Dermatology Revenue Cycle Management: Complete Guide for Skin Care Practices 2026
The Qualigenix Editorial Team consists of certified billing and coding experts with over 40 years of experience across 38+ medical specialties. Our content is rigorously researched against CMS, AMA, and payer-specific guidelines to ensure total compliance and accuracy. We apply the same elite standards to our resources as we do our client work, consistently delivering high claim accuracy and significant reductions in AR days.

Dermatology billing is among the most technically demanding in outpatient medicine. A single patient visit can produce an E&M service, a biopsy, a shave removal, and a lesion excision — all on the same claim, each with its own CPT code, modifier requirements, and medical necessity standards. Get any one of them wrong and you face a denial, an audit flag, or lost revenue. Add biologic prior authorization battles, Mohs surgery stage-based coding, cosmetic vs. medical necessity documentation requirements, and annual CPT revisions — and you have a billing environment where errors are predictable, frequent, and expensive. This guide covers every major dermatology billing category — lesion coding, modifier rules, Mohs, biologics, denial management, and more — with the workflows that help Qualigenix clients achieve a 99% claim accuracy rate, 95% first-pass acceptance, and a 30% reduction in AR days.
Dermatology practices face a billing paradox. The procedures are often brief. The coding complexity is anything but.
A shave removal that takes five minutes in the exam room requires the biller to know the lesion diameter, the anatomical location category, whether an E&M service qualifies for Modifier 25, whether a same-day biopsy creates a bundling issue, and whether the ICD-10 code documents medical necessity or inadvertently signals a cosmetic indication. Miss any one of those and the claim denies or pays at reduced rate.
In a busy dermatology practice seeing 40 to 60 patients per day, billing errors are not isolated incidents. They are systematic revenue leaks that compound daily, month after month, until AR aging expands and collections fall short of the care delivered.
This guide gives dermatology practices the complete picture of revenue cycle management in 2026 — where the billing complexity lives, where practices consistently lose revenue, and what a high-performing dermatology RCM process looks like end to end.
Dermatology revenue cycle management is the specialized billing and collections process for skin care practices. It covers lesion excision and destruction coding by size and location, biopsy CPT selection by technique, modifier rules for same-day E&M and procedure encounters, cosmetic vs. medically necessary service documentation, prior authorization for biologics and Mohs surgery, and dermatology-specific denial management — all in a specialty where a single patient visit commonly generates three to five simultaneous procedure and service codes, each with its own billing requirements.
Why Dermatology Billing Is Different From Every Other Specialty
Ask a dermatology biller what makes this specialty uniquely difficult, and the answer is the same across every practice: the volume and simultaneity of procedures. In family medicine, a visit generates one E&M code. In dermatology, one visit can generate an E&M, two biopsies, a shave removal, and a lesion destruction — all on the same claim, all subject to their own coding rules, all subject to NCCI bundling edits that determine which can be paid together and which require modifiers.
Three factors make dermatology billing structurally different from most outpatient specialties.
The Multi-Procedure Problem
Dermatology is one of the few outpatient specialties where multi-procedure encounters are the routine, not the exception. Patients regularly present with multiple concurrent skin conditions. Dermatologists diagnose and treat several in a single visit. The result is a claim that requires careful modifier application, NCCI edit awareness, and medical necessity documentation for every service — not just the primary one.
The hierarchy of procedures, the correct modifier for each service in the context of the others, and which combinations payers will bundle vs. pay separately — this is knowledge that takes years to build and months to lose when staff turns over.
The Cosmetic-Medical Boundary
Dermatology sits at the intersection of covered medical services and non-covered cosmetic procedures more than any other specialty. Many dermatology services exist in both worlds simultaneously — acne treatment is medical; laser resurfacing for scarring can be medical or cosmetic depending on the indication and documentation. Sebaceous cyst removal is medical when symptomatic; cosmetic when performed for appearance only.
This boundary is drawn entirely by documentation. The diagnosis code, the clinical note language, and the documented medical necessity determine whether a payer covers the service or denies it as cosmetic. Practices with inconsistent documentation standards create inconsistent billing outcomes — and inconsistent revenue.
Annual Coding Changes With High Specificity Requirements
Dermatology CPT codes change meaningfully every year. The 2019 biopsy code revisions — which replaced three codes with a technique-based system of seven — caught many practices still using outdated codes years later. Lesion excision codes require measurement specificity down to the millimeter. Destruction codes cascade based on the number of lesions, not the size. Any year’s updates can affect the most frequently billed codes in the practice.
What makes dermatology billing more complex than other outpatient specialties?
Three factors: a single patient visit routinely generates three to five simultaneous procedure codes, each with its own coding rules and modifier requirements; many dermatology services exist at the cosmetic-medical boundary and are covered or denied based entirely on clinical documentation; and dermatology CPT codes require high-specificity measurements — lesion diameter in centimeters, anatomical location category, number of lesions, biopsy technique — that must be documented precisely in the clinical note to support the selected code.
