Oncology Revenue Cycle Management: Guide for Cancer Care Practices 2026
The Qualigenix Editorial Team consists of certified billing and coding experts with over 40 years of experience across 38+ medical specialties. Our content is rigorously researched against CMS, AMA, and payer-specific guidelines to ensure total compliance and accuracy. We apply the same elite standards to our resources as we do our client work, consistently delivering high claim accuracy and significant reductions in AR days.

Oncology billing is unlike any other specialty in medicine. Drug costs represent 60 to 80% of total revenue. A single incorrect J-code unit calculation or missing NDC number on a $40,000 chemotherapy claim costs more than a week of average medical office revenue. Add prior authorization battles for immunotherapy, 340B compliance requirements, clinical trial billing rules, and step therapy denials — and you have a billing environment where errors are expensive, fast, and easy to make. This guide covers J-code billing, buy-and-bill, 340B, clinical trial compliance, step therapy appeals, and the workflows that help Qualigenix clients achieve a 99% claim accuracy rate, 95% first-pass acceptance, and a 30% reduction in AR days.
No other specialty puts as much financial pressure on billing as oncology. In a typical cardiology or orthopedic practice, billing errors cost hundreds of dollars per claim. In oncology, a single drug billing error on a CAR-T cell therapy claim can cost $400,000. That is not a billing department problem. That is a practice-survival problem.
Oncology revenue cycle management is distinct from every other specialty. It requires mastery of drug-specific J-codes and NDC numbers, daily familiarity with chemotherapy dosing protocols, working knowledge of 340B drug pricing rules, clinical trial billing compliance, and a systematic strategy for fighting step therapy denials with NCCN guideline citations.
Generalist billing teams do not have these skills. And the consequences of that gap are not just operational — they show up directly in the financial viability of the practice.
This guide gives you the complete picture of oncology RCM — where the revenue is, where it leaks, and how to build a billing process that captures every dollar of the complex care your oncology team delivers.
Oncology revenue cycle management is the specialized billing and collections process for cancer care practices. It covers chemotherapy drug billing using J-codes and NDC numbers, prior authorization for cancer treatments, administration code billing, clinical trial billing compliance, oral chemotherapy reimbursement, 340B drug pricing program management, and oncology-specific denial management — all tailored to a specialty where drug costs represent 60 to 80% of total practice revenue.
Why Oncology Billing Is Different From Every Other Specialty
Ask an experienced oncology biller what separates this specialty from others, and the answer is immediate: the drug revenue. In family medicine or dermatology, billing errors cost $100 to $300 per claim. In oncology, a single drug billing error on a high-cost immunotherapy claim can cost $20,000 to $50,000. A CAR-T cell therapy billing failure can cost ten times that.
Three factors make oncology billing fundamentally different.
Drug Costs Dominate the Revenue Stream
In most medical practices, physician services (E&M visits, procedures) drive the majority of revenue. In oncology, the relationship is inverted. Chemotherapy drugs — billed separately from the physician’s professional fee — represent 60 to 80% of a typical oncology practice’s total revenue.
This matters because drug billing is more complex, more error-prone, and more consequential than any other billing category. Getting J-code selection, unit calculation, NDC numbers, and administration code hierarchy right on every drug claim is not optional. It is the core financial function of the practice.
The Buy-and-Bill Model Creates Unique Financial Risk
The dominant drug reimbursement system in oncology is buy-and-bill. The practice purchases chemotherapy drugs at acquisition cost — then bills the payer at the contracted reimbursement rate after administration. The difference between what the practice pays for the drug and what the payer reimburses is the drug margin.
This model works when billing is accurate. It fails when claims are denied, underpaid, or coded with incorrect units. A denied buy-and-bill claim leaves the practice holding the acquisition cost with no reimbursement. At $5,000 to $50,000 per infusion encounter, that exposure is significant.
Regulatory Complexity Layered on Top of Clinical Complexity
Oncology billing does not just require clinical knowledge of cancer drugs. It requires compliance knowledge across multiple overlapping regulatory frameworks: 340B drug pricing rules, Medicare Part B drug billing requirements, clinical trial billing compliance under the Medicare Clinical Trial Policy, and state-level step therapy exemption laws. Each one creates compliance obligations that, if violated, generate not just denials but audit risk and potential recoupment demands.
What makes oncology billing different from other specialties?
Three things: drug costs represent 60 to 80% of practice revenue — far more than any other specialty; the buy-and-bill model means billing errors leave the practice holding drug acquisition costs with no reimbursement; and multiple overlapping regulatory frameworks — 340B rules, Medicare Part B drug requirements, clinical trial billing compliance, and step therapy laws — create compliance obligations that generalist billing teams are not equipped to manage.
