Cardiology Revenue Cycle Management: Guide for Cardiology Practices 2026
The Qualigenix Editorial Team consists of certified billing and coding experts with over 40 years of experience across 38+ medical specialties. Our content is rigorously researched against CMS, AMA, and payer-specific guidelines to ensure total compliance and accuracy. We apply the same elite standards to our resources as we do our client work, consistently delivering high claim accuracy and significant reductions in AR days.

Cardiology billing is among the most complex — and highest-stakes — in all of medicine. High-value procedures, strict prior authorization requirements, global period rules, professional vs. facility fee splits, and cardiology-specific modifier requirements create a billing environment where errors are expensive and denials are common. Cardiology practices without specialist billing support typically see denial rates of 10 to 18% and lose significant revenue to undercoded procedures and missed modifier opportunities. This guide covers everything: CPT coding for diagnostic and interventional cardiology, prior authorization, global periods, modifier rules, denial management, and the workflows that help Qualigenix clients achieve a 99% claim accuracy rate, 95% first-pass acceptance, and a 30% reduction in AR days.
Cardiology practices face a billing challenge that most other specialties do not: the procedures are high-value, the rules are complex, and a single billing error can cost thousands of dollars. A missed modifier on a cardiac catheterization. A prior authorization that expired before the procedure date. A post-operative E&M visit billed during a 90-day global period without the right modifier. Each one generates a denial that could have been prevented.
Cardiology revenue cycle management is not a variation of general medical billing. It is a distinct specialty with its own CPT code structure, its own modifier requirements, its own prior authorization landscape, and its own high-dollar denial patterns that generalist billing teams consistently miss.
This guide gives you the full picture — what makes cardiology RCM unique, where revenue leaks, and how to build a billing process that captures every dollar your clinical team earns.
Cardiology revenue cycle management is the specialized billing and collections process for cardiology practices. It covers cardiology-specific CPT coding for diagnostic and interventional procedures, prior authorization for high-cost cardiac services, modifier application for bilateral and multiple procedures, global period billing rules, professional vs. facility fee coordination, denial management, and AR follow-up — all tailored to the high-value, high-complexity billing environment of cardiology.
Why Cardiology Billing Is Different From General Medical Billing
Ask any experienced cardiology biller what separates this specialty from others, and the answer is consistent: the stakes are higher and the rules are stricter. A billing error in a family medicine practice costs $80. The same category of error in interventional cardiology costs $8,000.
Three factors make cardiology billing fundamentally different from general medical billing.
High-Value Procedures With Complex Coding Requirements
Cardiology procedures carry some of the highest CPT code reimbursements in outpatient medicine. A left heart catheterization with coronary angiography (CPT 93458) generates $600 to $900 in professional fees and $3,000 to $8,000 in facility fees. A percutaneous coronary intervention (CPT 92928) generates $1,500 to $2,500 in professional fees and $8,000 to $20,000 in facility fees.
These are not simple codes. Correct billing requires accurate selection from a family of related codes, correct modifier application, proper documentation of the specific vessels treated, and coordination between the professional fee and the facility fee claim. A single wrong code or missing modifier on a high-value cardiology claim generates a denial worth more than a week of average medical office revenue.
Extensive Prior Authorization Requirements
Prior authorization requirements in cardiology are more extensive than in almost any other outpatient specialty. Stress testing, echocardiography, cardiac catheterization, PCI, implantable devices, electrophysiology studies, and cardiac imaging all require authorization from most commercial payers and Medicare Advantage plans.
The authorization process for a high-cost cardiac procedure requires detailed clinical documentation — patient symptoms, cardiac history, prior workup results, and a clinical rationale demonstrating the procedure is medically necessary under the payer’s criteria. Getting this wrong — or missing the authorization entirely — generates a denial worth thousands of dollars that is often non-appealable.
Strict Post-Operative Billing Rules
Cardiac surgical procedures carry 90-day global periods. During those 90 days, Medicare and most commercial payers bundle all routine post-operative care into the surgical procedure payment. Billing separately for a post-operative visit during the global period — without the correct modifier — generates a denial. And unlike coding errors, global period violations often cannot be recovered through appeal because the services were legitimately included in the global fee.
What makes cardiology billing harder than general medical billing?
Three things: high-value procedures with complex CPT coding and modifier requirements where errors cost thousands; extensive prior authorization for cardiac procedures where a missing authorization can result in a non-appealable denial worth $5,000 to $50,000; and strict global period rules for cardiac surgical procedures where billing errors during the 90-day post-operative window generate permanent revenue loss.
Cardiology Revenue Cycle Benchmarks
| Metric | Typical Cardiology Practice | Best Practice Target | Qualigenix |
|---|---|---|---|
| Denial Rate | 10–18% | Under 5% | <5% |
| Clean Claim Rate | 70–82% | 95%+ | 95% |
| Days in AR | 40–60 days | 30–38 days | 36 days avg. |
| Claim Accuracy Rate | 72–85% | 95%+ | 99% |
| Prior Auth Denial Share | 25–35% of all denials | Near zero with tracking | Systematic auth management |
| Medical Necessity Denial Share | 20–30% of all denials | Under 8% with documentation | Documentation review included |
| Modifier Error Denial Share | 10–15% of all denials | Under 2% with scrubbing | Pre-submission scrub included |
| Peer-to-Peer Overturn Rate | 50–70% of well-prepared appeals | Maximize with preparation | Peer-to-peer facilitated |
| Left Heart Cath — Professional Fee (93458) | $600–$900 | Collect 100% of allowed | Underpayment detection included |
| PCI Single Vessel — Professional Fee (92928) | $1,500–$2,500 | Collect 100% of allowed | Underpayment detection included |
| Transthoracic Echo — Professional Fee (93306) | $150–$250 | Collect 100% of allowed | Underpayment detection included |
| Global Period — Major Cardiac Surgery | 90 days | Zero global period violations | Global period tracking included |
| AR Days Reduction Post-Outsourcing | — | 20–30% | 30% within first quarter |
| Onboarding Time | 2–4 weeks (typical vendor) | Under 2 weeks | As few as 6 days |
Sources: MGMA Cost and Revenue Survey 2025; ACC Advocacy and Health Policy Report 2025; CMS Cardiology Billing Guidelines 2026; Qualigenix internal performance data 2026.