Dermatology Revenue Cycle Benchmarks
| Metric | Typical Dermatology Practice | Best Practice Target | Qualigenix |
|---|---|---|---|
| Denial Rate | 8–15% | Under 5% | <5% |
| Clean Claim Rate | 72–82% | 95%+ | 95% |
| Days in AR | 45–65 days | 30–38 days | 36 days avg. |
| Modifier 25/59 Denial Share | 25–35% of all denials | Near zero with pre-claim review | Modifier review on every claim |
| Biologic Auth Denial Share | 20–30% of biologic claims | Near zero with tracking system | Systematic auth management |
| Lesion Excision Coding Error Rate | Est. 12–18% of procedure claims | Under 1% with pre-billing review | Measurement verification included |
| Cosmetic vs. Medical Denial Rate | Top 3 denial cause in dermatology | Eliminated with documentation standards | ICD-10 and note audit built-in |
| Biopsy Coding Error Rate | High — 2019 revision still causing errors | Zero with current code knowledge | Updated biopsy coding library |
| States with Step Therapy Exemption Laws | 30+ states as of 2026 | Know and cite applicable state law | State law tracking included |
| Claim Accuracy Rate | 72–84% | 95%+ | 99% |
| AR Days Reduction Post-Outsourcing | — | 20–30% | 30% within first quarter |
| Onboarding Time | 2–4 weeks (typical vendor) | Under 2 weeks | As few as 6 days |
Sources: AAD Practice Profile Survey 2025; MGMA Medical Practice Excellence Report 2025; CMS Dermatology Billing Guidelines 2026; Qualigenix internal performance data 2026.
Lesion Removal Coding: The Financial Engine of Dermatology RCM
Lesion removal is the most frequently billed procedure category in most dermatology practices — and the category with the highest coding error rate. The errors are systematic and predictable: wrong size category, wrong location category, wrong procedure type, or all three.
The Three Procedure Types
Dermatology lesion removal divides into three fundamentally different CPT families, each with its own coding logic.
Shave removal (11300–11313) is used when the lesion is removed by horizontal shaving — not by a full-thickness incision with suture closure. The shaved layer does not penetrate below the dermis. Shave removal codes are selected based on lesion diameter and anatomical location.
Excision of benign lesions (11400–11471) covers full-thickness removal through the dermis of benign lesions with sutured or non-sutured closure. The critical measurement is the excised diameter — not just the lesion diameter. Excised diameter equals the widest lesion measurement plus the narrowest margin on each side. Location category (trunk/extremities vs. face/ears/eyelids/nose/lips) then determines which code in the range applies.
Excision of malignant lesions (11600–11646) follows the same excised-diameter logic as benign excision but uses a separate CPT range with higher relative value units. A histologic diagnosis of malignancy — confirmed by pathology — is required to justify this code series. Billing malignant excision codes without pathology documentation of malignancy is a compliance violation.
The Excised Diameter Rule
The most common lesion excision coding error in dermatology is using the lesion diameter rather than the excised diameter to select the CPT code. These are not the same number — and the difference determines which code applies.
Excised diameter = widest lesion dimension + narrowest surgical margin on each side of the specimen.
Example: A 1.2cm basal cell carcinoma on the cheek is excised with 0.3cm margins on all sides. The excised diameter is 1.2 + 0.3 + 0.3 = 1.8cm. The correct malignant excision code for face, 1.1 to 2.0cm excised diameter is CPT 11642. If the biller codes from the lesion diameter alone (1.2cm), they select a lower code — underbilling by one or two code levels. In a practice performing 20 excisions per week, systematic underbilling of this type produces significant annual revenue loss.
Warning — Excised Diameter Documentation: The excised diameter must be explicitly documented in the operative note. Billing reviewers and auditors look for this measurement. If the note documents lesion size only — and the claim uses an excision code implying a larger excised diameter — you have a documentation-code mismatch that generates audit risk. Train clinicians to document: (1) lesion diameter at widest dimension, (2) surgical margins in centimeters on each side, and (3) the calculated excised diameter in the procedure note body. This single documentation habit prevents the most common lesion excision audit trigger in dermatology.
Commonly Billed Dermatology Lesion Removal CPT Codes
| CPT Range | Procedure Type | Code Selection Factor | Key Billing Rule |
|---|---|---|---|
| 11300–11305 | Shave removal — trunk, arms, legs | Lesion diameter | Horizontal shaving technique; no full-thickness incision |
| 11306–11313 | Shave removal — scalp, neck, face, ears | Lesion diameter | Higher-value location category; document site clearly |
| 11400–11406 | Excision, benign — trunk, arms, legs | Excised diameter | Full thickness; suture closure common but not required |
| 11420–11426 | Excision, benign — scalp, neck, hands, feet, genitalia | Excised diameter | Mid-range location category; higher RVU than trunk |
| 11440–11446 | Excision, benign — face, ears, eyelids, nose, lips | Excised diameter | Highest location category for benign excision |
| 11600–11606 | Excision, malignant — trunk, arms, legs | Excised diameter | Requires histologic malignancy diagnosis to justify |
| 11620–11626 | Excision, malignant — scalp, neck, hands, feet, genitalia | Excised diameter | Higher RVU than trunk; same malignancy documentation requirement |
| 11640–11646 | Excision, malignant — face, ears, eyelids, nose, lips | Excised diameter | Highest RVU malignant excision series; face location |
| 17000 | Destruction, benign/premalignant — first lesion | Number of lesions | Actinic keratoses, warts, seborrheic keratoses |
| 17003 | Destruction — each additional lesion (2nd–14th) | Number of lesions | Add-on to 17000; list total number of additional lesions |
| 17004 | Destruction — 15 or more lesions | Total lesion count ≥15 | Stand-alone code when 15+ lesions destroyed; do not use with 17000/17003 |
| 11102–11107 | Skin biopsy (2019 revised codes) | Technique (tangential, punch, incisional) + additional specimens | Primary code for first specimen; add-on code for each additional specimen |
| 17311–17315 | Mohs surgery | Anatomical location + number of stages | Surgeon is also the pathologist; path interpretation built into code |
Biopsy Coding: The 2019 Revision Still Catching Practices Off Guard
The 2019 skin biopsy CPT code revision was one of the most significant dermatology coding changes in the past decade. It replaced the previous system with a technique-based approach that changed how the primary code is selected — and many practices are still using incorrect code logic years later.