Oncology Revenue Cycle Benchmarks
| Metric | Typical Oncology Practice | Best Practice Target | Qualigenix |
|---|---|---|---|
| Denial Rate | 12–20% | Under 5% | <5% |
| Clean Claim Rate | 68–80% | 95%+ | 95% |
| Days in AR | 45–65 days | 30–38 days | 36 days avg. |
| Prior Auth Denial Share | 30–40% of all denials | Near zero with tracking | Systematic auth management |
| Medical Necessity Denial Share | 20–30% of all denials | Under 8% with NCCN documentation | NCCN guideline appeals included |
| J-Code Unit Error Rate | Est. 15–20% of drug claims | Under 1% with dosage review | Dosage calculation review included |
| Drug Costs as Share of Revenue | 60–80% | Maximize drug margin capture | Drug revenue capture optimized |
| Medicare Drug Reimbursement Rate | ASP + 6% | Collect 100% of allowed | Underpayment detection included |
| 340B Drug Discount vs. Market | 25–50% below average market price | Maximize margin with JG modifier compliance | 340B billing compliance built-in |
| Peer-to-Peer Overturn Rate (Oncology) | 60%+ when NCCN supports treatment | Maximize with preparation | Peer-to-peer facilitated |
| States with Step Therapy Exemption Laws | 30+ states as of 2026 | Know and cite applicable state law | State law tracking included |
| Claim Accuracy Rate | 68–82% | 95%+ | 99% |
| AR Days Reduction Post-Outsourcing | — | 20–30% | 30% within first quarter |
| Onboarding Time | 2–4 weeks (typical vendor) | Under 2 weeks | As few as 6 days |
Sources: ASCO Practice Survey 2025; ACCC Oncology Billing and Reimbursement Report 2025; CMS Oncology Billing Guidelines 2026; Qualigenix internal performance data 2026.
J-Code Billing: The Financial Engine of Oncology RCM
J-codes are HCPCS Level II codes that identify specific injectable and infusible medications billed in a clinical setting. In oncology, J-codes are how chemotherapy drug revenue flows from clinical care to reimbursement. Getting them right on every claim is the most important billing function in any oncology practice.
How J-Codes Work
Every injectable or infusible chemotherapy drug has one or more J-codes assigned by CMS. The J-code identifies the drug by name. The number of units billed identifies the dose. Most J-codes are defined per a specific measurement unit — per mg, per 10mg, per 100mg, or per vial.
For example: J9035 is bevacizumab (Avastin), billed per 10mg. A patient receiving 400mg of bevacizumab requires 40 units (400 ÷ 10 = 40). Bill 39 units and you undercharge by $700 to $1,500 depending on the payer rate. Bill 41 units and you overbill — creating audit risk and potential recoupment.
This calculation happens for every drug, every cycle, every patient. In a busy infusion suite with 20 to 40 patients per day receiving multiple agents, even a small systematic error rate produces significant revenue loss or compliance risk over time.
Commonly Billed Oncology J-Codes
| J-Code | Drug Name (Brand) | Unit | Drug Category |
|---|---|---|---|
| J9035 | Bevacizumab (Avastin) | Per 10mg | Targeted therapy / VEGF inhibitor |
| J9070 | Cyclophosphamide | Per 100mg | Alkylating chemotherapy |
| J9355 | Trastuzumab (Herceptin) | Per 10mg | HER2-targeted therapy |
| J9306 | Pembrolizumab (Keytruda) | Per 1mg | Immunotherapy / PD-1 inhibitor |
| J9299 | Nivolumab (Opdivo) | Per 1mg | Immunotherapy / PD-1 inhibitor |
| J9173 | Docetaxel (Taxotere) | Per 1mg | Taxane chemotherapy |
| J9264 | Paclitaxel (Taxol) | Per 1mg | Taxane chemotherapy |
| J9025 | Azacitidine (Vidaza) | Per 1mg | Hypomethylating agent — hematology |
| J9310 | Rituximab (Rituxan) | Per 100mg | Anti-CD20 monoclonal antibody |
| J9217 | Leuprolide Acetate (Lupron) | Per 3.75mg | Hormonal therapy — prostate cancer |
| J9228 | Ipilimumab (Yervoy) | Per 1mg | Immunotherapy / CTLA-4 inhibitor |
| J9144 | Daratumumab (Darzalex) | Per 10mg | Anti-CD38 — multiple myeloma |
NDC Numbers: The Medicare and Medicaid Requirement
Medicare and Medicaid require a National Drug Code (NDC) number on every claim for a separately billable drug. The NDC is an 11-digit code identifying the specific drug product — manufacturer, strength, and package size.
Every oncology claim for Medicare and Medicaid must include the NDC number in addition to the J-code. The format is specific: NDC qualifier (N4), the 11-digit NDC number, the unit qualifier, and the quantity dispensed. Missing or incorrect NDC numbers generate claim rejections that require correction and resubmission before payment occurs.
The billing challenge: different vial sizes of the same drug have different NDC numbers. If a patient receives bevacizumab from two different vial sizes in the same infusion (common when vials are mixed to minimize waste), both NDC numbers must appear on the claim. Billing teams need real-time access to drug inventory and vial tracking data to get NDC numbers right on high-volume oncology claims.
Warning — J-Code Unit Calculation: J-code unit errors are among the most common and most costly billing mistakes in oncology. The most frequent pattern: billing units based on the ordered dose rather than the actual administered dose. If a patient’s dose is rounded down from 420mg to 400mg due to vial availability, the billed units must reflect 400mg — not 420mg. Billing the ordered dose instead of the administered dose is systematic overbilling that creates recoupment risk. Drug administration records, not physician orders, control the correct unit count.
Chemotherapy Administration Codes: Billing the Service, Not Just the Drug
Every chemotherapy infusion encounter generates two categories of charges: the drug charge (J-codes) and the administration charge (CPT codes). Missing either category leaves money on the table. Using the wrong hierarchy produces bundling denials.
Administration CPT Codes in Oncology
The correct administration code depends on the type of administration (infusion, push, or injection) and whether it is the initial or a subsequent drug in the encounter.
Chemotherapy infusion codes:
- CPT 96413 — Chemotherapy administration, intravenous infusion, initial substance, up to 1 hour. This is the initial infusion code — bill once per encounter for the first chemotherapy drug infused.
- CPT 96415 — Each additional hour of the same drug infusion (add-on to 96413).
- CPT 96417 — Each additional sequential infusion of a different chemotherapy agent (add-on).
