multiple add-on codes per multi-level fusion case, this error compounded across a year of claims represents sustained annual underpayment that never shows up as a denial — it shows up as systematically lower reimbursement that nobody questions. The only way to catch it is a quarterly coding audit comparing expected reimbursement against actual payments for add-on codes.
- Global Period Violations — Billing Included Services Without Modifiers. Billing E/M visits, minor procedures, or post-op care included in the 90-day global package without the correct modifier generates automatic denials. The reverse problem — not billing legitimately separate services with Modifier 24 — creates invisible revenue loss. Both directions are systematic and preventable with a global period tracking protocol embedded in the scheduling and billing workflow.
- Authorization Expired Before Service or Wrong CPT Code Authorized. Authorization approvals have date windows — and orthopedic procedures get delayed regularly due to patient health issues, scheduling conflicts, and facility availability. Track authorization expiration dates alongside case scheduling and flag conflicts before they become denial scenarios. If the procedure changes between auth submission and the OR date, initiate retro-auth before the case proceeds.
- Arthroscopic Multi-Procedure CCI Edit Bundling Errors. Knee arthroscopy cases billing meniscectomy (29881), chondroplasty (29877), and debridement (29879) in the same session require CCI edit analysis to determine which combinations are bundled and which require Modifier 59 for separate reimbursement. A billing team without current knowledge of these edit pairs will consistently underbill multi-intervention knee arthroscopy cases — and won’t know it until a retrospective audit.
How do you document orthopedic procedures to survive a payer audit in 2026?
The operative note is not just a clinical record of what happened in the OR. In 2026, it’s the primary evidence document that supports payment — and payer AI systems are reading it with specific criteria checklists, not clinical judgment.
For total joint replacement, your operative note must document: the specific implant manufacturer, model, and component sizes used; the approach technique and any deviations; intraoperative findings including the condition of joint surfaces, presence and extent of cartilage damage, and bone quality; and the rationale for the specific implant design selected. “TKA performed without complications” doesn’t pass a post-payment audit. “Tricompartmental OA confirmed on arthrotomy with full-thickness cartilage loss on medial and patellofemoral surfaces, cruciate-retaining implant selected based on intact PCL” does.
For arthroscopic procedures, document the compartments visualized, the specific findings in each compartment, the procedures performed in each compartment (not just the billed code), and any decision-making that occurred intraoperatively — particularly decisions that change the billing from what was originally planned. When Modifier 59 is applied, the operative note must describe why the procedures were distinct — different compartments, different structures, different anatomical sites. The modifier alone doesn’t justify the separate payment. The documentation behind it does.
In-House Orthopedic Billing vs. Specialized Outsourced Billing: What’s the Real Difference?
❌ In-House Billing (Typical Orthopedic ASC)
- Denial rate: 14–22% (vs. 11.8% industry average)
- Prior auth: Case-by-case — gaps during staff absences
- Global period tracking: Often informal — modifier errors common
- ICD-10 specificity: Unspecified codes used frequently under time pressure
- Spinal add-on compliance: Modifier 51 applied — silent underpayment
- 2026 CPT compliance: Charge master updates often delayed until February
- Annual revenue at stake (per $700K practice): ~$210,000 in delayed or lost revenue
- AR days: 55–75 days (typical orthopedic practice)
✅ Qualigenix Specialized Orthopedic Billing
- Denial rate: Under 5% — specialty-specific modifier and ICD-10 protocols
- Prior auth: Systematic workflow by procedure type and payer with expiration tracking
- Global period tracking: Calendared per patient with modifier protocol embedded
- ICD-10 specificity: Laterality and 7th character verified as pre-submission step
- Spinal add-on compliance: Add-on protocol prevents Modifier 51; quarterly audits catch underpayments
- 2026 CPT compliance: Annual charge master audit completed before January 1 every year
- Annual revenue at stake (per $700K practice): ~$20,000 at under 4% denial rate
- AR days: 36-day average collection cycle — 30% reduction from baseline
How Does Qualigenix Maximize Revenue for Orthopedic Practices?