Cardiology CPT Coding: Diagnostic vs. Interventional
Cardiology CPT coding divides into two broad categories: diagnostic services that evaluate cardiac function without intervention, and interventional services that deliver treatment. Each has different coding structures, different reimbursement levels, and different documentation requirements.
Diagnostic Cardiology CPT Codes
Diagnostic cardiology covers the services that assess cardiac structure and function — echocardiography, stress testing, cardiac monitoring, electrocardiography, and diagnostic imaging. These are the most frequently billed cardiology codes and the ones most often miscoded.
Electrocardiography:
- CPT 93000 — ECG with at least 12 leads, with interpretation and report. The global code — billed when the same physician owns the equipment and interprets the tracing.
- CPT 93005 — ECG, tracing only. Technical component only — no interpretation.
- CPT 93010 — ECG, interpretation and report only. Professional component only — use when another provider owns and operates the ECG equipment.
Echocardiography:
- CPT 93306 — Transthoracic echocardiography (TTE) with Doppler and color flow. The most frequently billed echo code for a complete study.
- CPT 93307 — TTE without Doppler. Use when Doppler is not performed — billing 93306 without Doppler documentation is a coding error.
- CPT 93308 — TTE follow-up or limited study. Use when a complete study is not performed.
- CPT 93312 — Transesophageal echocardiography (TEE), including probe placement, image acquisition, interpretation, and report.
- CPT 93351 — Stress echocardiography, complete, with interpretation and report.
Cardiac Stress Testing:
- CPT 93015 — Cardiovascular stress test, complete (physician supervision, ECG monitoring, interpretation, and report). Global code.
- CPT 93016 — Cardiovascular stress test, physician supervision only. Use when the physician supervises but does not interpret.
- CPT 93017 — Cardiovascular stress test, tracing only without interpretation.
- CPT 93018 — Cardiovascular stress test, interpretation and report only. The professional component — use when the facility owns and operates the treadmill equipment.
Cardiac Monitoring:
- CPT 93224–93227 — Holter monitor recording and analysis, 24–48 hours.
- CPT 93228–93229 — Mobile cardiovascular telemetry, up to 30 days.
- CPT 93241–93248</ — External electrocardiographic recording services (event monitors, extended Holter).
Cardiac Catheterization CPT Codes
Cardiac catheterization codes cover diagnostic left heart and right heart catheterization procedures. Code selection depends on which chambers are catheterized, what studies happen, and whether angiography is included.
- CPT 93451 — Right heart catheterization, including measurement of oxygen saturation and cardiac output.
- CPT 93452 — Left heart catheterization, including left ventriculography when performed.
- CPT 93453 — Combined right and left heart catheterization, including measurements and ventriculography when performed.
- CPT 93454 — Coronary angiography, without left heart catheterization.
- CPT 93455 — Coronary angiography with right heart catheterization.
- CPT 93456 — Coronary angiography with right heart and left heart catheterization.
- CPT 93457 — Coronary angiography with right and left heart catheterization, including left ventriculography.
- CPT 93458 — Left heart catheterization with coronary angiography. One of the most commonly billed catheterization codes.
- CPT 93459 — Left heart catheterization with coronary angiography and left ventriculography.
- CPT 93460 — Right and left heart catheterization with coronary angiography.
- CPT 93461 — Right and left heart catheterization with coronary angiography and left ventriculography.
Warning — Catheterization Code Selection: Selecting the wrong catheterization code is one of the most expensive coding errors in cardiology. Billing 93452 (left heart cath only) when 93458 (left heart cath with coronary angiography) happened underbills significantly. Billing 93458 when only 93454 (coronary angiography without left heart cath) happened is upcoding. The procedure note must document exactly which chambers were catheterized, which measurements were taken, and whether ventriculography happened — this documentation controls the correct code.
Interventional Cardiology CPT Codes
Interventional cardiology codes cover therapeutic procedures performed during cardiac catheterization. These are the highest-value codes in cardiology and carry the strictest documentation and authorization requirements.
Percutaneous Coronary Intervention (PCI):
- CPT 92928 — Percutaneous transcatheter placement of intracoronary stent, single vessel.
- CPT 92929 — PCI, each additional vessel (add-on to 92928).
- CPT 92933 — PCI with atherectomy, single vessel.
- CPT 92934 — PCI with atherectomy, each additional vessel (add-on).
- CPT 92937 — PCI, restenotic stent, single vessel.
- CPT 92941 — PCI during acute myocardial infarction, single vessel.
- CPT 92943 — PCI, chronic total occlusion, single vessel.
- CPT 92944 — PCI, chronic total occlusion, each additional vessel (add-on).
