Insurance Credentialing for Multi-Provider Practices: What Breaks Down at Scale
The Qualigenix Editorial Team consists of certified billing and coding experts with over 40 years of experience across 38+ medical specialties. Our content is rigorously researched against CMS, AMA, and payer-specific guidelines to ensure total compliance and accuracy. We apply the same elite standards to our resources as we do our client work, consistently delivering high claim accuracy and significant reductions in AR days.
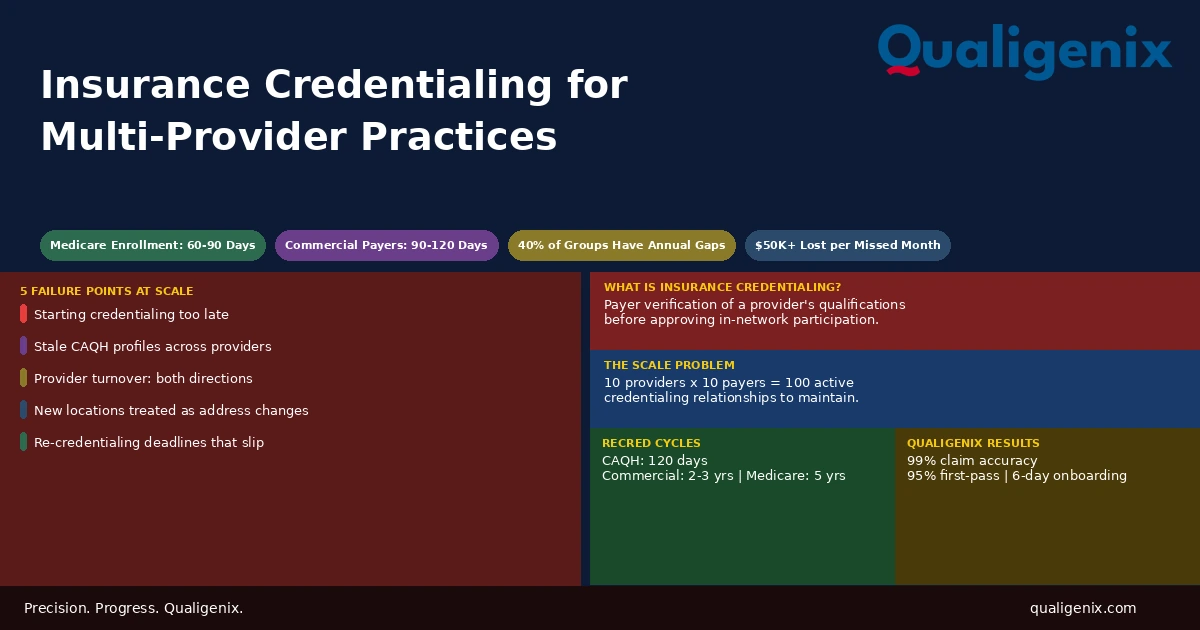
Insurance credentialing is manageable for one or two providers. For practices with five, ten, or twenty providers across multiple locations, it becomes a continuous operational challenge. Credentialing gaps, missed re-credentialing deadlines, stale CAQH profiles, and untracked location updates all cause claim denials that are difficult to trace and expensive to recover. The practices that avoid these problems do so by treating credentialing as an ongoing system, not a one-time task.
A single-provider practice filing for insurance credentialing has a clear task. One provider, one set of documents, one application per payer. The process is tedious, but it’s contained. A group practice adding its eighth provider while two others are up for re-credentialing, a new location just opened, and one payer is requesting updated licensure documentation is managing a completely different problem.
Complexity scales faster than headcount. Each new provider doesn’t just add one credentialing project. It adds a credentialing timeline, a CAQH profile, a set of payer applications, a re-credentialing cycle, and an expiration calendar that runs in parallel with every other provider in the practice. Without a system built to handle that volume, things fall through. And in insurance credentialing, what falls through doesn’t send a warning. It shows up in the denial queue weeks later.
