What Is Recredentialing and Why Missing the Deadline Costs More Than the Renewal
The Qualigenix Editorial Team consists of certified billing and coding experts with over 40 years of experience across 38+ medical specialties. Our content is rigorously researched against CMS, AMA, and payer-specific guidelines to ensure total compliance and accuracy. We apply the same elite standards to our resources as we do our client work, consistently delivering high claim accuracy and significant reductions in AR days.
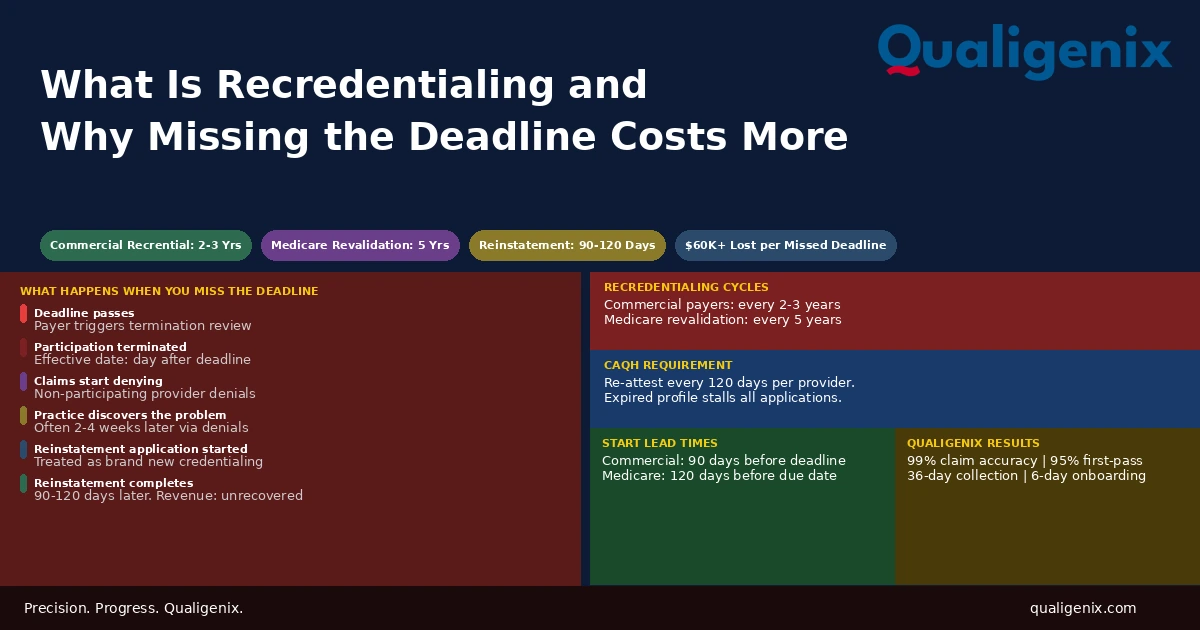
Recredentialing is the periodic renewal every provider must complete to stay on a payer’s network. Most commercial payers require it every two to three years. Medicare requires revalidation every five years. Missing a deadline doesn’t pause things while you catch up. It terminates your participation, stops payments, and forces you through a full reinstatement process that takes 90 to 120 days. The renewal takes two weeks of administrative effort. The missed deadline costs months of revenue.
Most practices know credentialing happens when a new provider joins. Fewer have a reliable system for what happens after that. Recredentialing is the part of the credentialing lifecycle that runs on a cycle, quietly accumulating toward a deadline that most practices don’t see coming until a payer terminates participation and claims start denying.
The renewal itself is not complicated. Gather updated documents, verify the CAQH profile, submit the application, follow up, confirm approval. Done in two to three weeks of focused administrative work if started on time. The problem is starting on time requires knowing the deadline exists, knowing exactly when it falls, and having the capacity to act on it 90 days in advance. Most practices with more than three providers don’t have a system that reliably does all three.