Orthopedic billing requires specialty expertise that general billing companies don’t have. The difference between Modifier 51 applied to an add-on code and Modifier 51 applied to a primary code isn’t a detail you learn from a general billing manual. The three-to-six months of documented conservative treatment failure that separates an authorized total joint replacement from a denied one isn’t information a generalist coder recognizes as a red flag. These orthopedic-specific knowledge gaps drive the 14–22% denial rates typical orthopedic ASCs experience — and they’re exactly what Qualigenix’s specialty training is designed to close.
Orthopedic-Trained Coders, Not Generalists
Qualigenix’s orthopedic billing services use CPC-certified coders who work orthopedic accounts exclusively — reading operative notes fluently, applying the full laterality modifier set correctly on every surgical claim, and verifying 2026 CPT compliance before a claim leaves the system. The charge master update that most practices delay until February — catching its first wave of denials from deleted codes — is completed by Qualigenix before January 1 every year. No deleted codes. No outdated add-on structures. No preventable rejections from codes that stopped being valid three months ago.
Prior Authorization Management Built Into the Workflow
For orthopedic practices, prior authorization isn’t a billing function — it’s a scheduling function that billing has to manage. Qualigenix’s prior authorization solutions track authorization requirements by payer and procedure type, manage submission and follow-up, monitor authorization expiration dates against the surgical schedule, and flag mismatches before the case goes to the OR. The authorization number that doesn’t match the billed CPT code — the scenario that generates one of orthopedic’s most frustrating hard denials — gets caught before the patient is prepped, not when the EOB arrives six weeks later.
Denial Root-Cause Analysis That Fixes the Process, Not Just the Claim
When denials do occur, Qualigenix’s denial management workflow goes beyond resubmission. Every denied claim is categorized by root cause — unspecified ICD-10, modifier error, global period violation, auth mismatch, or documentation gap. Pattern analysis across 30-day rolling windows surfaces systematic issues. A recurring medical necessity denial on lumbar fusion cases triggers a documentation template review, not just a case-by-case appeal. A pattern of Modifier 59 rejections on arthroscopic multi-procedure claims triggers a CCI edit audit. The goal isn’t to win individual appeals — it’s to eliminate the conditions that generate the same denial month after month. That’s the process that produces 95% first-pass acceptance sustainably.
For practices affiliated with TEAM Model hospitals — 741 acute care hospitals now bearing 30-day post-discharge financial accountability for orthopedic episodes — the revenue stakes extend beyond individual claim accuracy. Qualigenix’s integrated billing and AR management ensures the billing side of the orthopedic episode is precisely managed while the clinical team focuses on care quality that protects both the patient outcome and the hospital’s episode financial accountability. The downstream result is a stable revenue cycle that doesn’t depend on any single administrative step going right. It’s built to go right systematically.
Orthopedic Billing Compliance Checklist: 10 Steps for 2026
- ☐ Audit your charge master against 2026 CPT changes before Q2: Verify that updated spinal fusion add-on code rules, revised arthroplasty revision definitions, and clarified fracture care documentation requirements are reflected in your charge master. If not done since December 2025, it’s overdue.
- ☐ Replace all unspecified ICD-10 codes with laterality-specific codes: Build body-region-specific ICD-10 cheat sheets and eliminate M17.9, M16.9, and similar unspecified codes from orthopedic billing templates. In 2026, unspecified OA codes are among the most consistently denied ICD-10 choices in joint replacement billing.
- ☐ Enforce the 7th character requirement on all injury diagnoses: Create EHR prompts or billing workflow checkpoints that confirm the correct 7th character (A, D, or S) before claim submission on all fracture and injury codes. This single check prevents a high-frequency denial category.
- ☐ Build a modifier protocol — especially the add-on code Modifier 51 prohibition: Document explicitly in your billing protocol that Modifier 51 is never applied to add-on codes. Conduct a retrospective audit of the past 12 months of spinal surgery claims to quantify underpayment from this error.
- ☐ Track global period start dates in the scheduling system: Every surgical patient’s 90-day global period should be calendared at the time of surgery. Flag all follow-up visits during the window for modifier review — Modifier 24 for unrelated conditions, Modifier 79 for unrelated procedures.