This blog covers exactly where insurance credentialing breaks down in multi-provider settings, what it costs, and what a functional process looks like when a practice grows past what spreadsheets and memory can manage.
Insurance credentialing is the process by which a payer verifies a provider’s qualifications and approves them as a participating in-network provider. In multi-provider practices, credentialing breaks down because each provider has their own timeline, CAQH profile, payer applications, and re-credentialing deadlines running simultaneously. A gap in any one of them causes automatic claim denials for that provider until the gap is corrected.
Insurance Credentialing at Scale: Key Numbers
| Metric | Data Point | Source |
|---|---|---|
| Medicare enrollment average timeline | 60 to 90 days | CMS enrollment data |
| Commercial payer credentialing average timeline | 90 to 120 days | Payer processing benchmarks |
| Maximum credentialing timeline for some payers | Up to 180 days | Credentialing industry surveys |
| Revenue lost per uncompensated provider month | $15,000 to $50,000+ depending on specialty | Practice revenue benchmarks |
| CAQH re-attestation requirement | Every 120 days | CAQH ProView requirements |
| Commercial payer re-credentialing cycle | Every 2 to 3 years | Payer participation agreements |
| Medicare revalidation cycle | Every 5 years for most provider types | CMS revalidation policy |
| Average days between hire and credentialing start in most practices | 14 to 30 days | Credentialing workflow studies |
| Group practices experiencing credentialing gaps annually due to turnover | Estimated 40% | Healthcare operations surveys |
| Payer applications required per provider for a typical group practice panel | 8 to 15 per provider | Multi-payer practice analysis |
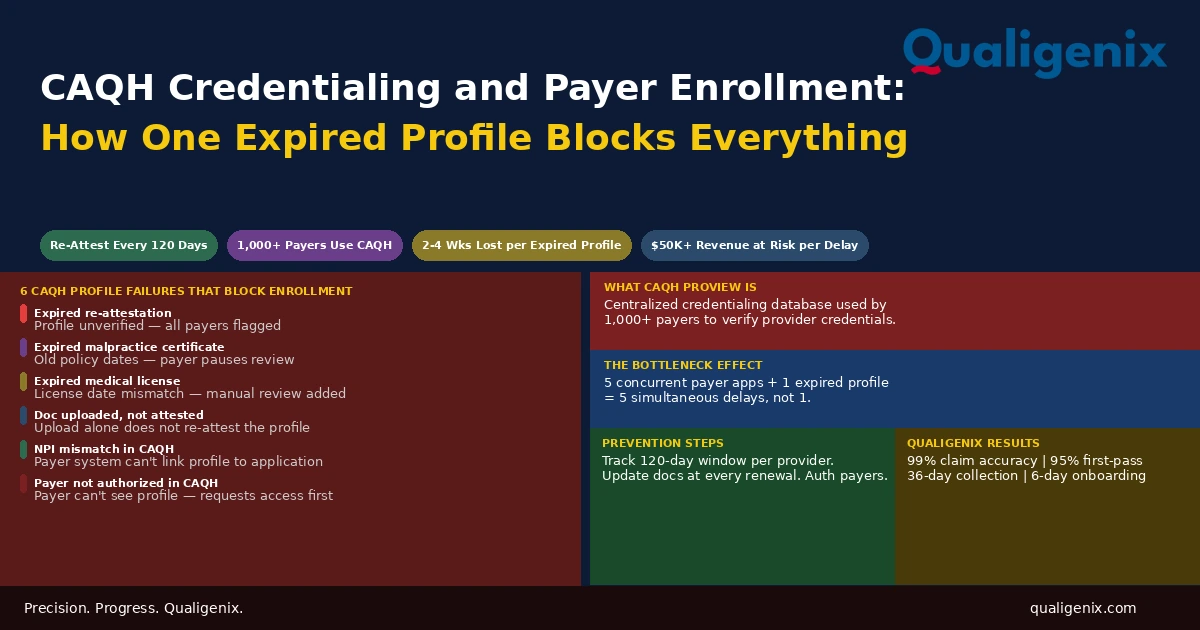
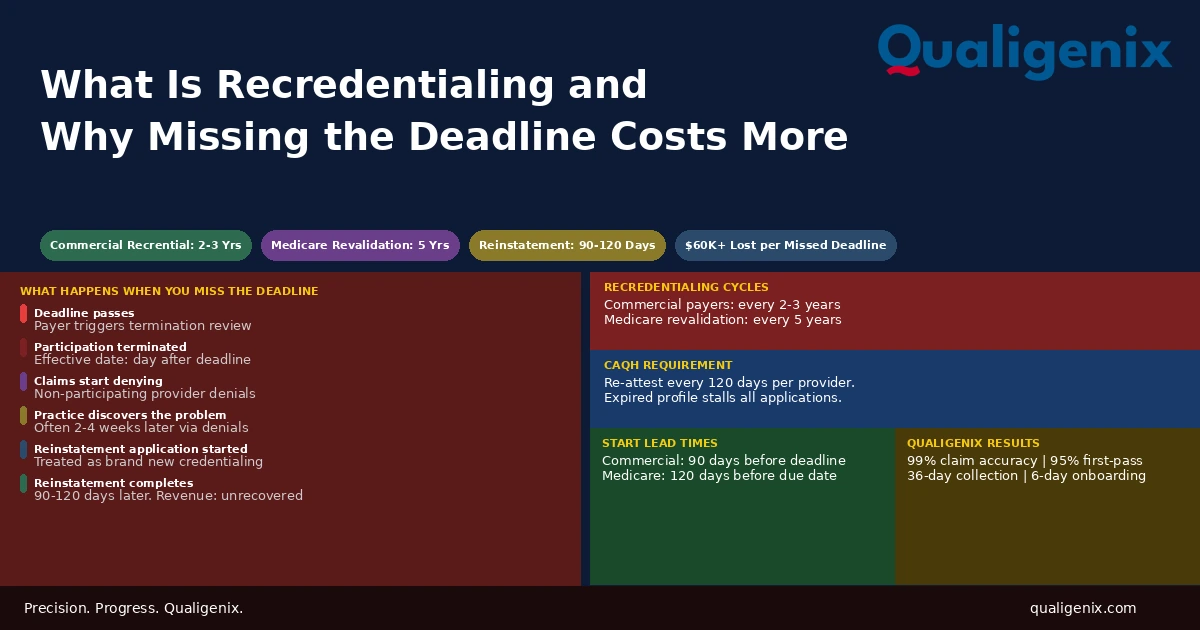