The New Biopsy Code Structure
The revised biopsy codes (11102–11107) are organized by technique, not by body location. The technique determines the primary code, and additional specimens at the same encounter use technique-specific add-on codes.
Tangential biopsy (11102, primary; 11103, each additional): removal of a tissue sample using a blade oriented tangentially — shave biopsy, saucerization, or similar technique. This is the most commonly performed biopsy technique in dermatology.
Punch biopsy (11104, primary; 11105, each additional): full-thickness skin sampling using a punch instrument. Common for inflammatory conditions, suspected melanoma, and deeper pathology evaluation.
Incisional biopsy (11106, primary; 11107, each additional): sharp incision into the skin for tissue sampling requiring direct visualization. Less frequent than tangential or punch biopsies but carries a higher RVU.
When multiple biopsies are performed at the same encounter using different techniques — for example, one punch biopsy and two tangential biopsies — bill the highest-value technique as the primary code and the others as add-on codes for their respective techniques. This hierarchy rule is frequently misapplied by practices still thinking in terms of the old single-code system.
How do I code a same-day punch biopsy and tangential biopsy in dermatology?
When two different biopsy techniques are used in the same encounter, bill the primary code for the highest-value technique first — punch biopsy (11104) has a higher RVU than tangential biopsy (11102) — then use the add-on code for the additional specimen of the other technique (11103 for the tangential biopsy). Do not bill two primary codes. The claim should show 11104 × 1 and 11103 × 1. Both require separate operative notes documenting the distinct lesion, technique, and location for each specimen submitted.
Modifier Rules in Dermatology: The Most Frequent Source of Denials
Modifier misuse — particularly Modifiers 25, 51, and 59 — generates more dermatology claim denials than any other single billing error category. Understanding when each modifier applies, when it does not, and what documentation supports its use is essential for any dermatology billing team.
Modifier 25: The Same-Day E&M and Procedure Rule
Modifier 25 is appended to the E&M code when a dermatologist provides a significant, separately identifiable evaluation and management service on the same day as a procedure.
The key phrase is “separately identifiable.” The E&M service must address a clinical problem that is distinct from the procedure performed. The clinical note for the E&M must document the evaluation — history, examination, medical decision-making — for a condition that stands independently of the procedure.
Modifier 25 is appropriate when: A patient comes in for a scheduled shave removal and also presents a new rash that the dermatologist evaluates, diagnoses, and initiates treatment for. The rash evaluation is a separate problem from the shave removal. The E&M code with Modifier 25 is correct.
Modifier 25 is NOT appropriate when: A patient comes in for a scheduled excision biopsy and the dermatologist performs the standard pre-procedure assessment. That assessment is part of the procedure service — it is not a separately identifiable E&M. Billing an E&M with Modifier 25 on top of the procedure in this scenario is incorrect and creates audit risk.
Audit Warning — Modifier 25 Overuse: CMS and commercial payers flag dermatology practices that bill Modifier 25 with high frequency relative to specialty benchmarks. If your practice is billing an E&M with Modifier 25 on more than 30–40% of procedure encounters, you may be at elevated audit risk. Appropriate use requires a distinct clinical problem, a separately documented E&M service in the clinical note, and a separate diagnosis code for the condition evaluated. Routine addition of Modifier 25 without this documentation is a compliance violation.
Modifier 59: Distinct Procedural Service
Modifier 59 is used to bypass an NCCI edit when two procedures performed together would normally be bundled — because the two services represent distinct and separate procedures not ordinarily performed together.
In dermatology, Modifier 59 most commonly appears when a biopsy and a procedure (shave removal or excision) are performed at different sites on the same day, or when two procedures that are ordinarily bundled under NCCI rules are clinically distinct in this patient’s case.
The documentation requirement for Modifier 59 is strict: the clinical note must clearly document why the two services are distinct — different anatomical sites, different sessions, different diagnoses, or different specimens. Appending Modifier 59 without corresponding documentation is the most common Modifier 59 compliance error in dermatology — and one payers actively audit.
Modifier 51: Multiple Procedures
Modifier 51 signals that a secondary procedure is subject to the multiple procedure payment reduction rule — where payers reimburse the primary procedure at 100% and secondary procedures at reduced rates (typically 50% for Medicare). Modifier 51 is applied to secondary procedures in the same operative session when no NCCI edit makes them bundled.
Modifier 51 is not a discretionary choice — it is applied based on which procedure carries the highest RVU. The primary procedure receives no modifier. Secondary procedures receive Modifier 51. Add-on codes (designated with a + symbol in the CPT book) are exempt from Modifier 51 and should never receive it.
What is the difference between Modifier 25, 51, and 59 in dermatology?
Modifier 25 goes on the E&M code — it tells the payer the E&M is a distinct service from the procedure. Modifier 51 goes on secondary procedure codes — it tells the payer this is a multiple-procedure encounter subject to payment reduction rules. Modifier 59 goes on a procedure code to override an NCCI bundling edit — it tells the payer the two services are distinct and separately payable despite what the NCCI edit table says. Each requires different documentation and applies to a different type of claim.
Mohs Surgery Billing: Stage-Based Coding and the Pathologist Role
Mohs micrographic surgery is one of the most precise — and most valuable — procedures in dermatology billing. It is also one of the most misunderstood from a coding standpoint. Getting Mohs billing right requires understanding both the stage-based coding structure and the unique role the Mohs surgeon plays as simultaneous surgeon and pathologist.
How Mohs Billing Works
Mohs surgery is billed per stage — each stage representing one layer of tissue excised and examined microscopically by the surgeon before the next stage is performed. The codes divide by anatomical location and by whether the stage is the first or subsequent at the same site.