Non-chemotherapy infusion codes (for supportive agents):
- CPT 96365 — Non-chemotherapy infusion, initial substance, up to 1 hour. Use for hydration agents, antiemetics, and supportive drugs.
- CPT 96366 — Each additional hour of the same non-chemo infusion.
- CPT 96367 — Each additional sequential infusion of a different non-chemo agent.
- CPT 96368 — Concurrent infusion — a second drug running simultaneously with the primary infusion.
Chemotherapy injection codes:
- CPT 96401 — Chemotherapy administration, subcutaneous or intramuscular injection.
- CPT 96402 — Hormonal antineoplastic therapy, subcutaneous or intramuscular.
- CPT 96409 — Chemotherapy administration by intravenous push, initial substance.
- CPT 96411 — Each additional substance pushed IV (add-on to 96409).
The Hierarchy Rule: Getting the Initial Code Right
Medicare and most commercial payers apply a strict hierarchy to administration codes. The “initial” code (96413 or 96409) can only be billed once per encounter — for the first drug in the infusion sequence. Every subsequent drug uses the “additional” or “sequential” codes.
The most common hierarchy error in oncology: billing 96413 for each drug in a multi-drug regimen instead of billing 96413 once and 96417 for each subsequent drug. Payers deny the additional 96413 codes and pay only one. The result: the practice loses administration revenue on every subsequent drug in every multi-drug regimen.
In FOLFOX (a common colorectal cancer regimen with oxaliplatin, leucovorin, and fluorouracil), the correct billing is: 96413 × 1 (first drug), 96415 for additional hours of the same drug, then 96417 × 2 for the two sequential additional drugs. Billing three 96413 codes is wrong and generates predictable denials.
What is the difference between 96413 and 96417 in oncology billing?
CPT 96413 is the initial chemotherapy infusion code — billed once per encounter for the first drug. CPT 96417 is the sequential chemotherapy infusion add-on code — billed for each additional, different chemotherapy drug infused after the first. In a multi-drug regimen like FOLFOX, billing 96413 for each drug is wrong and generates bundling denials. Bill 96413 once, then 96417 for each subsequent drug.
The Buy-and-Bill Model: Managing Drug Revenue and Margin
The buy-and-bill model creates a unique financial dynamic in oncology that does not exist in other specialties. The practice takes on both the clinical and financial risk of drug administration — and the billing accuracy determines whether that risk pays off or creates losses.
How Buy-and-Bill Works
The practice purchases chemotherapy drugs from a wholesaler or directly from a manufacturer at acquisition cost. The drugs are stored in the practice pharmacy or medication room, tracked by lot number and NDC, and dispensed to patients at each infusion visit. After administration, the billing team submits a claim using the appropriate J-code and unit count. The payer reimburses at the contracted rate — typically Average Sales Price (ASP) plus 6% for Medicare, or a negotiated rate for commercial payers.
The drug margin is the difference between acquisition cost and reimbursement. For most drugs, at ASP+6%, the margin is modest. For 340B-eligible practices, the margin is substantially larger because the acquisition cost is 25 to 50% below market while the reimbursement rate remains unchanged.
What Destroys Drug Margin
Three billing failures eat into drug margin faster than anything else.
J-code unit errors. Billing fewer units than administered means collecting less than the contracted reimbursement for the drug dispensed. The practice paid full acquisition cost. The billing team billed partial reimbursement. The shortfall comes directly out of drug margin.
Claim denials on drug charges. A denied J-code claim leaves the practice holding the full acquisition cost with zero reimbursement. At $3,000 to $40,000 per infusion encounter depending on the drug, even a 5% drug claim denial rate generates enormous revenue exposure.
Incorrect ASP pricing. Medicare ASP rates update quarterly. Billing at an outdated ASP rate — either higher (audit risk) or lower (revenue loss) than the current quarter — produces systematic errors across every Medicare claim for that drug. Keep ASP rate tables current and update billing system fee schedules every quarter.
340B Drug Pricing: The Compliance-Revenue Balance
The 340B Drug Pricing Program is one of the most powerful financial tools available to eligible oncology organizations — and one of the highest-compliance-risk areas in oncology billing.
Who Qualifies for 340B
340B eligibility extends to certain categories of hospitals — disproportionate share hospitals (DSH), children’s hospitals, critical access hospitals, rural referral centers — as well as federally qualified health centers (FQHCs) and Ryan White HIV/AIDS Program grantees. Most community oncology practices are NOT 340B-eligible. Hospital-based or FQHC-based oncology programs often are.
How 340B Changes the Drug Margin Equation
A 340B-eligible oncology program purchases drugs at the 340B ceiling price — which can be 25 to 50% below the average market price for many cancer drugs. The reimbursement rate from Medicare and commercial payers does not change — it is still ASP+6% for Medicare. The result is a larger spread between acquisition cost and reimbursement.
For a drug with a commercial acquisition cost of $10,000 and a Medicare reimbursement of $10,600 (ASP+6%), the standard buy-and-bill margin is $600. A 340B acquisition cost of $6,000 for the same drug produces a $4,600 margin on the same claim. The revenue impact across a busy infusion program is substantial.
340B Billing Compliance: The JG Modifier and Split-Billing
Medicare requires 340B-acquired drugs to be identified on claims with Modifier JG. Without JG, Medicare pays the standard ASP+6% rate — it does not penalize for missing JG. But it can identify the discrepancy during audit and demand repayment of the excess margin if the practice was not compliant with 340B billing rules.