| Qualigenix first-pass acceptance rate | 95% | Qualigenix performance data |
| Qualigenix claim accuracy rate | 99% | Qualigenix performance data |
| Qualigenix average collection cycle | 36 days | Qualigenix performance data |
| Qualigenix client onboarding time | 6 days | Qualigenix operations data |
The Core Problem: Each Provider Is an Independent Credentialing Project
Most practice administrators understand, in theory, that each new provider needs to be credentialed. What’s harder to internalize is that each provider is not just one credentialing event. It’s a continuous credentialing responsibility that runs for the entire duration of that provider’s time at the practice and requires active maintenance across multiple dimensions simultaneously.
A provider joining a 10-provider group needs a CAQH profile built and attested. They need applications submitted to Medicare, Medicaid, and each commercial payer the practice participates with. That’s typically 8 to 15 separate applications. Each payer runs its own review on its own timeline. Each payer may request additional documentation mid-process. Each payer has its own effective date once approved. Until every payer approves the provider, claims billed under that provider to that payer deny automatically.
For a 10-provider practice with 10 active payer contracts, that’s potentially 100 active credentialing relationships that must all be current, accurate, and up for renewal tracking at any given time. A single-person administrative team managing this alongside scheduling, billing, and compliance is almost guaranteed to miss something.
The practices that manage this well don’t rely on memory or spreadsheets. They have a dedicated credentialing system, a clear owner for the function, and a process that starts the moment a provider hire is confirmed, not on the provider’s first day.