This blog explains what recredentialing is, what each payer requires and when, and what a missed deadline actually costs in terms of revenue, reinstatement time, and patient impact.
Recredentialing is the periodic process through which a payer re-verifies a provider’s qualifications, licensure, malpractice history, and board certifications to confirm they still meet network participation standards. Most commercial payers require it every two to three years. Missing a recredentialing deadline results in terminated participation status, automatic claim denials, and a reinstatement process that takes 90 to 120 days with no retroactive revenue recovery.
Recredentialing: Key Numbers Every Practice Needs to Know
| Metric | Data Point | Source |
|---|---|---|
| Commercial payer recredentialing cycle | Every 2 to 3 years | Payer participation agreements |
| Medicare revalidation cycle | Every 5 years for most provider types | CMS revalidation policy |
| CAQH re-attestation requirement | Every 120 days | CAQH ProView requirements |
| Recredentialing processing time | 60 to 120 days depending on payer | Credentialing industry benchmarks |
| Reinstatement timeline after missed deadline | 90 to 120 days as new application | Payer credentialing policies |
| Revenue lost per payer per month during reinstatement | $10,000 to $60,000+ depending on specialty | Practice revenue benchmarks |
| Recommended start lead time (commercial) | 90 days before deadline | Credentialing best practices |
| Recommended start lead time (Medicare revalidation) | 120 days before deadline | CMS revalidation guidance |
| Multi-provider practices missing at least one deadline annually | Estimated 30% | Healthcare operations surveys |
| Qualigenix first-pass acceptance rate | 95% | Qualigenix performance data |
| Qualigenix claim accuracy rate | 99% | Qualigenix performance data |
| Qualigenix average collection cycle | 36 days | Qualigenix performance data |
| Qualigenix client onboarding time | 6 days | Qualigenix operations data |
What Recredentialing Actually Is
When a provider initially joins a payer’s network, the payer conducts a credentialing review. It verifies education, training, licensure, board certifications, malpractice history, and whether any adverse actions have been taken against the provider’s license. If the provider meets the payer’s standards, they’re approved as a participating provider and can bill the payer for in-network services.
That approval is not permanent. Payers require periodic re-verification to confirm that a provider’s credentials are still current, their malpractice coverage is still active, their license hasn’t been restricted or revoked, and their scope of practice still aligns with what they’re billing for. This periodic re-verification is recredentialing.
It isn’t a punishment or an investigation. It’s a routine administrative process that every provider on every payer panel faces at regular intervals throughout their career. The cycle varies by payer, but the core function is the same: the payer checks that the provider still meets the standards they approved initially and renews the participation agreement for another term.
The critical distinction between credentialing and recredentialing is timing. Initial credentialing happens once when a provider joins the network. Recredentialing happens repeatedly, on a fixed schedule set by each payer, for the entire duration of the provider’s participation. A practice that manages initial credentialing well but has no system for recredentialing will eventually face a termination notice it didn’t see coming.
Who Requires Recredentialing and How Often
Every commercial payer that credentialed a provider will require recredentialing at their own interval. There is no universal standard. Each payer sets its own cycle, typically written into the participating provider agreement. The most common commercial payer cycle is every two to three years. Some payers notify providers well in advance. Others send a single notice 60 to 90 days before the deadline. A few notify later than that.
Medicare operates differently. CMS doesn’t call it recredentialing. It’s called revalidation, and it happens every five years for most provider types through the Provider Enrollment, Chain, and Ownership System, known as PECOS. CMS notifies providers by mail and through their PECOS account when revalidation is due. Missing the revalidation deadline triggers a different consequence than commercial payer recredentialing, which is covered in detail later in this blog.