340B split-billing is the practice of tracking which patients received 340B-acquired drugs versus non-340B drugs and billing each correctly. Hospital outpatient departments and contract pharmacy arrangements add additional complexity. The core compliance requirement: 340B drugs cannot be billed for Medicare patients and non-340B drugs billed for Medicaid patients to capture the Medicaid rebate — this is prohibited duplicate discounting.
Pro Tip — 340B Audit Risk: CMS and the Health Resources and Services Administration (HRSA) have increased 340B audit activity significantly since 2023. The two most common audit findings are duplicate discounting (billing Medicaid for a drug that already received a 340B discount) and contract pharmacy compliance failures. If your organization participates in 340B, maintain documented drug tracking records by patient, payer, and NDC number — and review your contract pharmacy arrangements against current HRSA policy annually.
Prior Authorization in Oncology: The Biggest Revenue Risk
Prior authorization is the largest denial driver in oncology billing. It accounts for 30 to 40% of all oncology denials — and these denials carry the highest dollar values. A denied authorization for a pembrolizumab (Keytruda) course can represent $150,000 to $300,000 in annual drug revenue for a single patient.
Which Oncology Treatments Require Prior Authorization
Most commercial payers and Medicare Advantage plans require prior authorization for:
- Immunotherapy agents — pembrolizumab, nivolumab, ipilimumab, atezolizumab, durvalumab
- Targeted therapy agents — trastuzumab, bevacizumab, cetuximab, pertuzumab, imatinib
- CAR-T cell therapies — axicabtagene ciloleucel (Yescarta), tisagenlecleucel (Kymriah)
- PARP inhibitors — olaparib, niraparib, rucaparib
- CDK4/6 inhibitors (often covered under pharmacy benefit)
- Bone marrow stimulating agents — filgrastim, pegfilgrastim
- Hormonal therapies — leuprolide, degarelix, enzalutamide, abiraterone
- Radiation sensitizers and novel agents at payer discretion
Traditional Medicare does not require prior authorization for most Part B chemotherapy drugs. Medicare Advantage plans do — and their criteria vary by plan and formulary.
Building a Strong Authorization Request
Authorization requests for oncology treatments need to be built around the payer’s specific medical necessity criteria — which are typically based on NCCN Clinical Practice Guidelines. A strong oncology authorization request includes:
Pathology confirmation: The diagnosis confirmed by pathology, including histology, grade, and stage. For targeted therapies, include biomarker test results — HER2 status for trastuzumab, PD-L1 expression for pembrolizumab, BRCA mutation status for PARP inhibitors.
NCCN category citation: The specific NCCN guideline category (Category 1, 2A, 2B) for the requested treatment in the patient’s specific cancer type, stage, and biomarker profile. Category 1 evidence means uniform NCCN consensus based on high-level evidence — the strongest possible authorization argument.
Prior treatment history: For step therapy requirements, document any prior treatments tried and their outcomes. If the payer requires a prior therapy the patient cannot receive due to contraindication, document the contraindication explicitly.
Cycle schedule and duration: The specific dosing schedule, cycle frequency, and anticipated treatment duration. Authorization windows in oncology typically align with treatment cycles — know your payer’s authorization renewal requirements before the first cycle begins.
Step Therapy in Oncology: The Most Contentious Denial Category
Step therapy — the payer requirement to try and fail one or more preferred treatments before approving the requested agent — creates more conflict in oncology than in any other specialty. Cancer treatment is not a one-size-fits-all domain. A drug that is the preferred treatment for one patient’s tumor profile may be clinically inappropriate for another’s.
Why Step Therapy Is Particularly Problematic in Oncology
Step therapy fails in oncology for a fundamental clinical reason: cancer treatment selection depends on tumor histology, stage, and biomarker profile. A step therapy requirement designed around a common scenario may be clinically impossible to satisfy for a patient with a specific mutation or contraindication.
Requiring a patient with HER2-positive breast cancer to fail generic chemotherapy before approving trastuzumab — the NCCN Category 1 recommended first-line treatment for HER2+ disease — is not clinically rational. It delays guideline-recommended therapy and potentially harms the patient. More than 30 states have enacted step therapy exemption laws specifically to prevent this.
Step Therapy Exemption Laws
State step therapy exemption laws vary in their requirements but generally require payers to grant a step therapy exception when:
- The required step therapy agent is clinically contraindicated for the specific patient
- The patient has previously tried and failed the required step therapy agent
- The required step therapy agent is not clinically appropriate for the patient’s specific condition
- The requested treatment is NCCN Category 1 recommended for the patient’s specific indication
Know which states have enacted step therapy exemption laws and how to cite them in authorization requests and appeals. The combination of a state exemption law citation and NCCN Category 1 evidence resolves the majority of step therapy denials in oncology when properly documented.
What is step therapy and how does it affect oncology patients?
Step therapy is a payer policy requiring patients to try and fail one or more preferred drugs before the payer approves coverage for the requested treatment. In oncology, step therapy requirements frequently conflict with NCCN guideline-recommended first-line treatments for specific cancer types and biomarker profiles. Over 30 states have enacted step therapy exemption laws requiring payers to grant exceptions when the required step therapy agent is contraindicated or clinically inappropriate. Citing applicable state law and NCCN Category 1 evidence resolves most step therapy denials.
Clinical Trial Billing Compliance: A Mandatory Expertise Area
Oncology practices that enroll patients in clinical trials face a billing compliance requirement that has no equivalent in other specialties. The Medicare Clinical Trial Policy — and analogous policies for Medicaid and commercial payers — defines exactly what you can bill to insurance and what charge to the trial sponsor. Getting this wrong is not just a billing error. It is a False Claims Act compliance risk.