- ☐ Obtain prior authorization before scheduling — not at check-in: Build authorization confirmation into the scheduling workflow as a non-negotiable prerequisite for surgical booking. Authorization status, expiration date, and authorized CPT code should appear in the scheduling system alongside the booked procedure.
- ☐ Verify authorization CPT code matches intended procedure at pre-op: Add a pre-operative verification step confirming the authorized CPT code matches the planned procedure. If there’s a mismatch — due to an updated plan, a surgeon preference change, or a clinical decision — initiate retro-auth immediately.
- ☐ Document conservative treatment failure with specificity before authorizing joint replacement: Pre-surgical notes must include treatment types, dates started and ended, frequency, and objective evidence of ongoing functional limitation. “Patient tried PT” doesn’t support authorization; dated, specific, modality-specific documentation does.
- ☐ Run CCI edit validation on all multi-procedure arthroscopy claims before submission: Enable payer-specific CCI edit checks in your clearinghouse before submission — not after the denial arrives. Knee arthroscopy cases billing meniscectomy plus additional interventions require CCI edit analysis before every claim.
- ☐ Conduct quarterly coding audits on highest-volume CPT codes: Review joint replacement, spinal fusion, and high-volume arthroscopy claims every quarter for modifier accuracy, ICD-10 specificity, global period compliance, and authorization match. The orthopedic denial patterns that cost the most money are systematic, not random — and quarterly audits catch them before they compound.
Frequently Asked Questions About Orthopedic Billing
What is orthopedic billing?
Orthopedic billing is the process of translating musculoskeletal clinical encounters — joint replacements, spinal surgeries, arthroscopy, fracture care, and office visits — into accurate insurance claims using CPT codes, ICD-10 diagnosis codes with full laterality, and specialty modifiers. It’s one of healthcare’s most complex billing environments because it requires managing the 90-day global surgical package, multi-code spinal procedures, high prior authorization burdens, and strict documentation requirements that payer AI systems now evaluate automatically.
The financial stakes in orthopedic billing are unusually high per claim. A total knee arthroplasty represents $11,400 or more in at-risk revenue on a single CPT code. Even a low denial rate in absolute percentage terms translates to substantial dollar amounts when the average claim value is this high.
What is the 90-day global surgical package in orthopedic billing?
The 90-day global surgical package bundles the pre-operative evaluation one day before surgery, the procedure itself, and all routine post-operative care within 90 days into a single global reimbursement. Billing any service included in the global package separately — without the correct modifier — generates an automatic denial. Modifiers 78 and 79 allow separate billing for return to OR, while Modifier 24 covers unrelated E/M visits during the global window.
The global period also creates a less-discussed revenue problem: practices that don’t use Modifier 24 when they should are losing reimbursement for legitimate, separately billable care. An unrelated condition evaluated during a post-op visit is billable with Modifier 24 — but only if someone applies the modifier. Without it, the claim denies and the visit goes uncompensated.
What ICD-10 codes should orthopedic practices avoid?
Orthopedic practices should avoid all unspecified codes when the clinical record supports specificity. Most consequentially: avoid M17.9 (knee OA, unspecified) — use M17.11 (right) or M17.12 (left) instead. Avoid M16.9 (hip OA, unspecified) — use M16.11 or M16.12. Avoid all injury codes without the required 7th character (A, D, or S). Unspecified codes trigger immediate medical necessity review or outright rejection in 2026.
Additionally, avoid using pain codes (M54.5 for low back pain, M25.561 for knee pain) as primary diagnoses for surgical procedures when a structural diagnosis is available and documented. Pain codes as primary diagnoses for joint replacement or spinal fusion claims generate medical necessity denials because they don’t establish the pathological basis for surgery.
How did 2026 change prior authorization for orthopedic procedures?
CMS-0057-F, effective January 1, 2026, shortened standard prior authorization decisions to 7 calendar days and urgent decisions to 72 hours. Payers must now provide specific denial reasons for every rejected authorization. AI review systems screen documentation gaps automatically before human review. 92% of orthopedic ASC claims require pre-authorization, and Medicare Advantage denied 7.4% of orthopedic prior auth requests in 2025.