Structural Heart Procedures:
- CPT 33477 — Transcatheter pulmonary valve implantation (TPVI/TAVR equivalent for pulmonic valve).
- CPT 33361–33366 — Transcatheter aortic valve replacement (TAVR), depending on approach.
- CPT 33418–33419 — Transcatheter mitral valve repair.
Pacemaker and ICD Implantation:
- CPT 33206–33208 — Insertion of pacemaker (single chamber, dual chamber) with transvenous electrodes.
- CPT 33223, 33230, 33231 — ICD implantation, single or dual chamber.
- CPT 33274–33275 — Leadless pacemaker implantation or removal.
Electrophysiology (EP) Study Codes
EP studies evaluate the heart’s electrical conduction system and guide ablation therapy. These are among the most complex coding scenarios in cardiology.
- CPT 93600 — Bundle of His recording.
- CPT 93610 — Intraatrial pacing.
- CPT 93612 — Intraventricular pacing.
- CPT 93620 — complete EP study without induction.
- CPT 93621 — complete EP study with left atrial pacing and recording (add-on).
- CPT 93650 — Intracardiac catheter ablation, AV node.
- CPT 93653 — complete EP study with ablation of focal atrial tachycardia or flutter.
- CPT 93654 — complete EP study with ablation of ventricular tachycardia.
- CPT 93656 — complete EP study with pulmonary vein isolation (PVI) for atrial fibrillation.
The Modifier Minefield: Getting Cardiology Modifiers Right
Modifier errors are one of the top three denial causes in cardiology billing. The combination of high-value procedures, multiple services performed in a single session, and strict payer bundling rules creates numerous scenarios where the wrong modifier — or a missing one — generates a preventable denial.
Modifier 26 — Professional Component
Modifier 26 indicates that only the professional component (physician interpretation and written report) of a diagnostic service bills. The technical component (equipment, supplies, technical staff) bills separately by the facility.
In cardiology, Modifier 26 applies when a cardiologist interprets a study — an echocardiogram, nuclear stress test, cardiac CT, or cardiac MRI — performed at a hospital or independent imaging center that separately bills for the technical component.
When does Modifier 26 NOT apply? When the cardiologist’s practice owns the equipment and performs the technical component. In that case, they bill the global CPT code (no modifier) and collect both the professional and technical reimbursement.
The most common error: a hospital cardiologist interprets an echo performed in the hospital’s echo lab, but bills the global CPT 93306 instead of CPT 93306-26. The hospital separately bills for the technical component (CPT 93306-TC). Both claims go to the payer. The payer sees two claims for the technical component and denies one or both.
Modifier 59 and the X-Modifiers
Modifier 59 — Distinct Procedural Service — indicates that two or more procedures performed on the same day are distinct and independent. Without Modifier 59, payers may bundle multiple cardiology procedures into a single payment.
CMS introduced four more specific X-modifiers to replace many Modifier 59 uses:
- XS — Separate structure (different anatomical site)
- XP — Separate practitioner
- XE — Separate encounter (different session)
- XU — Unusual non-overlapping service
In cardiology, Modifier 59 or XS is frequently required when a cardiologist performs both a diagnostic catheterization and a PCI during the same session. Without the modifier, payers may bundle the diagnostic cath payment into the PCI reimbursement — treating the cath as integral to the PCI rather than as a separately billable diagnostic procedure.
Global Period Modifiers
During the 90-day global period following major cardiac surgery, several modifiers allow separate billing for services that are not part of the global package:
- Modifier 24 — Unrelated E&M service during the postoperative period. Use when a patient is seen during the global period for a condition unrelated to the original surgery. Documentation must clearly support the unrelated nature of the visit.
- Modifier 25 — Separately identifiable E&M service on the same day as a procedure. Use when an E&M service happens on the same day as a procedure with a global period and the E&M is distinct from the pre-operative assessment.
- Modifier 57 — Decision for surgery. Use when the E&M visit results in the initial decision to perform major surgery. This modifier allows billing for the pre-operative visit even when surgery happens the same day or next day.
- Modifier 79 — Unrelated procedure during the postoperative period. Use when a procedure unrelated to the original surgery happens during the global period.
What is the global period in cardiology billing?
A global period is the post-operative window during which Medicare and most payers bundle routine follow-up care into the surgical procedure payment. Major cardiac surgical procedures carry a 90-day global period. During those 90 days, billing separately for routine post-operative visits generates denials. Only services unrelated to the surgery — or services meeting specific exceptions — you can bill separately with the correct modifier (24, 25, 57, or 79).
Prior Authorization for Cardiology: Managing the Biggest Revenue Risk
Prior authorization is the single biggest revenue risk in cardiology billing. A denied authorization for a $15,000 PCI or a $50,000 TAVR is not a billing department problem — it is a practice revenue crisis. Managing authorization proactively is not optional in cardiology. you need.
Which Cardiology Procedures Require Prior Authorization
Most commercial payers and Medicare Advantage plans require prior authorization for:
- Cardiac catheterization (diagnostic and interventional)
- Percutaneous coronary intervention (PCI)
- Stress testing (exercise and pharmacological)
- Stress echocardiography
- Nuclear cardiology imaging (myocardial perfusion imaging)
- Cardiac CT and CTA
- Cardiac MRI
- Pacemaker and ICD implantation
- Electrophysiology studies and catheter ablation
- TAVR, TMVR, and other structural heart procedures
- Loop recorder implantation
- Cardiac rehabilitation programs
Traditional Medicare (fee-for-service) does not require prior authorization for most cardiology procedures — but Medicare Advantage plans do, and their criteria vary by plan.