Failure Point 1: Starting Credentialing Too Late
The single most common and most costly insurance credentialing failure in multi-provider practices is starting the process too late. A provider accepts an offer in March. The practice plans to start credentialing when the provider arrives in May. By the time the CAQH profile is built, the payer applications are submitted, and the first approvals come back, the provider has been seeing patients for 60 to 90 days without active enrollment on any payer panel.
Those 60 to 90 days of claims deny. Some payers offer retroactive credentialing under narrow circumstances, typically when the provider was already credentialed elsewhere and the new enrollment was in process. Most payers don’t. The practice absorbs the revenue loss for every patient that provider saw before their credentialing was active.
For a hospitalist or a surgeon, two months of uncompensated patient encounters can represent $30,000 to $80,000 in lost revenue. For a primary care physician, the number is lower but still significant. For a multi-provider practice adding three new providers in the same quarter, the cumulative impact of three credentialing delays running simultaneously is a material financial event.
Warning: The fix is simple in theory and consistently ignored in practice: start credentialing the day an offer is accepted, not the day the provider walks in the door. Medicare enrollment alone takes 60 to 90 days. If the provider’s start date and the enrollment start date are the same, there will be a billing gap. It is not a risk. It is a certainty.
Failure Point 2: CAQH Profiles That Don’t Stay Current
CAQH ProView is the centralized credentialing database most commercial payers use during the insurance credentialing review process. A provider builds a CAQH profile with their education, training, licensure, board certifications, malpractice history, and work history. Payers query that profile instead of requesting the same documents repeatedly through separate applications. In theory, it reduces paperwork significantly. In practice, it only works if the profile stays accurate and current.
CAQH requires providers to re-attest their profile every 120 days. If a provider doesn’t re-attest within that window, the profile expires. An expired CAQH profile stalls every credentialing application that depends on it. Payers checking the profile mid-review find incomplete or outdated data and flag the application for follow-up, which adds weeks to the timeline.
In a single-provider practice, one re-attestation reminder is manageable. In a 15-provider practice, re-attestation deadlines for 15 providers are staggered throughout the year. Provider A’s 120-day window expires in February. Provider B’s expires in April. Provider C’s expires in May. Tracking all of them, sending reminders to individual providers who are busy seeing patients, and confirming the re-attestation was completed before the deadline is an ongoing administrative process, not a one-time task.
What Stale CAQH Profiles Cost
When a CAQH profile expires or contains outdated information, the cost isn’t always visible immediately. The damage shows up when a re-credentialing review is triggered and the payer finds the profile data doesn’t match current records. The re-credentialing process stalls. The provider’s participation status lapses while the review is held up. Claims start denying. Billing staff investigate the denial pattern and eventually trace it back to a CAQH profile issue that no one flagged because no one was tracking it.
Related: CAQH Profile Management Services
Failure Point 3: Provider Turnover and the Double Problem It Creates
Provider turnover is a credentialing event that works in two directions simultaneously, and most practices only manage one of them.
When a provider leaves, their credentialing must be terminated across every payer panel. This is not optional and not automatic. A provider who resigns from a practice but whose name remains on active payer enrollments creates compliance exposure. Claims submitted under a provider no longer practicing at the group are a payer audit trigger. In states that require prompt notification of provider departures to payers, failing to terminate enrollment is a regulatory issue as well as a compliance one.
At the same time, the incoming replacement provider needs a full credentialing process started immediately. In most practices, the termination step gets handled (eventually) but the incoming credentialing process starts late because the practice is still managing the transition and credentialing feels like something that can wait a few weeks. Those few weeks become a billing gap that starts the moment the new provider sees their first patient.
Every provider departure should trigger two simultaneous actions: immediate initiation of payer termination across all active enrollments, and immediate initiation of the replacement provider’s credentialing process. In multi-provider practices that experience two or three provider changes per year, these two actions need to happen as automatic protocol, not case-by-case decisions.
Failure Point 4: New Locations Treated as Address Updates
When a group practice opens a second or third location, the credentialing implications are frequently underestimated. The instinct is to notify payers of a new address and assume the update is processed quickly. That assumption is wrong, and it’s expensive.