The practical implication: prior authorization submissions need to be complete on first submission more than ever. The strategy of submitting and then supplementing when the payer asks questions no longer works when AI review generates a rejection in hours. Documentation completeness is now a submission prerequisite, not a follow-up task.
What modifiers are most commonly misused in orthopedic billing?
The most costly orthopedic modifier errors are: applying Modifier 51 to add-on codes in spinal surgery (generates sustained underpayment across hundreds of cases); omitting RT or LT laterality modifiers on unilateral procedures; failing to use Modifier 24 for unrelated E/M visits during the global period; and applying Modifier 59 to code combinations that are not actually distinct per CCI edits.
Modifier 51 on add-on codes is dangerous specifically because it doesn’t generate an outright denial — it generates reduced payment. Practices can go months without noticing because the claim pays, just at a lower amount than contracted. A quarterly audit comparing expected versus actual reimbursement on add-on code claims is the only way to systematically catch this error.
What are the major 2026 CPT code changes for orthopedics?
The 2026 AMA CPT update introduced 418 total changes with musculoskeletal and spine coding among the most affected. Key orthopedic changes: refined multi-level spinal fusion coding rules where add-on codes 22614 and 22632 are not interchangeable; updated arthroplasty revision definitions distinguishing complete from partial revision; and clarified fracture care documentation thresholds distinguishing closed treatment with and without manipulation.
Practices whose charge masters were not updated by January 1, 2026 are generating avoidable denials from deleted or revised codes. The charge master update is not a January problem — it’s a November and December problem that determines whether January billing starts clean or generates its first wave of preventable rejections.
How does Qualigenix help orthopedic practices reduce denials?
Qualigenix provides orthopedic billing with CPC-certified coders trained specifically in musculoskeletal and spinal surgery coding, 2026 CPT compliance workflows, global period tracking with modifier protocol enforcement, laterality-specific ICD-10 verification, prior authorization management with authorization-to-CPT matching, CCI edit validation before every submission, and monthly denial pattern analysis correcting workflow problems at their source. The result: 99% claim accuracy and 95% first-pass acceptance across all orthopedic procedure types.
The documentation feedback loop is particularly impactful for orthopedic practices where the operative note is the primary evidence document for both authorization and payment. When Qualigenix identifies that denial patterns trace to documentation gaps in conservative treatment failure or revision arthroplasty component specificity, structured queries go to the clinical team — improving documentation quality at the point of care, not after the denial arrives. Book a free consultation for an immediate orthopedic billing assessment and denial pattern analysis.
Related Qualigenix Resources
Specialty billing — 2026 CPT compliant, 99% claim accuracy
CPC-certified specialty coders across 38+ specialties
Root-cause analysis and systematic denial prevention
Authorization tracking with CPT-match verification
Clean orthopedic claims with NCCI edit validation
Recover unpaid orthopedic claims — nothing ages out unworked
Clean Claim Rate: Benchmarks & Best Practices
How to benchmark and improve orthopedic first-pass performance
What Are Claim Denials? Types, Causes & Fixes 2026
The systematic approach to denial prevention and recovery
Eligibility Verification Services
Stop coverage gaps before they reach the OR
Revenue Cycle Management Services
End-to-end RCM for orthopedic practices — billing through collections
Stop Leaving $190,000 on the Table Every Year
Orthopedic practices that operate at under 4% denial rates collect $190,000 more annually than those running at 10–15% — on identical procedure volume. Qualigenix’s orthopedic-trained billing team manages 2026 CPT compliance, prior authorization, global period tracking, modifier protocols, and denial root-cause analysis so your revenue reflects the care your surgeons actually deliver.
Our team delivers 99% claim accuracy, a 95% first-pass acceptance rate, an average 36-day collection cycle, and a 30% reduction in AR days. We onboard in as few as 6 days.
Precision. Progress. Qualigenix.
What’s Next

Denial Management in 2026: The Top 10 Codes and the Appeal Playbook for Each
Denials cluster around a small set of codes, and each one has a different correct response. Some need a...