What Payers Require in the Authorization Request
Authorization requests for cardiology procedures typically require:
Clinical documentation — Patient’s cardiac history, current symptoms and functional class (NYHA classification for heart failure, CCS classification for angina), relevant cardiac test results (prior ECG, echo, stress test, Holter data), and a clinical narrative explaining why the procedure is necessary.
Diagnostic workup results — For PCI authorization, payers want to see prior non-invasive workup results showing ischemia or hemodynamically significant obstruction. A catheterization authorization request without supporting non-invasive evidence is often denied at first submission.
ACC/AHA guideline citations — Many payers use Milliman or InterQual criteria based on ACC/AHA guideline recommendations. Knowing which guideline class applies to the planned procedure and citing it in the authorization request strengthens the approval probability significantly.
Authorization Tracking for Cardiology Practices
Cardiology practices with active cardiac catheterization lab programs schedule high-value procedures multiple times per week. Each one needs a valid authorization. Each authorization has an expiration date. Each one has an authorized CPT code set that may not cover add-on procedures discovered during the case.
Authorization tracking in cardiology requires more than a simple spreadsheet. It needs to capture: the authorized CPT codes, the authorization period, the procedure date, and — critically — whether the actual procedure performed during the case matches the authorized codes. When a diagnostic cath converts to a PCI (an ad hoc PCI), a separate authorization may be required, depending on the payer.
Pro Tip — Ad Hoc PCI Authorization: When a diagnostic catheterization converts to an ad hoc PCI during the same session, authorization requirements vary by payer. Some payers cover the PCI under the diagnostic catheterization authorization if the clinical necessity is documented in the procedure note. Others require a separate PCI authorization, even for same-session interventions. Know your payers’ ad hoc PCI policies before the procedure — not after the claim is denied.
Professional vs. Facility Fee Billing in Cardiology
Many cardiology procedures happen in hospital cardiac catheterization labs or ambulatory surgical centers — not in the cardiologist’s office. This creates a split billing situation that requires precise coordination between two separate claims.
How the Split Works
The cardiologist submits a professional fee claim (CMS-1500) for their physician services. This claim uses cardiology CPT codes and — when the facility owns the technical equipment — appends Modifier 26 to indicate the professional component only.
The hospital or ASC submits a facility fee claim (UB-04) for the equipment, room, nursing, and technical staff. This claim uses the same CPT codes (or revenue codes, depending on the payer) but reflects the facility’s costs rather than the physician’s services.
Both claims go to the same payer for the same patient encounter. The payer adjudicates them separately and applies different fee schedules — the physician fee schedule for the professional claim and the hospital outpatient prospective payment system (OPPS) or ASC payment system for the facility claim.
Common Split-Billing Errors in Cardiology
Error 1: Billing the global code instead of Modifier 26. A hospital cardiologist bills CPT 93306 (global echocardiography) instead of CPT 93306-26 (professional component only). The hospital separately bills CPT 93306-TC for the technical component. The payer receives two claims for the technical component and denies one or both.
Error 2: Billing Modifier 26 when the practice owns the equipment. A practice-based cardiologist bills CPT 93306-26 even though the practice owns and operates the echo equipment. The practice should bill the global code (CPT 93306) and collect both components. Billing Modifier 26 voluntarily reduces reimbursement by the technical component value.
Error 3: Missing Modifier 26 on nuclear stress tests. Nuclear cardiology studies performed at a hospital nuclear medicine department require Modifier 26 on the cardiologist’s professional claim. Missing this modifier on high-value nuclear studies (CPT 78452, 78453, 78454) generates denials or overpayment recovery requests.
Top Denial Causes in Cardiology Billing — and How to Fix Each One
Cardiology denial patterns are predictable. Most practices face the same 6 denial categories repeatedly. Fixing them systematically recovers far more revenue than working individual claims one at a time.
Denial Cause 1: Missing or Expired Prior Authorization
Missing or expired authorization accounts for 25 to 35% of cardiology denials — and these are the most expensive. A PCI denial worth $15,000 represents more revenue than a week of general office billing. A TAVR denial worth $50,000 or more can destabilize a small practice’s cash flow.
The fix is a procedure-level authorization tracking system. Every scheduled cardiology procedure needs a confirmed authorization number, authorized CPT codes, authorization period, and a flag for any scheduled procedures approaching the authorization expiration date. Review it daily for a busy catheterization lab program.
Denial Cause 2: Medical Necessity Denial
Medical necessity denials account for 20 to 30% of cardiology claim denials. They almost always point to one of two problems: insufficient clinical documentation in the authorization request or procedure note, or payer criteria that diverge from ACC/AHA guideline recommendations.
The documentation fix is a pre-procedure checklist that ensures every cardiology procedure note contains the elements payers require — patient symptoms and functional class, relevant diagnostic findings, prior treatment history, and a clear clinical rationale matching the payer’s criteria language. The appeal fix for criteria-based denials: cite the specific ACC/AHA guideline class supporting the procedure in your appeal letter and request a peer-to-peer review with a cardiologist reviewer.
Denial Cause 3: Modifier Errors
Modifier errors account for 10 to 15% of cardiology denials. Missing Modifier 26 on professional component claims. Missing Modifier 59 on same-session diagnostic and interventional procedures. Incorrect global period modifiers. Wrong modifier on bilateral procedures. Each one generates a denial that pre-submission claim scrubbing would have caught.