What you can bill to Insurance During a Clinical Trial
Routine costs of care — services the patient would receive regardless of trial participation — you can bill to Medicare and most payers. Routine costs include: conventional care items and services consistent with standard medical care for the patient’s diagnosis, the physician’s E&M visits related to cancer management, and supportive care services not unique to the trial protocol.
Investigational items — the experimental drug itself, tests done solely to collect research data, and items provided solely to satisfy protocol requirements — charge to the trial sponsor. They cannot be billed to Medicare, Medicaid, or commercial payers.
The Compliance Risk: Mixed Billing
The most common clinical trial billing error is mixed billing — charging to payers for items that should be funded by the trial sponsor. This happens when billing teams do not have a clear per-patient, per-claim review process that identifies which charges for a trial patient are routine care and which are research costs.
The consequences of mixed billing extend beyond denial. CMS and the Office of Inspector General (OIG) treat improper clinical trial billing as a False Claims Act violation — potentially triggering federal audit, repayment demands, and civil monetary penalties. A clinical trial billing compliance program is not optional for oncology practices that enroll patients in trials.
Oral Chemotherapy Billing: The Pharmacy-Medical Benefit Divide
Oral chemotherapy drugs create a billing pathway problem that infused drugs do not face. Infused chemotherapy is a medical benefit — billed to the medical insurance using J-codes. Most oral cancer drugs are pharmacy benefits — dispensed through a pharmacy, covered by the patient’s prescription drug benefit, and billed using NDC codes rather than J-codes.
The Oral Chemotherapy Parity Problem
Under most health plans, infused chemotherapy is subject to the patient’s medical benefit cost-sharing — typically 20% of allowed charges after the deductible. Oral chemotherapy covered under the pharmacy benefit is subject to the pharmacy cost-sharing structure — which often means much higher out-of-pocket costs for the patient.
More than 45 states have enacted oral chemotherapy parity laws requiring commercial health plans to cover oral cancer drugs under the same cost-sharing terms as infused cancer drugs. But enforcement varies, patient education is incomplete, and many oncology practices do not have a systematic process for identifying when a patient’s oral chemotherapy is subject to parity protections and advocating for the patient when it is not.
In-House Pharmacy Billing for Oral Agents
Oncology practices with in-house dispensing pharmacies have the option to dispense oral chemotherapy directly to patients. When billed through the in-house pharmacy, oral chemotherapy uses NDC billing under the medical benefit — generating both the drug revenue and the dispensing fee. This requires pharmacy licensure, a pharmacy billing workflow separate from the medical billing process, and payer-specific authorization for in-house oral dispensing.
Top Denial Causes in Oncology Billing — and How to Fix Each One
Oncology denial patterns are predictable. Most practices face the same 6 denial categories repeatedly. Fixing them systematically recovers far more revenue than working individual claims one at a time — and prevents the high-dollar losses that compound quickly in a drug-intensive specialty.
Denial Cause 1: Missing or Expired Prior Authorization
Missing or expired authorization causes 30 to 40% of oncology denials and carries the highest dollar values. An immunotherapy authorization denial can represent $15,000 to $30,000 per infusion cycle. A CAR-T authorization denial represents the cost of the entire CAR-T therapy — often $400,000 to $500,000.
The fix is a treatment-level authorization tracking system. Every patient on active chemotherapy needs a confirmed authorization number, authorized drug(s), authorized cycle schedule, and a renewal trigger when the current authorization is within 2 cycles of expiration. Review it weekly for every active patient.
Denial Cause 2: J-Code Unit Errors
J-code unit errors — billing the wrong number of units for the administered dose — are the most financially significant coding error in oncology. Underbilling loses drug margin. Overbilling creates audit and recoupment risk. Both are preventable with a pre-billing drug administration record review.
The fix: require billing staff to reconcile every J-code unit count against the drug administration record before claim submission. The administered dose — not the ordered dose, not the rounded dose, not the vial size — controls the correct unit count. Our medical coding services include dosage calculation review on every oncology drug claim.
Denial Cause 3: Missing NDC Numbers
Missing NDC numbers on Medicare and Medicaid claims generate automatic claim rejections. The claim does not enter adjudication — it comes back immediately as a reject requiring correction and resubmission. Every day of delay means a day of delayed drug reimbursement on a high-value claim.
The fix: integrate NDC tracking into the drug administration workflow. Every drug dispensed from the infusion pharmacy should generate an administration record that includes the NDC number. The billing system should pull NDC numbers from administration records automatically — not require billing staff to look them up manually for each claim.
Denial Cause 4: Administration Code Hierarchy Errors
Billing 96413 (initial infusion) for each drug in a multi-drug regimen instead of billing 96413 once and 96417 for subsequent drugs is one of the most common administration code errors in oncology. Payers deny the additional 96413 codes and pay only one. The practice loses administration revenue on every drug after the first in every multi-drug encounter.
The fix: build administration code hierarchy rules into the billing system so multi-drug regimens automatically generate the correct code sequence. Our claim submission services include administration code hierarchy verification on every oncology encounter before submission.
Denial Cause 5: Step Therapy Denials
Step therapy denials in oncology are among the most complex to appeal but also among the most winnable when handled correctly. The key is speed — cancer patients cannot wait weeks for a standard appeal process while treatment is delayed.
The fix is a step therapy exemption workflow that triggers immediately upon denial receipt: identify the applicable state exemption law, pull the NCCN guideline category for the denied treatment, compile the clinical documentation, and request an expedited peer-to-peer review within 24 hours of the denial. Expedited reviews are typically completed within 72 hours — fast enough to prevent treatment interruption for most patients.