CPT 17311 — First stage on the head, neck, hands, feet, genitalia, or any location involving muscle, cartilage, bone, tendon, or major nerves. This is the highest RVU Mohs code — reserved for high-complexity anatomical sites.
CPT 17312 — Each additional stage at the same site as 17311 (add-on).
CPT 17313 — First stage on the trunk, arms, or legs — lower-complexity locations.
CPT 17314 — Each additional stage at the same site as 17313 (add-on).
If Mohs surgery is performed at two separate anatomical sites on the same day — for example, a BCC on the nose and a BCC on the trunk — bill the first stage separately for each site. The nose uses 17311; the trunk uses 17313.
The Pathology Rule in Mohs Billing
The defining characteristic of Mohs surgery billing is that the surgeon interprets the frozen sections. The Mohs codes are comprehensive — they include the surgical excision, specimen processing, histopathologic examination, and microscopic interpretation by the surgeon. No separate pathology code should be billed alongside Mohs codes when the Mohs surgeon is performing the path interpretation.
Billing a separate 88304 or 88305 pathology code alongside Mohs codes when the surgeon is doing the path is unbundling — it will be denied and flagged for audit. If an independent pathologist separately processes and interprets non-Mohs specimens from the same encounter, a separate pathology code for that specimen may be appropriate — but not for the Mohs-controlled sections.
Prior Auth Tip — Mohs Surgery: While Medicare does not require prior authorization for Mohs surgery, many commercial payers and Medicare Advantage plans do. Before every Mohs procedure, verify payer-specific prior authorization requirements. For payers that require auth, submit the request with: pathology confirming skin cancer diagnosis, lesion location, and clinical rationale for Mohs vs. wide local excision (typically high-risk site or complex anatomy). The medical necessity for Mohs is well-established for high-risk sites — documented clearly, prior auth approvals are routine.
Biologic Billing and Prior Authorization: The Highest-Dollar Denial Category
The emergence of biologic medications for psoriasis, atopic dermatitis, and hidradenitis suppurativa has created a new high-stakes billing category in dermatology. A single approved dupilumab (Dupixent) prescription represents $25,000 to $40,000 in annual drug revenue. A denied authorization is not a billing problem — it is a patient care and financial problem simultaneously.
Which Biologics Require Prior Authorization
Virtually every biologic medication in dermatology requires prior authorization from commercial payers and Medicare Advantage plans. The most commonly prescribed biologics and their primary indications:
- Dupilumab (Dupixent) — Atopic dermatitis, prurigo nodularis. Requires documented moderate-to-severe disease (EASI >16 or IGA ≥3) and typically two prior conventional therapy failures.
- Secukinumab (Cosentyx) — Plaque psoriasis, psoriatic arthritis. Requires PASI or BSA documentation of moderate-to-severe disease.
- Ixekizumab (Taltz) — Plaque psoriasis, psoriatic arthritis. Similar prior auth requirements to secukinumab.
- Guselkumab (Tremfya) — Plaque psoriasis. IL-23 inhibitor; requires documented inadequate response to conventional therapy.
- Risankizumab (Skyrizi) — Plaque psoriasis. Similar pathway to guselkumab.
- Tralokinumab (Adbry) — Atopic dermatitis. Requires moderate-to-severe documented disease and prior conventional therapy failure.
- Adalimumab (Humira/biosimilars) — Plaque psoriasis, hidradenitis suppurativa. Step therapy to biosimilars increasingly required before branded adalimumab.
Building a Strong Biologic Authorization Request
Biologic authorization requests in dermatology must be built around the payer’s specific medical necessity criteria — which center on disease severity documentation and prior conventional therapy failure.
Disease severity documentation: Use validated scoring tools. PASI (Psoriasis Area and Severity Index), DLQI (Dermatology Life Quality Index), EASI (Eczema Area and Severity Index), IGA (Investigator Global Assessment), and BSA (Body Surface Area) are the tools payers cite in their criteria. Document severity scores in the clinical note at the biologic initiation visit — not just “moderate-to-severe psoriasis” as a narrative descriptor. Numeric scores are required.
Prior therapy documentation: Document every conventional therapy the patient has tried — drug name, dose, duration of treatment, and reason for failure (inadequate response, intolerance, or contraindication). Payers typically require at least two conventional systemic therapies before approving a biologic for psoriasis. For atopic dermatitis, the requirements vary by payer but typically include topical corticosteroids and topical calcineurin inhibitors.
Contraindication documentation: If the patient cannot try a required conventional therapy due to a medical contraindication, document the contraindication explicitly. Hepatic disease as a contraindication to methotrexate, renal impairment as a contraindication to cyclosporine — these documented contraindications are grounds for step therapy exemption under most payer policies and most state exemption laws.
Cosmetic vs. Medical Necessity: The Documentation-Driven Boundary
No other specialty has as many procedures that can be either covered or non-covered depending entirely on how they are documented. In dermatology, the cosmetic-medical boundary is not determined by what you do — it is determined by why you do it and how you record that reason.
Services That Live at the Boundary
Several common dermatology services fall at the cosmetic-medical boundary and require explicit medical necessity documentation to be covered:
Lesion removal: Sebaceous cysts, lipomas, and skin tags are covered when symptomatic — painful, inflamed, infected, or interfering with function. They are not covered when removed purely for cosmetic reasons. The ICD-10 code selection and clinical note must reflect the symptom or functional impact, not just the lesion’s existence.
Scar revision: Scar treatment is covered when the scar causes functional impairment — restriction of motion, interference with hygiene, or a documented functional limitation. It is not covered for purely cosmetic improvement. The clinical note must document the functional problem, not just the appearance concern.