The fix: implement dual-layer pre-submission claim scrubbing — practice management system edits plus clearinghouse scrubbing — with cardiology-specific modifier rules programmed into the editing logic. Our claim submission services include cardiology modifier review on every claim before submission.
Denial Cause 4: Catheterization Code Selection Errors
The cardiac catheterization code family (93451–93461) has 11 codes covering different chamber combinations, studies performed, and whether angiography is included. Selecting the wrong code — billing 93452 when 93458 happened, or billing 93458 when only 93454 applies — generates denials or underpayments.
Code selection errors in cardiac cath typically trace to two problems: the procedure note does not clearly document which chambers were catheterized and which studies were performed, or the billing team selects a default code rather than reviewing the procedure note for each case.
The fix is a cardiology-specific coding review on every catheterization claim — comparing the billed code to the procedure note documentation before submission. Our medical coding services include procedure note review for every cardiac catheterization case.
Denial Cause 5: Global Period Violations
Global period violations occur when a cardiologist bills for a service during the 90-day post-operative global period without the correct modifier. The most common scenario: a patient who had coronary bypass surgery returns for a follow-up visit 30 days post-operatively. The visit is routine post-operative care — bundled in the surgical global fee. Billing it as a separate E&M without Modifier 24 (unrelated visit) generates a denial.
The fix is a global period tracking flag in the practice management system. Every patient who undergoes a major cardiac surgical procedure should have a 90-day global period flag attached to their record — visible to schedulers and billing staff — that triggers a modifier review before any service during that window bills.
Denial Cause 6: Bundling Errors on Combined Diagnostic and Interventional Cases
When a diagnostic catheterization converts to a PCI during the same session, payers may bundle the diagnostic cath payment into the PCI reimbursement — treating the diagnostic portion as integral to the intervention. Preventing this requires Modifier 59 (or XS) on the diagnostic catheterization code to indicate it was a distinct, separately performed service.
Without Modifier 59, the payer pays the PCI at the full PCI rate and denies the diagnostic cath as a bundled component. The cardiologist loses the diagnostic cath reimbursement ($600 to $900 professional fee) on every combined case.
What is the peer-to-peer review process for cardiology denials?
A peer-to-peer review is a direct conversation between the treating cardiologist and the payer’s medical reviewer who issued the denial. Request it through the payer’s utilization management department, typically within 10 to 14 days of the denial. In cardiology, peer-to-peer reviews are especially effective — the reviewing physician is often a cardiologist who recognizes guideline-supported clinical indications. Overturn rates of 50 to 70% are common in well-prepared cardiology peer-to-peer reviews. Request one on every medical necessity denial before moving to a formal written appeal.
Cardiology-Specific AR Management: High-Dollar Claims Need Proactive Follow-Up
Standard AR follow-up processes are designed for average claim values of $150 to $300. Cardiology AR includes claims worth $10,000 to $50,000 or more. The same 21-day follow-up standard applies — but the urgency and the stakes are different.
Prioritize by Dollar Amount, Not Just by Age
In most practices, AR follow-up is sorted by claim age — oldest claims first. In cardiology, dollar amount matters as much as age. A 25-day-old PCI claim worth $18,000 deserves faster follow-up than a 45-day-old office visit claim worth $180. Sort your cardiology AR queue by both age AND dollar amount. High-dollar cardiology claims approaching 30 days unpaid need active payer outreach — not a place in a queue behind lower-value claims.
Track Structural Heart Procedure Claims Separately
TAVR, TMVR, structural heart interventions, and complex EP procedures generate claims worth $50,000 to $200,000 or more on the facility side. These claims warrant individual tracking outside the standard AR workflow. Assign a dedicated follow-up owner for each high-value structural heart claim. Check status weekly from day 14. Escalate immediately if any documentation request or additional information (AI) notice arrives — these requests have short response windows and missing them can result in denial.
Underpayment Detection in Cardiology
Underpayment detection is particularly valuable in cardiology. Payers apply complex fee schedules to cardiac procedure codes — and occasionally apply the wrong rate, miss an applicable modifier, or calculate a multi-vessel PCI add-on code incorrectly. Reconciling payments against contracted rates for cardiology procedure codes reveals underpayments that, at the fee values involved, represent meaningful recoverable revenue.
Our AR follow-up services include payment reconciliation against cardiology contracted rates — flagging underpayments on high-value cardiology claims before the appeal window closes.
In-House vs. Outsourced Cardiology RCM
| Factor | In-House Billing | Outsourced Cardiology Specialist |
|---|---|---|
| Cardiology CPT Expertise | Requires specialist hire and ongoing education | Built-in across diagnostic and interventional cardiology |
| Prior Authorization Tracking | Manual — high failure risk for high-value procedures | Systematic tracking with procedure-level alerts |
| Global Period Compliance | Manual tracking — errors generate unrecoverable denials | Automated global period flag per patient |
| Modifier 26 and 59 Accuracy | Depends on individual biller knowledge | Pre-submission scrubbing catches every error |
| High-Dollar Claim Follow-Up | Often treated same as low-value claims | Dollar-weighted priority queue |
| Medical Necessity Appeals | Rarely uses guideline citations effectively | ACC/AHA guideline-supported appeals standard |
| Underpayment Detection | Rarely performed on cardiology codes | Quarterly reconciliation against contracted rates |
| Monthly Cost | $5,000–$9,000+ salary + benefits + software | 4–9% of collections |
| Coverage During Staff Absence | High-dollar claims stall | Continuous team-based coverage |
How Qualigenix Supports Cardiology Revenue Cycle Management
At Qualigenix, we bring cardiology-specific billing expertise to every client engagement. Every cardiology onboarding starts with a baseline audit — current denial rates, E&M and procedure code distribution, prior authorization tracking gaps, modifier compliance, and AR aging. We set improvement targets and measure progress monthly.