Many payers treat a new practice location as a new enrollment application. The new location has its own address, its own Type II NPI in many cases, and its own place-of-service information that must be verified before claims from that location can be paid. Some payers require a separate participation agreement for the new location. Others process it as a modification to the existing group record. The payer’s treatment of the situation determines the timeline, and that timeline can run from two weeks to four months depending on the payer.
Claims submitted from a new location before the payer’s records reflect that location deny. They may deny on place-of-service grounds. They may deny because the group NPI isn’t associated with the new address. They may route to an incorrect fee schedule. All of these outcomes require rework, and all of them are avoidable if the location expansion is treated as a credentialing and enrollment project from the start.
The Multi-Location Payer Update Process
When adding a new location, every active payer contract must be reviewed and updated. This means contacting each payer’s provider relations team, submitting the location update through the payer’s required channel (some use online portals, some require paper forms, some require a direct phone call with a follow-up letter), and tracking each update through to confirmed status.
For a group with 12 active payer contracts opening a second location, that’s 12 separate update processes running simultaneously, each with its own confirmation timeline. Without a tracker, the practice has no way to know which payers have updated their records and which haven’t. Claims from the new location will deny silently until billing staff notice the pattern.
Failure Point 5: Re-credentialing Deadlines That Slip
Insurance credentialing is not permanent. Commercial payers require re-credentialing every two to three years. Medicare requires revalidation every five years for most provider types. Each deadline requires the provider to resubmit updated documentation, complete a new participation review, and in some cases sign a new participation agreement.
Missing a re-credentialing deadline doesn’t just delay the renewal. Many payers terminate a provider’s participation status when the re-credentialing deadline passes without a completed renewal. Termination means the provider is no longer in network. Claims submitted after the termination date deny as out-of-network or non-participating provider, and patients may receive unexpected balance bills.
In a 10-provider practice, re-credentialing deadlines are distributed across a two to three year cycle. In any given month, one or two providers may have an upcoming renewal. Without a system that flags these 90 days in advance, the first sign of a missed deadline is often a denial notice or a payer letter notifying the practice of terminated participation status.
| Credentialing Event | Required Timeline | Consequence if Missed | Lead Time Needed |
|---|---|---|---|
| New provider Medicare enrollment | 60 to 90 days to complete | Claims deny, uncompensated care | Start on hire confirmation |
| Commercial payer credentialing | 90 to 120 days to complete | Claims deny until approval | Start on hire confirmation |
| CAQH re-attestation | Every 120 days | Profile expires, applications stall | 30 days before deadline |
| Commercial payer re-credentialing | Every 2 to 3 years | Participation terminated | 90 days before deadline |
| Medicare revalidation | Every 5 years | Billing privileges deactivated | 90 days before deadline |
| New location payer update | 2 weeks to 4 months per payer | Claims from new location deny | Start before location opens |
| Provider departure termination | Varies by payer, typically 30 days | Compliance exposure, audit risk | Initiate on departure notice |
The Credentialing Tracker Every Multi-Provider Practice Needs
None of the failure points described above are complicated to prevent. They’re all traceable to the same root cause: no one had a system that flagged the upcoming event in time to act on it. The solution is a credentialing tracker that functions as a live operational document, not a one-time checklist.
A functional credentialing tracker covers every active provider in the practice and records the following for each payer relationship: application date, approval date, effective date, re-credentialing due date, and current status. It also tracks each provider’s CAQH re-attestation deadline, their license expiration dates, their DEA and state permit expirations, and their malpractice certificate renewal dates. Any of these credentials expiring triggers a payer to put the enrollment on hold or terminate participation.
The tracker needs an owner. In multi-provider practices, credentialing tracking assigned as a secondary responsibility to a billing or administrative staff member who also manages other functions will consistently get deprioritized. The complexity of managing 10 or more providers across 10 or more payer contracts requires either a dedicated credentialing coordinator or a credentialing management partner.