Acne treatment: Medical management of acne — prescription topicals, oral antibiotics, isotretinoin — is medically necessary for inflammatory acne and is covered. Cosmetic procedures for acne scarring may not be covered depending on the payer and the documented indication.
Laser treatments: Laser treatment for vascular lesions (port wine stains, hemangiomas) is typically medically necessary and covered when clinically significant. Laser treatment for cosmetic redness reduction is typically not covered. The ICD-10 code and clinical documentation must reflect the clinical indication.
Billing Compliance Warning — ICD-10 Code Selection: In dermatology, ICD-10 code selection directly determines coverage status for borderline procedures. Using a cosmetic-indicating diagnosis code for a procedure that could be coded as medically necessary signals a non-covered service to the payer’s auto-adjudication system. Conversely, using a medical necessity code for a service performed for cosmetic reasons is billing fraud. Train clinicians to use diagnosis codes that accurately reflect the clinical indication — and ensure billing staff review the ICD-10 code against the clinical note for every cosmetic-adjacent procedure before submission.
Top Denial Causes in Dermatology Billing — and How to Fix Each One
Dermatology denial patterns are predictable and practice-wide. The same six denial categories appear in nearly every dermatology practice that has not built systematic prevention into its billing workflow. Fixing them reduces denial rates, accelerates collections, and removes the high administrative cost of working preventable claim failures.
Denial Cause 1: Modifier 25 Errors
Missing Modifier 25 when a same-day E&M is separately payable — or incorrectly adding Modifier 25 when the E&M is not separately identifiable — is the single most common dermatology claim failure. It appears on 25 to 35% of all dermatology denials in practices without a modifier review protocol.
The fix: require pre-claim review of every encounter that includes both an E&M code and a procedure code. The reviewer verifies that the clinical note documents a distinct problem for the E&M, that the E&M diagnosis is different from the procedure diagnosis, and that Modifier 25 is applied if and only if those conditions are met. Our medical coding services include Modifier 25 validation on every dermatology encounter before submission.
Denial Cause 2: Missing or Expired Prior Authorization for Biologics
Biologic drug denials carry the highest dollar values in dermatology. A single missed authorization for a dupilumab or secukinumab prescription can represent $3,000 to $8,000 per dose — and practices that do not track authorization renewal windows commonly deliver unauthorized doses across multiple cycles before the denial pattern is detected.
The fix is a biologic-specific authorization tracking system. Every patient on a biologic medication needs a confirmed authorization number, the authorized drug and dosage, the authorized date range or number of doses, and a renewal trigger at least two doses before the current authorization expires. Our revenue cycle management services include dedicated biologic authorization tracking for every active dermatology patient.
Denial Cause 3: Incorrect Lesion Removal Code Due to Wrong Size or Location Category
Using the lesion diameter instead of the excised diameter, selecting the wrong anatomical location category, or coding a shave removal as an excision — these are the three most common lesion procedure coding errors. Each selects a different CPT code and produces a systematic pattern of either underpayment or denial.
The fix: build a pre-billing code verification step that cross-checks the selected CPT code against the documented excised diameter, anatomical location, and procedure technique in the operative note. These three data points must align precisely. If they do not, the claim goes back to the coder for review before submission.
Denial Cause 4: Cosmetic vs. Medical Necessity Documentation Failure
ICD-10 codes that signal cosmetic indication, or clinical notes that fail to document a medical reason for a procedure that could be cosmetic, produce payer denials that are extremely difficult to appeal after the fact. The payer adjudicated based on the information in the claim — and the claim said cosmetic.
The fix: create a list of every procedure in your practice that exists at the cosmetic-medical boundary. For each of those procedures, document the required medical necessity elements in the clinical note template — symptoms, functional impact, prior conservative treatment, clinical rationale. This documentation audit happens before the visit note is finalized, not after the claim is denied.
Denial Cause 5: Biopsy Code Errors From Pre-2019 Coding Habits
Practices that have not fully updated their biopsy coding knowledge since the 2019 revision still use legacy codes or apply the new codes incorrectly — billing two primary biopsy codes instead of one primary and one add-on, or using 11102 for a punch biopsy that should be 11104. These errors produce systematic underbilling and occasional outright rejections from payers whose edits flag invalid code combinations.
The fix: conduct an annual biopsy code audit — pull 30 to 50 biopsy claims, trace each back to the operative note, verify technique documented, verify code selected, and verify add-on code use for multiple specimens. This audit quickly identifies whether staff is applying current coding logic correctly or using outdated patterns.
Denial Cause 6: Modifier 59 Used Without Supporting Documentation
Modifier 59 appended to override an NCCI edit, without clinical note documentation supporting that the two procedures were truly distinct, creates both a denial and an audit trigger. Payers increasingly review Modifier 59 usage in dermatology because it is among the most frequently misused modifiers in the specialty.
The fix: treat every claim with Modifier 59 as requiring an additional documentation review step. Before submission, confirm that the clinical note explicitly documents why the two billed services are distinct — different sites, different diagnoses, different specimens. If the documentation does not support Modifier 59, remove it and re-evaluate whether both procedures should be billed.
How Qualigenix Supports Dermatology Revenue Cycle Management
Qualigenix brings dermatology-specific billing expertise to every client engagement. We understand the lesion measurement requirements that drive excision code selection, the modifier hierarchy rules for multi-procedure encounters, the 2019 biopsy code updates, the biologic authorization tracking workflows, and the cosmetic-medical documentation standards that determine coverage status.
Our revenue cycle management services for dermatology cover the full billing cycle. Eligibility verification with dermatology-specific benefit checks — biologic benefit tier, step therapy requirements, prior authorization needed before each biologic dose. Lesion procedure coding with excised diameter verification against the operative note before every claim submission.