Our revenue cycle management services for cardiology practices cover the full billing cycle. Eligibility verification with cardiology-specific benefit checks. Procedure-specific coding review by cardiology-trained coders who know the catheterization code family, PCI add-on codes, EP study codes, echocardiography variants, and modifier requirements for every scenario.
We manage prior authorizations for all scheduled cardiology procedures — tracking authorization numbers, expiration dates, authorized CPT codes, and flagging ad hoc PCI scenarios before the claim goes out. Our denial management includes ACC/AHA guideline-supported medical necessity appeals and peer-to-peer review coordination.
For cardiology practices with active catheterization lab programs, our medical billing outsourcing services provide high-volume same-day claim submission with cardiology-specific pre-submission scrubbing. High-dollar claims get priority follow-up. Structural heart procedure claims get individual tracking.
Clients achieve a 99% claim accuracy rate, a 95% first-pass acceptance rate, and a 30% reduction in AR days — with onboarding in as few as 6 days.
Cardiology RCM Checklist
Prior Authorization
- ☐ Authorization confirmed before every scheduled cardiac catheterization, PCI, stress test, echo, and device procedure
- ☐ Authorization tracking log maintained with CPT codes, expiration dates, and procedure dates
- ☐ Ad hoc PCI authorization policy confirmed for each active payer
- ☐ Authorization renewal submitted before expiration for ongoing procedures
Coding and Modifiers
- ☐ Catheterization code selected by reviewing procedure note — not assigned by default
- ☐ Modifier 26 applied on all professional-component-only diagnostic studies
- ☐ Modifier 59 (or XS) applied when diagnostic cath and PCI bill same session
- ☐ Global period flag active for all post-cardiac-surgery patients
- ☐ Global period modifiers (24, 25, 57, 79) applied correctly for excepted services
- ☐ Pre-submission claim scrubbing active with cardiology-specific modifier rules
High-Dollar Claim Management
- ☐ PCI, TAVR, EP ablation, and structural heart claims tracked individually
- ☐ Dollar-weighted AR follow-up — high-value claims followed up at 14 days, not 21
- ☐ AI (additional information) requests responded to within 5 business days
- ☐ Quarterly underpayment audit on top cardiology procedure codes
Denial Management
- ☐ All denials worked within 48 hours of receipt
- ☐ Medical necessity denials appealed with ACC/AHA guideline citations
- ☐ Peer-to-peer review requested on every medical necessity denial
- ☐ Monthly root cause analysis on cardiology denial reason codes
Cardiology Revenue Cycle Management Glossary
Global Period
The post-operative period following a surgical procedure during which routine follow-up care is bundled into the procedure payment. Major cardiac surgical procedures carry a 90-day global period. During this window, billing separately for routine post-operative visits generates unrecoverable denials. Services unrelated to the surgery or meeting specific exceptions you can bill separately with the correct modifier: Modifier 24 (unrelated E&M), Modifier 25 (separately identifiable E&M same day as procedure), Modifier 57 (decision for surgery), or Modifier 79 (unrelated procedure).
Modifier 26 — Professional Component
A CPT modifier indicating that only the physician interpretation and written report of a diagnostic service bills — not the equipment and technical staff (technical component). In cardiology, Modifier 26 applies when a cardiologist interprets a study performed at a facility that separately bills the technical component. Billing without Modifier 26 when appropriate double-bills the technical component and generates payer denials or overpayment recovery requests.
Percutaneous Coronary Intervention (PCI)
A non-surgical cardiac catheterization procedure that opens narrowed or blocked coronary arteries using balloon angioplasty, stent placement, or atherectomy. Billed using CPT codes 92928–92944 depending on vessel(s) treated and technique. PCI procedures require prior authorization from most payers, carry reimbursement values of $1,500 to $2,500 (professional fee) and $8,000 to $20,000 (facility fee), and generate significant revenue losses when denied due to missing authorization or documentation errors.
Modifier 59 — Distinct Procedural Service
A CPT modifier indicating that two or more procedures performed on the same day are distinct and independent — not components of a single bundled service. In cardiology, Modifier 59 (or the X-modifiers XS, XP, XE, XU) prevents payers from bundling a diagnostic catheterization payment into a PCI payment when both happen in the same session. Missing Modifier 59 on combined diagnostic and interventional cardiology cases results in bundling denials that reduce reimbursement by the diagnostic cath value.
Echocardiography (Echo, TTE, TEE)
Ultrasound imaging of the heart evaluating cardiac structure and function. Transthoracic echocardiography (TTE) uses CPT 93306 (with Doppler) or 93307/93308 (without Doppler or limited). Transesophageal echocardiography (TEE) uses CPT 93312–93318. Stress echocardiography uses CPT 93351. Echocardiography billing frequently requires Modifier 26 when a cardiologist interprets a study performed at a hospital or imaging center that separately bills the technical component.