Medicaid revalidation cycles vary by state. Most state Medicaid programs align with CMS standards and require revalidation every five years, but state-specific variations exist. Providers enrolled in multiple state Medicaid programs may face staggered revalidation deadlines across different state programs.
| Payer Type | Recredentialing Cycle | Process | Consequence if Missed |
|---|---|---|---|
| Commercial payers | Every 2 to 3 years | Payer application, CAQH query | Network termination |
| Medicare (CMS) | Every 5 years | PECOS revalidation submission | Billing privileges deactivated |
| Medicaid (state) | Every 5 years (varies by state) | State-specific portal or paper | Medicaid billing suspended |
| CAQH ProView | Every 120 days (re-attestation) | Online re-attestation by provider | Profile expires; slows all credentialing applications |
| Medicare Advantage plans | Every 2 to 3 years (varies by plan) | Plan-specific application | Network termination for that plan |
| Hospital privileges | Every 2 years (most hospitals) | Medical staff office process | Privileges suspended |
What the Recredentialing Process Involves
The recredentialing process is structurally similar to initial credentialing but faster to complete because the provider is already in the system. The payer re-verifies the key credential components rather than building a new record from scratch.
Step 1: Document Verification
The provider must provide current versions of their medical license, DEA registration, malpractice insurance certificate with current policy dates and coverage limits, board certification documentation, and NPI confirmation. Any of these that have expired since the last credentialing cycle must be renewed before the recredentialing application can be processed. A medical license that expired two months ago will halt a recredentialing review regardless of how complete the rest of the application is.
Step 2: CAQH Profile Update and Re-attestation
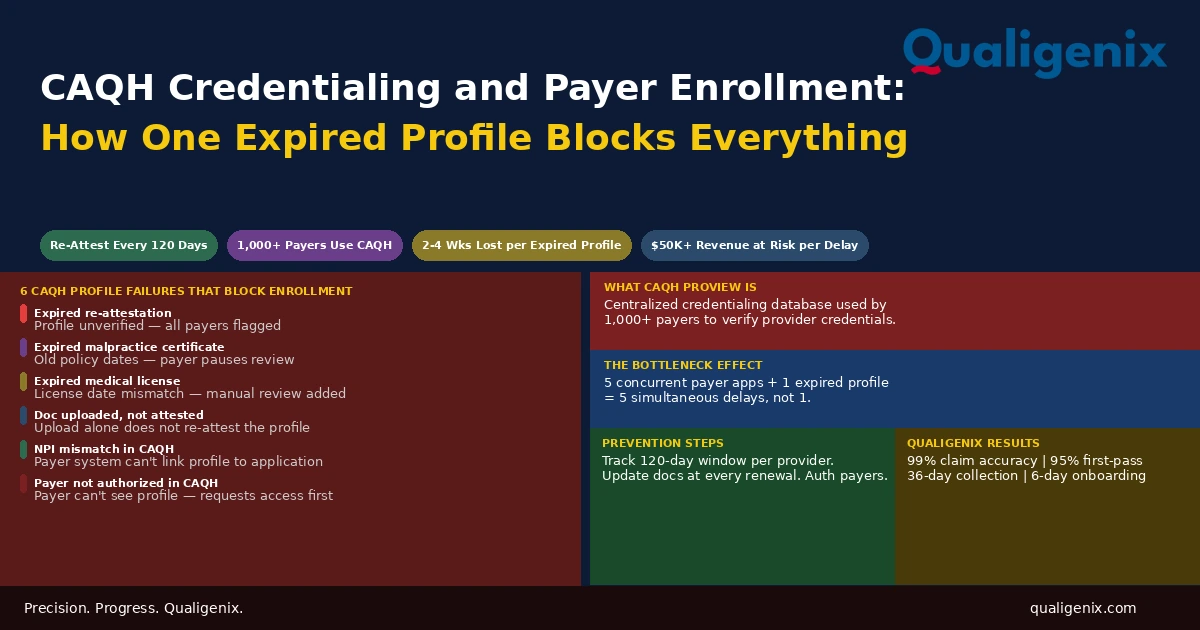
Most commercial payers query CAQH ProView during recredentialing review. Before submitting any recredentialing application, the provider’s CAQH profile must be current, fully attested, and accurately reflect the provider’s current practice information. An expired CAQH profile delays every payer application that depends on it. Providers who haven’t re-attested their CAQH profile in more than 120 days will have an expired status that flags immediately during payer review.