We manage prior authorizations for every active biologic patient — tracking authorization numbers, dose approval limits, and renewal timelines. Our denial management includes step therapy appeal support with AAD guideline citations and expedited peer-to-peer review coordination for patients with severe disease.
Our AR follow-up prioritizes biologic and Mohs claims by dollar value — high-value claims receive follow-up at 14 days, not 21 — and we track underpayments against fee schedules quarterly.
Clients achieve a 99% claim accuracy rate, a 95% first-pass acceptance rate, and a 30% reduction in AR days — with onboarding in as few as 6 days.
Dermatology RCM Checklist
Lesion Procedure Coding
- ☐ Excised diameter calculated (lesion + margins) and documented in operative note before code selection
- ☐ Anatomical location category confirmed (trunk/extremity vs. face/ears/nose vs. scalp/hands/feet)
- ☐ Procedure type confirmed — shave removal, benign excision, or malignant excision — from operative note
- ☐ Malignant excision codes (11600–11646) only used when histologic malignancy diagnosis is confirmed
- ☐ Destruction codes (17000/17003/17004) checked against total lesion count in the note
Biopsy Coding
- ☐ 2019 technique-based codes in use — no legacy codes in claim system
- ☐ Technique confirmed from operative note (tangential, punch, or incisional)
- ☐ Multiple biopsies: one primary code for highest-value technique; add-on codes for each additional specimen
- ☐ Each biopsy specimen documented separately with distinct site, technique, and lesion description
Modifier Compliance
- ☐ Modifier 25 on E&M code only when clinical note documents a distinct, separately identifiable E&M service
- ☐ Modifier 25 E&M diagnosis is different from the procedure diagnosis
- ☐ Modifier 59 only used when clinical note clearly documents distinct services (different site, diagnosis, or session)
- ☐ Modifier 51 on secondary procedures — never on add-on codes (CPT add-ons are Modifier 51 exempt)
Prior Authorization — Biologics
- ☐ Authorization confirmed for every biologic patient before every dose
- ☐ Authorization tracking log maintained by patient, drug, authorized dates, and renewal trigger date
- ☐ Disease severity score (PASI, DLQI, EASI, IGA) documented in clinical note for every biologic auth request
- ☐ Prior conventional therapy documented by drug name, dose, duration, and reason for failure
- ☐ Step therapy exemption grounds documented when conventional therapy is contraindicated
Cosmetic vs. Medical Necessity
- ☐ ICD-10 code reflects clinical indication — not cosmetic-signaling diagnosis codes
- ☐ Cosmetic-adjacent procedures reviewed: symptoms, functional impact, and medical rationale documented in note
- ☐ Patients informed of non-covered cosmetic service costs in writing before procedure
Denial Management
- ☐ All denials worked within 48 hours — biologic denials escalated same day
- ☐ Step therapy denials trigger peer-to-peer review request and AAD guideline citation within 24 hours
- ☐ Applicable state step therapy exemption law cited in every biologic step therapy appeal
- ☐ Denial root cause tracked monthly by category — modifier errors, auth failures, cosmetic/medical mix
Dermatology Revenue Cycle Management Glossary
Modifier 25
Appended to an evaluation and management (E&M) code to indicate that a significant, separately identifiable E&M service was performed on the same day as a procedure. In dermatology, Modifier 25 is the most frequently misused modifier — added incorrectly to pre-procedure assessments that are part of the procedure service, or omitted when a genuine separate problem is evaluated. The clinical note must document a distinct problem, distinct examination, and distinct decision-making separate from the procedure. CMS and commercial payers actively audit dermatology Modifier 25 usage.
Modifier 59
Appended to a procedure code to indicate a distinct procedural service that would otherwise be bundled under NCCI edits. In dermatology, Modifier 59 is required when procedures at different anatomical sites, with different diagnoses, or in different sessions are coded on the same claim and would otherwise be denied as bundled. Modifier 59 must be supported by explicit clinical note documentation of the distinctness — applying it routinely to override edits without documentation support is a compliance violation that creates audit and recoupment risk.
Excised Diameter
The measurement that determines the correct CPT code for lesion excision in dermatology. Excised diameter equals the widest lesion dimension plus the narrowest surgical margin on each side. It is not the same as lesion diameter. For a 1.5cm lesion excised with 0.2cm margins: excised diameter = 1.5 + 0.2 + 0.2 = 1.9cm. This number — documented explicitly in the operative note — controls which excision code is selected. Using lesion diameter instead of excised diameter is one of the most common and most correctable revenue losses in dermatology billing.
Medical Necessity
The payer requirement that a service is appropriate, reasonable, and necessary to diagnose or treat a patient’s condition. In dermatology, medical necessity is the dividing line between covered and non-covered procedures — particularly for services that can be performed for both cosmetic and medical reasons. Documentation in the clinical note — diagnosis, symptoms, functional impact, prior conservative treatment, and clinical rationale — establishes medical necessity. ICD-10 code selection must reflect the medical indication, not cosmetic intent.
Mohs Surgery
A specialized skin cancer excision technique in which the surgeon also interprets the frozen tissue sections at each stage — eliminating the need for a separate pathologist during the procedure. Billed using stage-based CPT codes (17311–17315) by anatomical location and stage count. Pathology interpretation is built into the Mohs codes — billing a separate pathology code for Mohs-controlled sections is unbundling. Mohs achieves the highest cure rates for basal cell and squamous cell carcinoma in complex anatomical sites where tissue conservation is critical.