What Group Practice Enrollment Requires Beyond Individual Credentialing
Insurance credentialing in a group practice has an additional layer that solo practitioners don’t deal with: the group itself must be enrolled with each payer in addition to individual providers. Group practice enrollment links the group NPI and Tax ID to the payer’s billing system so claims submitted under the group entity can be processed correctly.
Individual providers render services and are identified as rendering providers on claims. The group bills and receives payment as the billing entity. Both relationships must be active and correctly linked for claims to process without error. When a new provider joins a group, they must be credentialed individually and linked to the group enrollment. When a provider leaves, they must be removed from both the individual enrollment and the group linkage.
This dual-layer structure is one of the most common sources of confusion in group practice billing. A provider who is individually credentialed with a payer but not linked to the group NPI will produce claims that deny because the billing entity and the rendering provider aren’t recognized as related by the payer’s system. The fix requires a direct enrollment update, which takes time and delays payment further.
How Qualigenix Manages Insurance Credentialing for Multi-Provider Practices
At Qualigenix, we manage insurance credentialing for practices across 38+ specialties, from solo practitioners to multi-location group practices with dozens of active providers. Our credentialing team handles every stage of the process: CAQH profile build and ongoing maintenance, primary source verification, payer application submission and follow-up, re-credentialing renewals, and provider departure terminations.
We maintain a live credentialing tracker for every client with all active provider enrollments, re-credentialing deadlines, CAQH attestation windows, and license expiration dates. When a deadline approaches, we initiate the renewal process. We don’t wait for a payer to notify you that participation is lapsing. We prevent the lapse from happening.
When a new provider joins a practice, we start the credentialing process the day we’re notified of the hire. For Medicare, that means submitting the PECOS enrollment immediately. For commercial payers, it means building the CAQH profile and submitting applications in priority order by patient volume. Our goal is to close the gap between a provider’s first day and their first billable date as quickly as possible.
Our performance reflects this approach: a 99% claim accuracy rate, a 95% first-pass acceptance rate, and an average 36-day collection cycle. We onboard new clients in as few as 6 days. If your practice is managing credentialing across multiple providers and starting to see the gaps, we’re built to handle exactly this situation.
Related services: Provider Credentialing | Payer Enrollment | CAQH Profile Management | Re-credentialing Services
Insurance Credentialing Checklist for Multi-Provider Practices
- Credentialing process started for every new hire on the day an offer is accepted
- CAQH ProView profile built and completed before any payer applications are submitted
- CAQH re-attestation tracked per provider with alerts set 30 days before 120-day deadline
- Payer applications submitted in priority order by patient volume and payer type
- Central credentialing tracker maintained with all active enrollments and renewal dates
- Re-credentialing renewal process started 90 days before each payer deadline
- Medicare revalidation due dates tracked in PECOS for every provider
- Provider departures trigger immediate payer termination notifications
- New location payer updates treated as enrollment projects starting before opening day
- Group NPI linkage verified for every provider at every payer after any enrollment change
Frequently Asked Questions: Insurance Credentialing
What is insurance credentialing?
Insurance credentialing is the process by which a payer verifies a provider’s education, training, licensure, malpractice history, and board certifications before approving them as a participating in-network provider. Until credentialing is complete and enrollment is active, a provider cannot bill that payer. Claims submitted before the effective date deny automatically with no appeal path for most payers.
How long does insurance credentialing take for a new provider?
Medicare enrollment averages 60 to 90 days. Commercial payer credentialing averages 90 to 120 days, with some payers taking up to 180 days for new participating provider applications. Delays from incomplete applications, missing documents, or expired CAQH profiles extend these timelines further. This is why starting credentialing on the day a hire is confirmed, not on the provider’s start date, is the single most important timing decision a practice can make.
What breaks down in insurance credentialing when a practice has multiple providers?
With multiple providers, credentialing breaks down because each provider has their own applications, CAQH profile, enrollment timelines, and re-credentialing deadlines running in parallel with no centralized tracking. Providers start seeing patients before enrollment completes. CAQH profiles expire unnoticed. Re-credentialing deadlines pass without renewal. Location additions don’t get reflected across all payer records. The larger the provider count, the more likely one of these gaps causes a billing disruption at any given time.