Warning: A common recredentialing failure isn’t a missed payer deadline. It’s a CAQH profile that expired quietly in the background. The provider’s payer deadline is 60 days away. The team submits the application. The payer queries CAQH, finds an outdated profile, and flags the application for follow-up. The follow-up takes three weeks. The payer deadline passes before the application is complete. Participation lapses. The CAQH expiration, not the missed deadline, was the root cause.
Step 3: Attestation of Changes
The provider must attest whether anything material has changed since the last credentialing cycle: new malpractice claims or settlements, any restriction or sanction on their license, changes in hospital privileges, any criminal history changes, and whether they are currently under investigation by any regulatory body. Payers use this attestation to assess whether any change in the provider’s background warrants additional review before renewing participation.
Step 4: Application Submission and Follow-Up
The completed application goes to the payer through their preferred channel, either a provider portal, a paper form, or through a credentialing service. After submission, the practice must track the application status actively. Payers may issue requests for additional information mid-review. Applications that don’t receive a timely response to these requests stall in queue and miss the deadline while the practice doesn’t know the application is on hold.
Following up with the payer’s provider relations team every two weeks is standard practice for any recredentialing application within 90 days of a deadline. Passive waiting is the approach that turns a 60-day review into a 120-day review that runs past the participation expiration date.
What Actually Happens When a Recredentialing Deadline Is Missed
This is the part most practices don’t understand until it happens to them. Missing a recredentialing deadline doesn’t put the provider’s participation on hold while the renewal catches up. It terminates participation. The distinction matters enormously for billing.
Termination and What It Triggers
When a provider’s recredentialing deadline passes without an approved renewal, the payer terminates their network participation. This termination has an effective date, often the day after the deadline. From that date forward, the provider is no longer a participating in-network provider for that payer. Every claim submitted to that payer after the termination effective date denies as a non-participating provider service.
Patients whose insurance requires in-network providers for coverage will receive those denials. In plans where out-of-network services carry high cost sharing or no coverage at all, patients may face unexpected bills for services they believed were covered. This is a patient trust issue on top of a revenue issue, and it happens not because of any clinical problem but because of an administrative deadline that was missed.
Payers are not required to notify providers that their termination effective date has arrived. Many practices discover a missed recredentialing deadline only when billing staff notice a denial pattern for a specific payer and trace it back to a termination notice that was sent weeks earlier and never actioned. By the time billing staff identify the problem, several weeks of claims may already be unrecoverable.
The Reinstatement Process
Getting back onto a payer panel after a termination due to missed recredentialing is not a simple correction. Most payers treat reinstatement as a brand new credentialing application. The provider goes back through the full initial credentialing process: new application, primary source verification, payer committee review, and a new participating provider agreement. That process takes 90 to 120 days.
During those 90 to 120 days, every claim for that payer continues to deny. There is no grace period. There is no retroactive billing for the reinstatement window. The revenue lost during the gap is gone. A practice whose highest-volume commercial payer terminates a physician’s participation will see a sharp and immediate drop in collections from that payer that continues for three to four months while reinstatement processes.
For a primary care physician who sees 20 patients per day and whose largest commercial payer represents 35% of their patient volume, a 90-day reinstatement gap can mean $25,000 to $50,000 in unrecoverable lost revenue. For a specialist with higher per-visit reimbursement rates, the number is larger. None of it is recoverable once the reinstatement completes. The payer won’t pay retroactively for the gap period.
Medicare Revalidation: How It Differs and What the Stakes Are
Medicare revalidation operates under different rules than commercial recredentialing, and the consequences of missing it are different in important ways.
CMS notifies providers of their revalidation due date through the PECOS system and by mail to the address on file in their enrollment record. If the address on file is outdated, the provider may never receive the notice. This is one of the most common reasons Medicare revalidation deadlines are missed: the CMS notice went to an old office address or a former billing contact and was never forwarded.