NCCI Edits (National Correct Coding Initiative)
CMS-maintained tables defining CPT code combinations that should not be billed together because one service is considered a component of the other. In dermatology, NCCI edits affect same-day E&M and procedure billing (resolved with Modifier 25 when applicable), and certain procedure-procedure combinations (potentially resolvable with Modifier 59 when truly distinct). Routine use of modifiers to bypass NCCI edits without documentation is a compliance violation flagged in CMS Correct Coding Initiative education materials.
Step Therapy
A payer policy requiring patients to try and fail preferred treatments before the payer approves the requested treatment. In dermatology, step therapy is most aggressively applied to biologics for psoriasis and atopic dermatitis — requiring documented failure of at least two conventional systemic therapies before a biologic is approved. Over 30 states have enacted step therapy exemption laws. When conventional therapy is contraindicated, documenting the contraindication explicitly creates grounds for a step therapy exception without requiring the patient to try and fail the contraindicated agent.
Prior Authorization
Approval from a health insurance plan required before a provider can deliver certain services and receive reimbursement. In dermatology, prior authorization is required by most commercial payers and Medicare Advantage plans for biologic medications, Mohs surgery, phototherapy courses, and certain laser procedures. Authorization must be confirmed before the date of service — delivering an unauthorized biologic dose and billing for it produces a denial with no viable appeal pathway in most cases. Authorization windows for biologics typically align with prescription refill cycles and must be renewed proactively.
Frequently Asked Questions: Dermatology Revenue Cycle Management
What is dermatology revenue cycle management?
Dermatology RCM is the specialized billing and collections process for skin care practices — covering lesion excision and destruction coding by size and location, biopsy CPT selection by technique, modifier 25/51/59 rules for multi-procedure encounters, cosmetic vs. medically necessary documentation, prior authorization for biologics and Mohs surgery, and dermatology-specific denial management. It is uniquely complex because a single patient visit commonly produces three to five simultaneous codes, each with its own billing requirements.
What are the most common claim denial reasons in dermatology billing?
The top causes are: Modifier 25 errors — missing it when needed or using it without documentation support (25–35% of denials); missing or expired biologic prior authorization; medical necessity denials for cosmetic-adjacent procedures without proper documentation; incorrect lesion removal codes from wrong size or location category; outdated biopsy codes from pre-2019 habits; and Modifier 59 applied without clinical note documentation. Each is preventable with systematic pre-claim review.
How do I correctly code dermatology lesion removal?
Lesion removal coding requires three documented facts: procedure type (shave removal, benign excision, or malignant excision), excised diameter in centimeters (widest lesion + narrowest margin on each side), and anatomical location category (trunk/extremities vs. scalp/hands/feet vs. face/ears/eyelids/nose/lips). All three must be in the operative note. The excised diameter — not just the lesion diameter — controls CPT code selection for excisions.
When should I use Modifier 25 in dermatology?
Modifier 25 goes on the E&M code when the dermatologist provides a significant, separately identifiable evaluation and management service for a problem that is distinct from the reason for the procedure. The clinical note must document a separate problem with its own history, examination, and decision-making — and the E&M diagnosis code should be different from the procedure diagnosis code. Pre-procedure assessment for a scheduled procedure is not a separately identifiable E&M and does not qualify for Modifier 25.
What is the difference between Modifier 25, 51, and 59 in dermatology?
Modifier 25 goes on the E&M code — it signals a distinct, separately payable E&M service on a procedure day. Modifier 51 goes on secondary procedure codes in a multiple-procedure encounter — it signals multiple procedure payment reduction applies. Modifier 59 goes on a procedure code to override an NCCI bundling edit — it signals two services are distinct and separately payable despite the NCCI edit. Each requires different documentation and applies to a different billing scenario.
Does insurance cover cosmetic dermatology procedures?
Most purely cosmetic procedures are not covered. However, many services that appear cosmetic — symptomatic lesion removal, laser treatment for vascular lesions, scar revision for functional impairment — are medically necessary and billable when properly documented. The ICD-10 code and clinical note must document the medical diagnosis, symptoms, and functional impact. Without this documentation, the same procedure will be denied as cosmetic even when a legitimate medical indication exists.
How does Mohs surgery billing work?
Mohs surgery is billed per stage using CPT codes 17311–17315, selected by anatomical location (high-complexity site = 17311/17312; trunk/extremity = 17313/17314) and stage count. The surgeon is also the pathologist — pathology interpretation is built into the Mohs codes and cannot be separately billed alongside them. If multiple separate sites are treated on the same day, each site is billed with its own first-stage code. Prior authorization is required by many commercial payers and Medicare Advantage plans.
What prior authorizations does dermatology typically require?
Virtually all biologic medications for psoriasis, atopic dermatitis, and hidradenitis suppurativa require prior authorization — dupilumab, secukinumab, ixekizumab, guselkumab, risankizumab, tralokinumab, and adalimumab. Mohs surgery requires authorization from some commercial and Medicare Advantage payers. Phototherapy courses and certain laser procedures also require authorization from many plans. Traditional Medicare does not require prior auth for most dermatology procedures, but Medicare Advantage plans impose their own requirements.
How can dermatology practices reduce AR days?
Reduce AR days by verifying eligibility 48 hours before every appointment, confirming biologic authorizations before every dose, submitting clean claims within 24 hours of service, working all denials within 48 hours, and prioritizing high-dollar biologic and Mohs claims for same-day follow-up when they deny. A systematic pre-claim review process that catches modifier and coding errors before submission is the single highest-impact AR reduction lever. Outsourcing to an RCM partner like Qualigenix reduces AR days by up to 30%.
Should dermatology practices outsource their billing?