What is CAQH and why does it matter for insurance credentialing?
CAQH ProView is a centralized database where providers store their credentialing data for participating payers to query during the application review process. A stale, incomplete, or expired CAQH profile delays every credentialing application that relies on it. CAQH requires re-attestation every 120 days. In multi-provider practices, multiple providers have staggered attestation windows throughout the year, all of which require active tracking and follow-through.
What happens if a provider sees patients before insurance credentialing is complete?
Claims submitted under a provider before their credentialing effective date deny automatically. Most payers do not allow retroactive billing for services delivered before the credentialing approval date. The practice delivers the care and absorbs the full revenue loss for that period. For a high-volume provider, two months of uncompensated encounters can represent $30,000 to $80,000 depending on specialty and patient volume.
How does provider turnover affect insurance credentialing in a group practice?
Provider turnover creates two simultaneous credentialing obligations: terminating the departing provider from all active payer panels and starting the incoming provider’s credentialing immediately. Both must happen in parallel. Failing to terminate a departing provider creates compliance exposure. Starting the incoming provider’s credentialing late creates a billing gap. Most practices handle one and delay the other, which means they’re always exposed on at least one side of every transition.
What is re-credentialing and how often is it required?
Re-credentialing is the periodic renewal of a provider’s participation status with a payer. Commercial payers typically require it every two to three years. Medicare requires revalidation every five years. Missing a re-credentialing deadline can result in terminated participation status, which causes all claims submitted after the termination date to deny as non-participating. The only way to prevent this in a multi-provider practice is a calendar system that flags renewals 90 days in advance.
Does insurance credentialing need to be done separately for each payer?
Yes. Each payer has its own credentialing application and participation agreement. Being credentialed with one payer does not extend to any other. CAQH reduces duplication by giving payers shared access to a provider’s profile data, but the participation application and contract must still be completed with each payer individually. A 10-provider practice with 10 payer contracts has up to 100 active credentialing relationships to maintain.
How does adding a new location affect insurance credentialing for existing providers?
Adding a new location requires updating payer enrollment records with the new address, NPI, and Tax ID across every active payer contract. Many payers treat a new location as a new enrollment application with a timeline of two weeks to four months. Claims submitted from a new location before payer records reflect it will deny. Location expansion must be treated as an enrollment project starting before the new location sees its first patient.
Should a multi-provider practice outsource insurance credentialing?
Most multi-provider practices benefit from outsourcing insurance credentialing because the volume of applications, CAQH updates, re-credentialing renewals, and location changes exceeds what in-house administrative staff can manage accurately alongside other responsibilities. A credentialing partner maintains a live tracker across all providers and payers, flags upcoming deadlines, starts new provider applications immediately on hire, and handles terminations without any step falling through.
Related Resources from Qualigenix
Growing Practice. Growing Credentialing Complexity. We Handle Both.
Qualigenix manages insurance credentialing across every provider, every payer, and every location in your practice. We start new enrollments the day a hire is confirmed, track every re-credentialing deadline, and maintain CAQH profiles so nothing expires quietly in the background.
Our team delivers 99% claim accuracy, a 95% first-pass acceptance rate, an average 36-day collection cycle, and a 30% reduction in AR days. We onboard in as few as 6 days.
Precision. Progress. Qualigenix.
What’s Next

Vendor Credentialing Management for Healthcare Organizations: Keeping Compliance Current Across Every Vendor
Vendor credentialing is the process by which healthcare facilities verify that vendors, sales representatives, and third-party service providers meet...
CAQH Credentialing and Payer Enrollment: How One Expired Profile Blocks Every Application Behind It
CAQH credentialing is the process of building and maintaining a provider’s profile in the CAQH ProView database, which...
What Is Recredentialing and Why Missing the Deadline Costs More Than the Renewal
Recredentialing is the periodic renewal every provider must complete to stay on a payer’s network. Most commercial payers require...