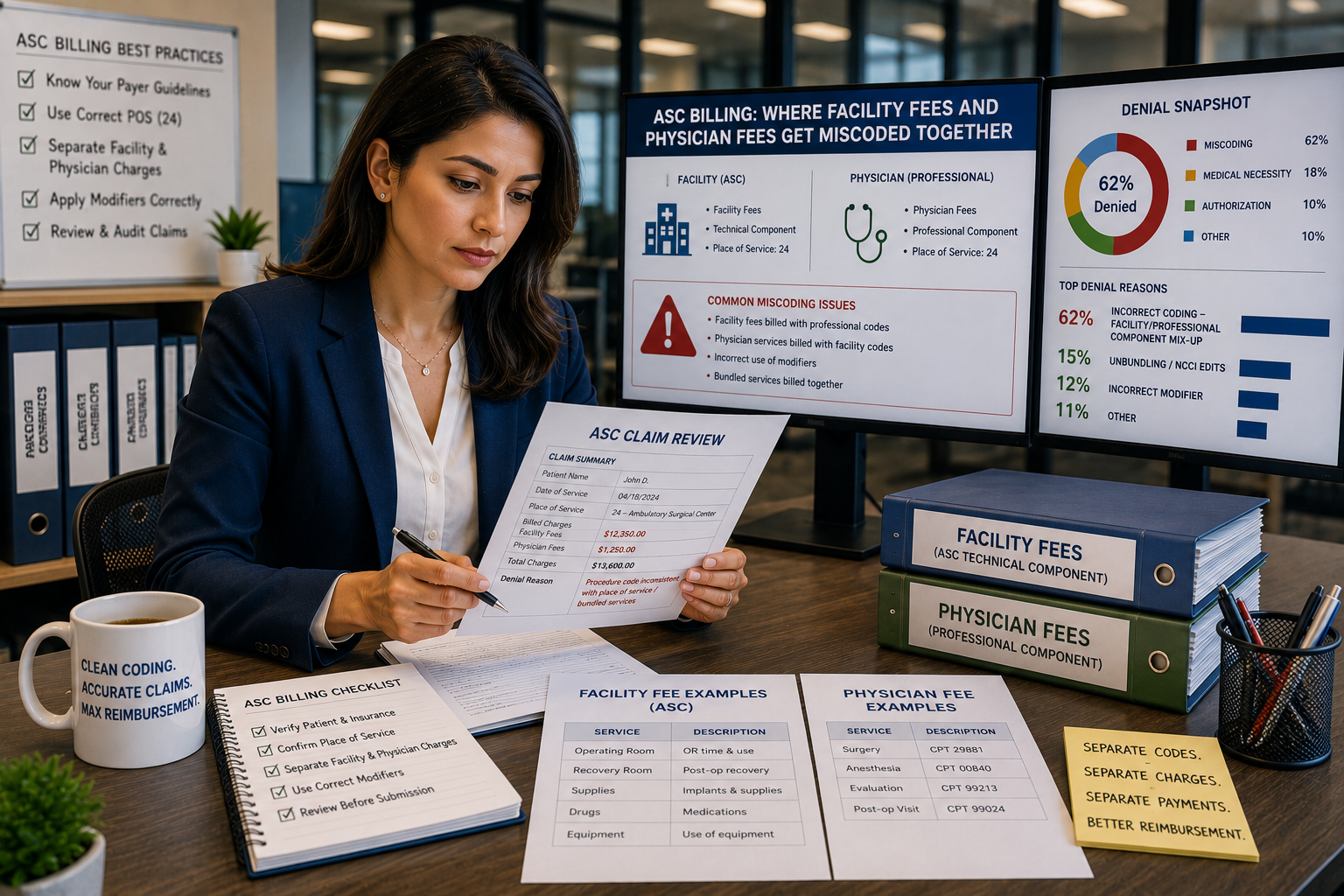
ASC Billing: Where Facility Fees and Physician Fees Get Miscoded Together
ASC facility and physician claims both go out on a CMS-1500 form with the same CPT code and place...