Denial Cause 6: Clinical Trial Billing Compliance Errors
Billing payers for investigational items that charge to the trial sponsor is a denial cause and a compliance risk simultaneously. The payer denies the claim because the item is not a covered benefit for non-trial patients. The compliance risk comes from having billed a federally funded program for a research cost.
The fix is a clinical trial billing compliance matrix — a per-protocol document for each active trial that identifies which services are routine care (billable to payers) and which are investigational (charged to the sponsor). Every trial patient’s claims review against the compliance matrix before submission. This is not optional for any oncology practice enrolled in federally funded trials.
How Qualigenix Supports Oncology Revenue Cycle Management
Qualigenix brings oncology-specific billing expertise to every client engagement. We understand the J-code dosage calculation requirements, the NDC number tracking workflows, the 340B compliance obligations, the step therapy appeal process using NCCN guidelines, and the clinical trial billing compliance framework.
Our revenue cycle management services for oncology practices cover the full billing cycle. Eligibility verification with oncology-specific benefit checks — medical benefit vs. pharmacy benefit for each drug, prior authorization requirements, and specialty pharmacy coordination. Drug claim coding with dosage calculation review on every J-code claim before submission.
We manage prior authorizations for every active patient on chemotherapy — tracking authorization numbers, cycle windows, and renewal timelines so the practice never delivers a treatment without confirmed authorization. Our denial management includes NCCN guideline-supported step therapy appeals and expedited peer-to-peer review coordination.
For oncology practices with 340B programs, we build JG modifier compliance into the billing workflow and maintain split-billing documentation. For practices with clinical trial patients, we provide per-protocol billing compliance review before every claim submission.
Our AR follow-up prioritizes oncology claims by dollar amount — high-value drug claims get follow-up at 14 days, not 21 — and we reconcile drug claim payments against current ASP rates quarterly to detect underpayments.
Clients achieve a 99% claim accuracy rate, a 95% first-pass acceptance rate, and a 30% reduction in AR days — with onboarding in as few as 6 days.
Oncology RCM Checklist
Drug Billing (J-Codes and NDC)
- ☐ J-code unit count verified against drug administration record before every claim submission
- ☐ NDC number pulled from administration record — not manual lookup — for every Medicare and Medicaid claim
- ☐ ASP rates updated in billing system every quarter for all active drug codes
- ☐ 340B drugs identified and billed with Modifier JG on Medicare claims
- ☐ 340B split-billing records maintained by patient, payer, and NDC
Administration Code Hierarchy
- ☐ 96413 billed once per encounter — 96417 for each subsequent chemotherapy drug
- ☐ 96365 used for non-chemotherapy supportive agents — not 96413
- ☐ 96368 used for concurrent infusions — not additional 96413 or 96417
- ☐ Administration hours calculated from infusion start/stop times in nursing notes
Prior Authorization
- ☐ Authorization confirmed for every patient before every treatment cycle
- ☐ Authorization tracking log maintained by patient, drug, authorized cycles, and expiration date
- ☐ Renewal request submitted 2 cycles before current authorization expires
- ☐ NCCN category cited in every authorization request for targeted and immunotherapy agents
Clinical Trial Billing
- ☐ Per-protocol compliance matrix created for every active clinical trial
- ☐ Every trial patient’s claims reviewed against compliance matrix before submission
- ☐ Investigational items charged to trial sponsor — not billed to any payer
Denial Management
- ☐ All denials worked within 48 hours — drug denials escalated same day
- ☐ Step therapy denials trigger expedited peer-to-peer review request within 24 hours
- ☐ NCCN guideline category cited in every step therapy and medical necessity appeal
- ☐ Applicable state step therapy exemption law cited when relevant
Oncology Revenue Cycle Management Glossary
J-Code
HCPCS Level II codes identifying injectable and infusible medications billed in a clinical setting. In oncology, J-codes identify specific chemotherapy drugs by name and dosage unit. The number of units billed must match the actual administered dose — not the ordered dose, not the vial size. Medicare and Medicaid claims require an accompanying NDC number. J-code unit errors are the most common and most financially significant coding error in oncology billing.
Buy-and-Bill
The dominant drug reimbursement model in oncology. The practice purchases chemotherapy drugs at acquisition cost, administers them to patients, then bills the payer using J-codes at the contracted reimbursement rate. The drug margin — the difference between acquisition cost and reimbursement — depends entirely on billing accuracy. Denied drug claims leave the practice holding acquisition cost with no reimbursement.
Average Sales Price (ASP)
The CMS pricing benchmark for Medicare Part B drugs, updated quarterly. Medicare reimburses most chemotherapy drugs at ASP plus 6%. Knowing current ASP rates for every active drug in the formulary is essential for accurate drug margin management. ASP rates change quarterly — billing systems must be updated every quarter to reflect current CMS ASP pricing.
340B Drug Pricing Program
A federal program allowing eligible healthcare organizations to purchase outpatient drugs at discounted prices — typically 25 to 50% below market. 340B-eligible oncology programs purchase drugs at discounted rates and bill Medicare and commercial payers at standard ASP-based rates, generating larger drug margins. Medicare requires 340B-acquired drugs to be identified with Modifier JG. Duplicate discounting — billing Medicaid for 340B drugs that already received the Medicaid rebate — is prohibited.