When Medicare revalidation is not completed by the due date, CMS deactivates the provider’s Medicare billing privileges. Deactivation means Medicare will not pay claims submitted under that provider’s NPI after the deactivation date. Unlike commercial payer termination, Medicare deactivation doesn’t require a 90-day reinstatement process. Billing privileges can be restored faster once revalidation is completed and processed. But the gap period still produces denials, and those denied claims are not retroactively paid once billing privileges are restored.
Warning: CMS sends revalidation notices to the address on file in PECOS, not to whatever address is in your practice management system or your billing software. Practices that moved locations or changed their billing contact and didn’t update PECOS will not receive their revalidation notice. Checking the revalidation due date directly in PECOS at least once per year for every enrolled provider is the only way to catch this before the deadline arrives unannounced.
Medicare also conducts off-cycle revalidation for providers flagged for additional review, including providers with billing anomalies or those who received revalidation notices and didn’t respond. These off-cycle reviews are initiated by CMS without advance provider notification and can result in accelerated deactivation timelines.
The Hidden Cost: What a Missed Deadline Actually Adds Up To
The administrative cost of completing a recredentialing renewal on time is modest. Two to three hours of document gathering. A CAQH profile check. Application submission and follow-up calls over a 60-day period. For most practices, this is a manageable task if it’s planned.
The cost of missing the deadline is not modest. It has four components, and all four begin accumulating the day participation terminates.
The first is direct revenue loss. Every claim that would have been paid as an in-network service now denies. For a busy practice, this happens across every patient encounter with that payer for every day of the gap. The daily revenue loss from a single payer termination can run hundreds to thousands of dollars depending on patient volume and payer mix.
The second is staff cost for reinstatement. Someone has to assemble a full new credentialing application, submit it, follow up on it over 90 to 120 days, and track it through to approval. This is time taken away from other administrative functions.
The third is patient impact. Patients who receive bills for services they believed were covered in-network will be upset. Some will dispute charges. Some will find another in-network provider and not return. Patient attrition from a participation termination is difficult to measure but represents future revenue loss beyond the reinstatement window.
The fourth is denial management cost. Every denied claim from the gap period must be reviewed, patient-billed, or written off. Billing staff who are already managing the denial queue must now handle the added volume of termination-related denials, each of which requires individual attention.
| Cost Component | Description | Recoverable? |
|---|---|---|
| Direct revenue loss during gap | Claims denied as non-participating for full reinstatement window | No |
| Staff time on reinstatement application | Full new credentialing application over 90-120 days | No |
| Patient balance billing disputes | Patients billed unexpectedly for in-network services they received | Partial |
| Patient attrition | Patients who switch to other in-network providers during the gap | Rarely |
| Denial management staff cost | Additional billing staff time reviewing and working gap-period denials | No |
| Cost of timely recredentialing renewal | Document gathering, CAQH update, application submission, follow-up | N/A — preventive cost |
The CAQH Connection: Why Profile Maintenance Is Part of Recredentialing
CAQH ProView is the centralized database most commercial payers use during recredentialing review. The provider stores their credentialing data in CAQH, and payers query the database rather than collecting the same documents through separate paper applications. It’s a significant efficiency gain for both providers and payers when the CAQH profile is current.
The critical requirement is the 120-day re-attestation. Every 120 days, the provider must log into CAQH, review their profile for accuracy, and re-attest that the information is current. If this doesn’t happen, the profile expires. An expired CAQH profile is flagged by payers during any credentialing review, including recredentialing. The payer will request updated documentation, which adds two to four weeks to the processing timeline.
For practices with multiple providers, CAQH re-attestation deadlines are staggered across the year. One provider’s 120-day window may fall in February, another’s in May, another’s in August. Without a calendar that tracks each provider’s re-attestation due date and sends reminders in advance, some will expire unnoticed. The first time the practice discovers an expired profile is often when a recredentialing application stalls mid-review.