For most dermatology practices, yes — particularly when denial rates exceed 5%, AR days are above 45, or billing staff have turned over recently. Dermatology billing requires deep knowledge of lesion measurement-based code selection, modifier 25/59 rules, 2019 biopsy code revisions, Mohs stage-based coding, biologic authorization tracking, and cosmetic vs. medical necessity documentation. Generalist billing teams make predictable, systematic errors in each of these areas. A specialized partner brings the expertise and technology to capture more revenue per claim with fewer denials.
Related Resources
Qualigenix Service Pages:
- Revenue Cycle Management Services
- Medical Billing Outsourcing Services
- Denial Management Services
- AR Follow-Up Services
- Medical Coding Services
- Insurance Eligibility Verification
- Claim Submission Services
Related Blog Guides:
- What Is Revenue Cycle Management? Complete Guide
- Revenue Cycle Management Best Practices
- Oncology Revenue Cycle Management
- Medical Billing Outsourcing vs. In-House
- Denial Management Process: Essential Steps
- Accounts Receivable in Medical Billing
Dermatology Billing That Captures Every Dollar Your Practice Earns
Qualigenix brings dermatology-specific billing expertise to every engagement — from lesion measurement-based code selection to biologic authorization management to Modifier 25/59 compliance and step therapy appeals.
Our dermatology clients achieve 99% claim accuracy, a 95% first-pass acceptance rate, a 30% reduction in AR days, and an average 36-day collection cycle. We onboard in as few as 6 days.
Precision. Progress. Qualigenix.
What’s Next
Real-time eligibility returned active and the claim still denied: the five reasons why
An “active” eligibility result only proves the policy is in force. It never proves the service is covered, that...
Prior authorization turnaround requirements under the CMS interoperability rule: what changed for practices
The CMS interoperability rule (CMS-0057-F) forces impacted payers to decide standard prior authorizations in 7 calendar days and...
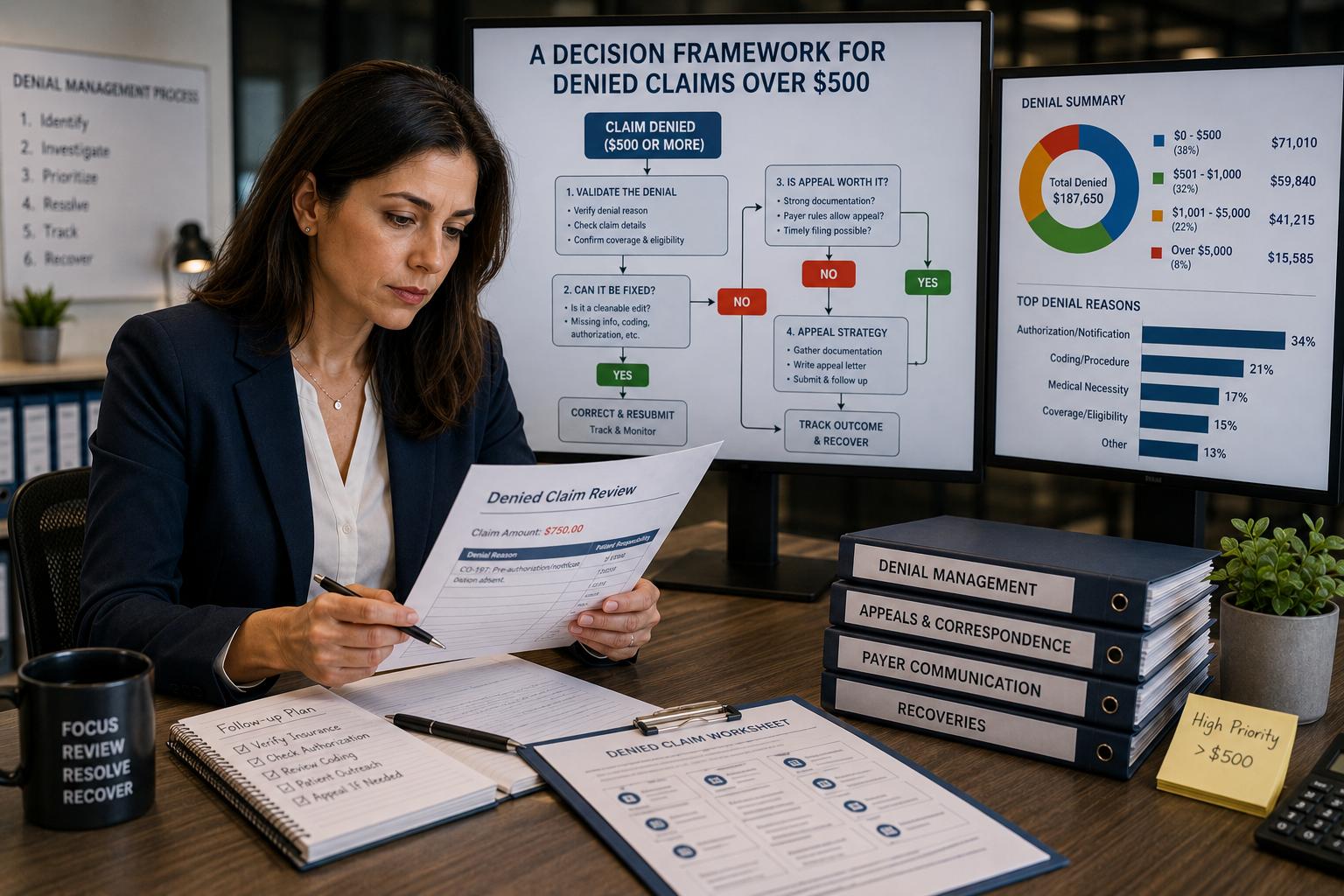
Appeal or Write Off? A Decision Framework for Denied Claims Over $500
Don’t let the dollar amount make the call by itself. Sort the denial by reason code, run the...