Step Therapy (Fail First)
A payer utilization management policy requiring patients to try and fail preferred drugs before the payer approves the requested treatment. In oncology, step therapy frequently conflicts with NCCN guideline-recommended first-line treatments for specific cancer types and biomarker profiles. Over 30 states have enacted step therapy exemption laws requiring payers to grant exceptions when the required step therapy agent is contraindicated, previously failed, or clinically inappropriate.
NCCN Guidelines
Clinical Practice Guidelines in Oncology published by the National complete Cancer Network — the standard clinical reference for oncology treatment decisions in the United States. NCCN assigns categories of evidence to treatment recommendations: Category 1 (uniform consensus, high-level evidence), Category 2A (uniform consensus, lower-level evidence), Category 2B (non-uniform consensus), Category 3 (major disagreement). Citing NCCN Category 1 evidence in prior authorization requests and appeals is the strongest possible clinical argument for oncology treatment coverage.
National Drug Code (NDC)
An 11-digit identifier for every drug product — manufacturer, strength, and package size. Medicare and Medicaid require NDC numbers on claims for separately billable drugs. Every oncology J-code claim for Medicare and Medicaid must include the correct NDC number of the specific drug administered. Missing NDC numbers generate automatic claim rejections. Different vial sizes of the same drug carry different NDC numbers — both must appear on claims when multiple vial sizes are mixed in one infusion.
Chemotherapy Administration Codes
CPT codes billing the infusion or injection service for chemotherapy — separate from the drug J-code charges. Key codes: 96413 (chemo infusion, initial hour — billed once per encounter), 96415 (each additional hour of same drug), 96417 (each additional sequential drug infused), 96401 (subcutaneous or intramuscular injection), 96409 (IV push, initial). Correct hierarchy payers require: 96413 bills once, 96417 for each subsequent drug. Billing multiple 96413 codes in a multi-drug regimen generates bundling denials.
Frequently Asked Questions: Oncology Revenue Cycle Management
What is oncology revenue cycle management?
Oncology RCM is the specialized billing and collections process for cancer care practices — covering J-code drug billing with accurate unit calculations and NDC numbers, prior authorization for cancer treatments, administration code hierarchy, clinical trial billing compliance, oral chemotherapy reimbursement, 340B drug pricing compliance, and oncology-specific denial management.
What are J-codes in oncology billing?
J-codes are HCPCS Level II codes identifying injectable and infusible medications billed in a clinical setting. In oncology, J-codes identify specific chemotherapy drugs and their dosage units. The number of billed units must match the actual administered dose. Medicare and Medicaid claims require an NDC number alongside each J-code. J-code unit errors are the most common and most costly coding error in oncology.
What causes the most denials in oncology billing?
The top causes are: missing or expired prior authorization for high-cost cancer drugs (30–40% of denials), medical necessity denials from insufficient documentation (20–30%), J-code unit errors, missing NDC numbers, administration code hierarchy errors in multi-drug regimens, step therapy denials, and clinical trial billing compliance errors. Each is preventable with the right process.
How does the buy-and-bill model work in oncology?
The practice buys chemotherapy drugs at acquisition cost, administers them to patients, then bills the payer at the contracted reimbursement rate using J-codes. The drug margin — the difference between acquisition cost and reimbursement — depends entirely on billing accuracy. Denied drug claims leave the practice holding acquisition cost with no reimbursement. 340B-eligible practices earn larger margins by purchasing drugs at significantly discounted prices.
What is the 340B Drug Pricing Program?
340B allows eligible healthcare organizations to purchase outpatient drugs at 25 to 50% below market price while billing Medicare and commercial payers at standard reimbursement rates, generating larger drug margins. Medicare requires 340B drugs to be billed with Modifier JG. Duplicate discounting — billing Medicaid for drugs that already received the Medicaid rebate — is prohibited. HRSA audit activity has increased significantly since 2023.
How does prior authorization work for oncology treatments?
Authorization requests require pathology confirmation of diagnosis and biomarker status, NCCN guideline category for the requested treatment, prior treatment history for step therapy requirements, and the proposed dosing schedule. Most commercial payers and Medicare Advantage plans require authorization for immunotherapy, targeted therapy, CAR-T, and hormonal agents. Authorization windows align with treatment cycles and must be renewed before expiration.
What is step therapy and how does it affect oncology patients?
Step therapy requires patients to try and fail preferred drugs before the payer approves the requested treatment. In oncology, this frequently conflicts with NCCN guideline-recommended first-line treatments for specific cancer types and biomarker profiles. Over 30 states have enacted step therapy exemption laws. Citing the applicable state law and NCCN Category 1 evidence — and requesting an expedited peer-to-peer review — resolves most step therapy denials.
What is clinical trial billing compliance in oncology?
Clinical trial billing compliance governs what you can bill to Medicare, Medicaid, or commercial payers when a patient is enrolled in a clinical trial. Routine care costs — services the patient would receive regardless of trial participation — you can bill to payers. Investigational items — the experimental drug, research-only tests — charge to the trial sponsor. Mixing research costs and payer charges on the same claim violates the False Claims Act.
Should an oncology practice outsource revenue cycle management?
For most oncology practices, yes. Oncology billing requires deep expertise in J-code dosage calculations, NDC tracking, 340B compliance, step therapy appeals, and clinical trial billing compliance that generalist billing teams consistently miss. An outsourced partner with oncology RCM expertise reduces denials, captures drug revenue accurately, and manages the compliance requirements that carry audit and recoupment risk.
How does Qualigenix help oncology practices with RCM?
Qualigenix provides end-to-end oncology RCM — J-code dosage calculation review, NDC number tracking, 340B billing compliance, administration code hierarchy verification, prior authorization management, NCCN guideline-supported step therapy appeals, clinical trial billing compliance review, and AR follow-up prioritized by dollar amount. Clients achieve 99% claim accuracy, 95% first-pass acceptance, and 30% reduction in AR days with onboarding in as few as 6 days.