Electrophysiology Study (EP Study)
A specialized cardiac catheterization procedure evaluating the heart’s electrical conduction system. EP studies use CPT codes 93600–93660 depending on specific measurements and interventions. Ablation procedures — including pulmonary vein isolation (CPT 93656) for atrial fibrillation and ventricular tachycardia ablation (CPT 93654) — are among the highest-value cardiology claims. EP procedures require meticulous prior authorization, complex modifier application, and careful add-on code selection.
Technical Component (TC Modifier)
The portion of a diagnostic service representing the equipment, supplies, and technical staff — as distinct from the professional component (physician interpretation). In cardiology, the technical component of echocardiography, nuclear stress testing, and cardiac imaging is typically billed by the facility. When a cardiologist’s practice owns the equipment, they bill the global CPT code (no modifier) and collect both components. When the facility owns the equipment, the cardiologist bills with Modifier 26 (professional component only).
Cardiac Catheterization (Cath, Coronary Angiography)
A diagnostic or interventional procedure inserting a catheter into the heart or coronary arteries to assess cardiac function, measure pressures, or deliver treatment. Diagnostic catheterization uses CPT codes 93451–93461 depending on chambers catheterized and studies performed. Code selection requires careful review of the procedure note — the same session may support multiple code components depending on what was done. Both professional (CMS-1500) and facility (UB-04) fees apply when performed in a hospital catheterization lab.
Frequently Asked Questions: Cardiology Revenue Cycle Management
What is cardiology revenue cycle management?
Cardiology RCM is the specialized billing and collections process for cardiology practices — covering cardiology-specific CPT coding for diagnostic and interventional procedures, prior authorization for high-cost cardiac services, modifier rules, global period compliance, professional vs. facility fee coordination, denial management, and AR follow-up for high-value claims.
Why is cardiology billing more complex than general medical billing?
Three reasons: high-value procedures with complex CPT coding and modifier requirements where a single error costs thousands; extensive prior authorization for cardiac procedures where a missing authorization on a PCI or TAVR can result in a non-appealable denial worth $5,000 to $50,000; and strict 90-day global periods for cardiac surgery where billing errors generate permanent revenue loss that appeals cannot recover.
What are the most commonly billed cardiology CPT codes?
The most common codes include: 93000 (ECG), 93306 (TTE with Doppler), 93458 (left heart cath with coronary angiography), 92928 (PCI single vessel), 93351 (stress echocardiography), 93015/93017/93018 (cardiac stress test), 93620 (complete EP study), and 93656 (EP study with pulmonary vein isolation). Correct selection within each code family requires procedure note review — default coding is a significant error risk in cardiology.
What causes the most denials in cardiology billing?
The top causes are: missing or expired prior authorization (25–35%), medical necessity denials from insufficient documentation (20–30%), modifier errors including missing Modifier 26 and 59 (10–15%), catheterization code selection errors, global period violations, and bundling errors on combined diagnostic and interventional cases. Each is preventable with the right process.
What is Modifier 26 and when is it required in cardiology?
Modifier 26 indicates that only the professional component (physician interpretation and report) of a diagnostic service bills — not the technical component. In cardiology, it applies when a cardiologist interprets a study (echo, nuclear stress test, cardiac CT) performed at a facility that separately bills for the equipment and technical staff. Billing without Modifier 26 when appropriate double-bills the technical component and generates payer denials.
What is the global period in cardiology billing?
The global period is the post-operative window during which routine follow-up care is bundled into the surgical procedure payment. Major cardiac surgical procedures carry a 90-day global period. During that window, billing separately for routine post-operative visits without the correct modifier generates unrecoverable denials. Services unrelated to the surgery you can bill separately using Modifier 24 (unrelated E&M) or Modifier 79 (unrelated procedure).
How does prior authorization work for cardiology procedures?
Cardiology authorization requests require clinical documentation of patient symptoms, cardiac history, prior diagnostic workup results, and a rationale demonstrating medical necessity under the payer’s criteria. High-cost procedures — cardiac catheterization, PCI, stress testing, implantable devices, EP ablations, TAVR — require authorization from most commercial payers and Medicare Advantage plans. Authorization obtain before the procedure, not on the day of service. Missing authorization on a high-value cardiology procedure results in a denial worth thousands to tens of thousands of dollars.
What is the difference between diagnostic and interventional cardiology billing?
Diagnostic cardiology billing covers services that evaluate cardiac function — echocardiography, stress testing, monitoring, ECGs, and diagnostic catheterization. Interventional cardiology billing covers therapeutic procedures — PCI, stent placement, structural heart interventions, EP ablations. Interventional procedures use significantly higher-reimbursing CPT codes, require more extensive prior authorization, have more complex modifier requirements, and generate higher-value denials when errors occur.
Should a cardiology practice outsource revenue cycle management?
For most cardiology practices — especially those with active catheterization lab programs — yes. Cardiology billing requires specialty expertise in high-value procedure codes, modifier rules, global periods, professional vs. facility fee coordination, and prior authorization management that generalist billers consistently get wrong. An outsourced specialist with cardiology billing experience reduces denials, accelerates collections on high-dollar claims, and prevents errors that in-house teams routinely make in this specialty.
How does Qualigenix help cardiology practices with RCM?
Qualigenix provides end-to-end cardiology RCM — eligibility verification, procedure-specific coding review by cardiology-trained coders, prior authorization management with procedure-level tracking, pre-submission claim scrubbing with cardiology modifier rules, denial management with ACC/AHA guideline-supported appeals, dollar-weighted AR follow-up, and monthly KPI reporting. Clients achieve 99% claim accuracy, 95% first-pass acceptance, and 30% reduction in AR days with onboarding in as few as 6 days.