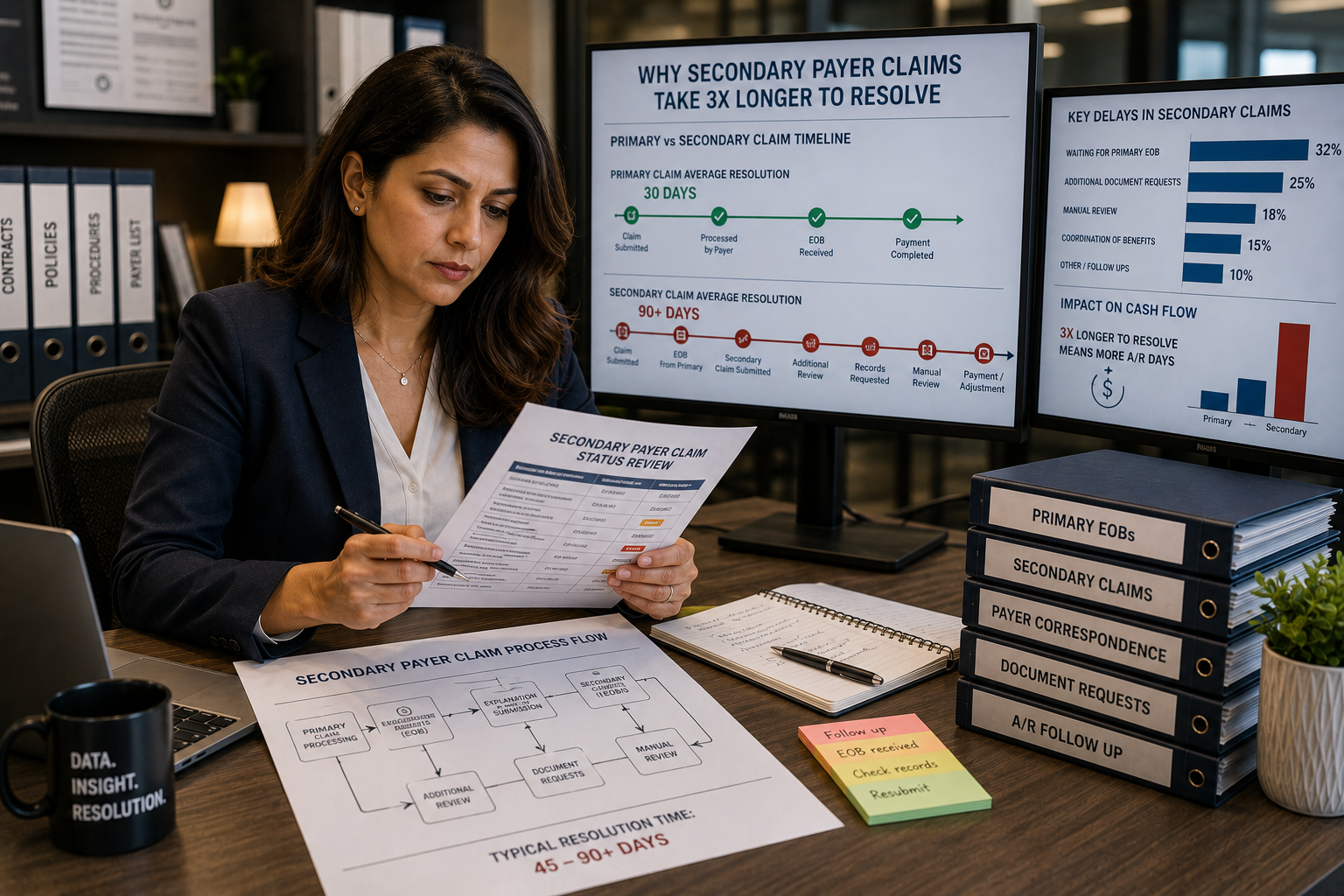
Coordination of benefits errors: why secondary payer claims take 3x longer to resolve
Secondary payer claims stall because coordination of benefits errors, wrong payer order, outdated COB records, and missing primary...