Related Resources
Qualigenix Service Pages:
- Revenue Cycle Management Services
- Medical Billing Outsourcing Services
- Denial Management Services
- AR Follow-Up Services
- Medical Coding Services
- Insurance Eligibility Verification
- Claim Submission Services
Related Blog Guides:
- What Is Revenue Cycle Management? Complete Guide
- Revenue Cycle Management Best Practices
- Cardiology Revenue Cycle Management
- Medical Billing Outsourcing vs. In-House
- Denial Management Process: Essential Steps
- Accounts Receivable in Medical Billing
Oncology Billing That Protects Your Drug Revenue — and Your Compliance
Qualigenix brings oncology-specific billing expertise to every engagement — from J-code dosage calculations to 340B compliance to NCCN guideline-supported step therapy appeals.
Our oncology clients achieve 99% claim accuracy, a 95% first-pass acceptance rate, a 30% reduction in AR days, and an average 36-day collection cycle. We onboard in as few as 6 days.
Precision. Progress. Qualigenix.
What’s Next
Real-time eligibility returned active and the claim still denied: the five reasons why
An “active” eligibility result only proves the policy is in force. It never proves the service is covered, that...
Prior authorization turnaround requirements under the CMS interoperability rule: what changed for practices
The CMS interoperability rule (CMS-0057-F) forces impacted payers to decide standard prior authorizations in 7 calendar days and...
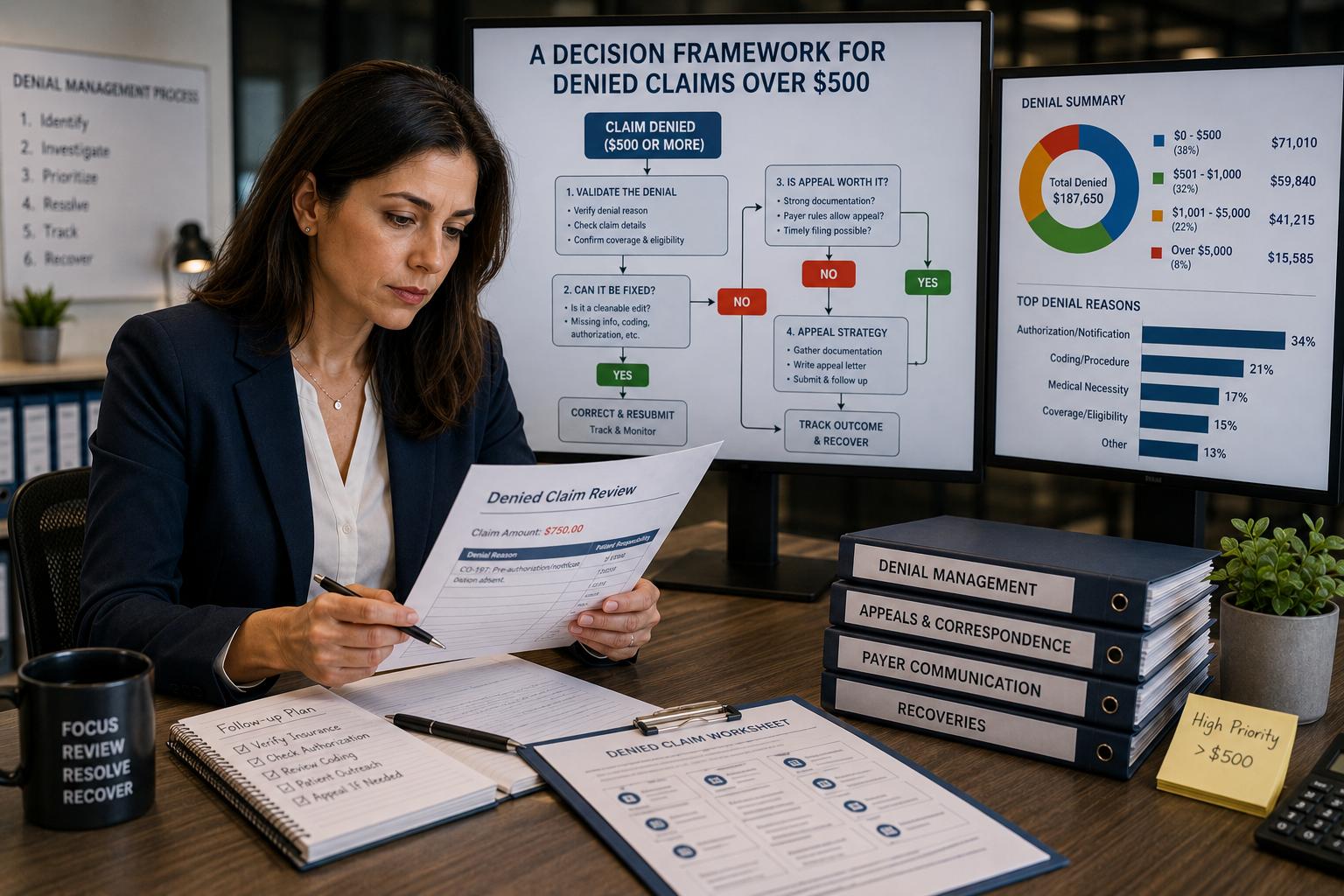
Appeal or Write Off? A Decision Framework for Denied Claims Over $500
Don’t let the dollar amount make the call by itself. Sort the denial by reason code, run the...