Related Resources
Qualigenix Service Pages:
- Revenue Cycle Management Services
- Medical Billing Outsourcing Services
- Denial Management Services
- AR Follow-Up Services
- Medical Coding Services
- Insurance Eligibility Verification
- Claim Submission Services
Related Blog Guides:
- What Is Revenue Cycle Management? Complete Guide
- Revenue Cycle Management Best Practices
- Medical Billing Outsourcing vs. In-House
- Denial Management Process: Essential Steps
- Accounts Receivable in Medical Billing
- Outsourcing Revenue Cycle Management: How It Works
Cardiology Billing That Matches the Precision of Your Clinical Work
Qualigenix brings cardiology-specific billing expertise to every engagement — from catheterization code selection to global period tracking to ACC/AHA guideline-supported denial appeals.
Our cardiology clients achieve 99% claim accuracy, a 95% first-pass acceptance rate, a 30% reduction in AR days, and an average 36-day collection cycle. We onboard in as few as 6 days.
Precision. Progress. Qualigenix.
What’s Next
Real-time eligibility returned active and the claim still denied: the five reasons why
An “active” eligibility result only proves the policy is in force. It never proves the service is covered, that...
Prior authorization turnaround requirements under the CMS interoperability rule: what changed for practices
The CMS interoperability rule (CMS-0057-F) forces impacted payers to decide standard prior authorizations in 7 calendar days and...
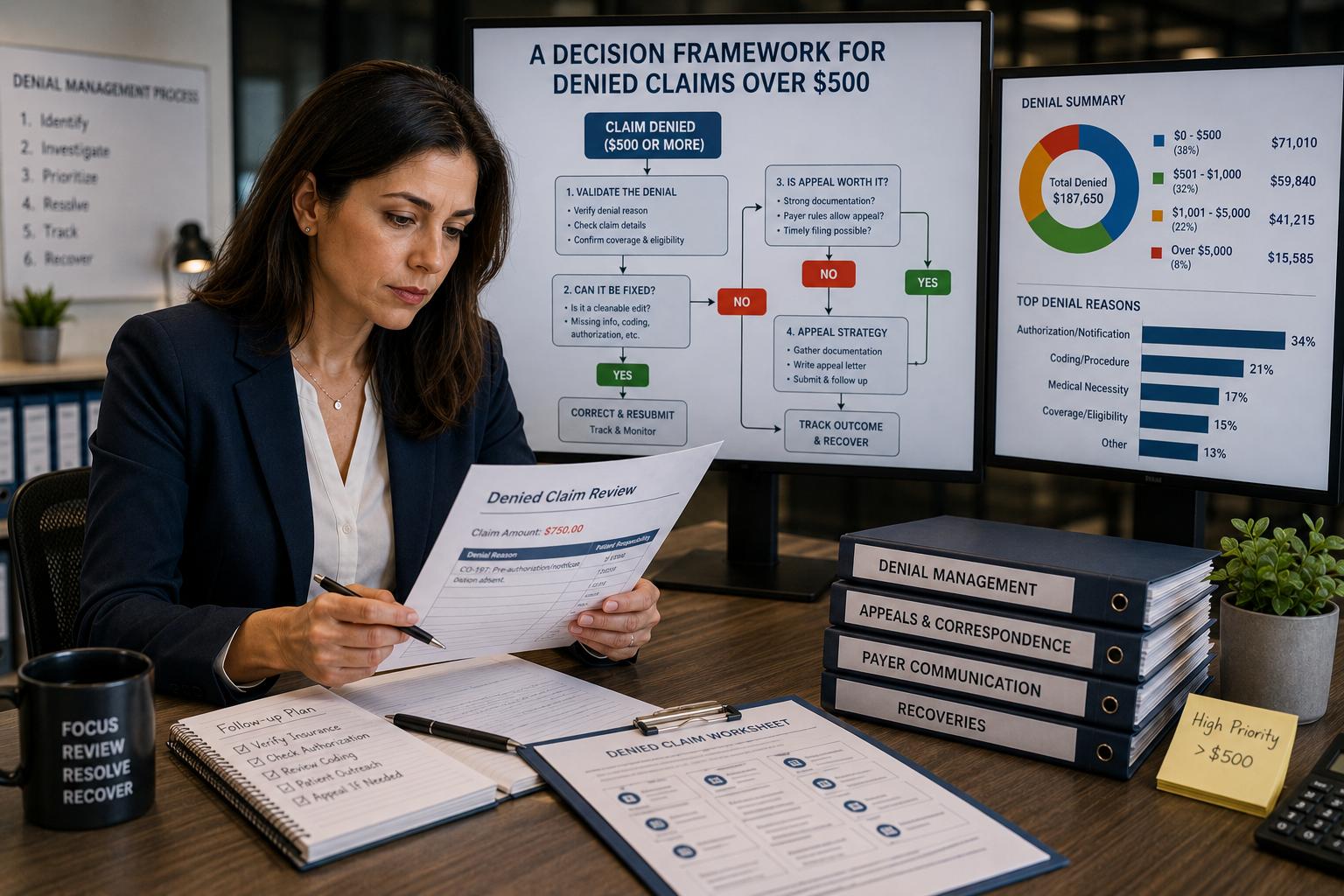
Appeal or Write Off? A Decision Framework for Denied Claims Over $500
Don’t let the dollar amount make the call by itself. Sort the denial by reason code, run the...