Related: CAQH Profile Management Services
How to Build a Recredentialing System That Doesn’t Miss Deadlines
The practices that never miss recredentialing deadlines share one thing: they treat recredentialing as a scheduled operational function, not an occasional administrative task. Here’s what that looks like in practice.
A Live Credentialing Renewal Calendar
Every active provider in the practice needs a renewal record that lists each payer they are credentialed with, the initial approval date, the recredentialing deadline, the date the renewal process must start (90 days before the deadline), and the current status of any renewal in progress. This calendar is reviewed monthly. Any deadline within the next 90 days triggers immediate action.
CAQH Re-attestation Tracking
Alongside payer deadlines, the calendar tracks each provider’s CAQH re-attestation date, which resets every 120 days from the last attestation. Reminders go out at 30 days before each expiration. Re-attestation takes 10 minutes and preventing it from expiring costs nothing. Recovering from an expired CAQH that delayed a recredentialing application costs weeks of processing time.
Proactive Document Expiration Monitoring
Medical licenses, DEA registrations, malpractice insurance certificates, and board certifications all have expiration dates. A recredentialing application that lands on a payer’s desk with an expired license doesn’t get processed. It gets returned. The credentialing calendar tracks the expiration date of every active credential for every provider and flags renewals before they expire, not after.
Active Application Follow-Up
Submitted recredentialing applications don’t process themselves. Payers have their own queues and timelines. Applications get stuck when payers request additional information and don’t receive it promptly. Active follow-up every two weeks on every in-flight application keeps renewals moving through the review process on a timeline that won’t miss the deadline.
How Qualigenix Manages Recredentialing for Practices
At Qualigenix, recredentialing is a core function, not an afterthought. We maintain a live renewal calendar for every provider across every payer for each client we serve. When a deadline is 90 days out, we start the renewal process. When a CAQH profile is 30 days from expiring, we send a re-attestation reminder. When a payer requests additional documentation mid-review, we respond and track the resolution.
We also monitor license expirations, DEA certificate renewals, and malpractice certificate dates for every provider we credential. A recredentialing application is only as strong as the documents supporting it. We don’t submit until we know everything in the application is current.
Our credentialing team handles recredentialing alongside initial credentialing, payer enrollment, CAQH profile maintenance, and Medicare revalidation for practices across 38+ specialties. When a provider joins a practice we serve, we start their initial credentialing immediately and build their renewal calendar from day one so the recredentialing cycle is tracked from the start, not discovered when a payer notice arrives.
Our results reflect a system that doesn’t miss deadlines: 99% claim accuracy rate, 95% first-pass acceptance rate, and an average 36-day collection cycle. We onboard new clients in as few as 6 days. If your practice is managing recredentialing without a reliable tracking system, we’re built to take that off your plate entirely.
Related services: Re-credentialing Services | Provider Credentialing | Payer Enrollment | CAQH Profile Management
Recredentialing Readiness Checklist
- Live renewal calendar maintained for every provider across every payer with deadlines and 90-day start dates
- CAQH re-attestation dates tracked per provider with 30-day advance reminders
- Medical license expiration dates monitored for all active providers
- DEA certificate renewal dates tracked and renewals initiated before expiration
- Malpractice insurance certificate dates confirmed current before any application submission
- Medicare revalidation due dates confirmed in PECOS annually for every enrolled provider
- PECOS mailing address verified current for all providers to ensure revalidation notices are received
- Recredentialing applications submitted 90 days before commercial deadlines
- Medicare revalidation submissions started 120 days before due date
- Active follow-up on every in-flight application every two weeks until confirmed approval
Frequently Asked Questions: Recredentialing
What is recredentialing?
Recredentialing is the periodic renewal process through which a payer re-verifies a provider’s qualifications and renews their network participation status. Most commercial payers require it every two to three years. Medicare requires revalidation every five years. The process involves updated documentation, CAQH profile verification, and a new application submission. Missing a deadline results in terminated participation and automatic claim denials that continue until reinstatement completes 90 to 120 days later.
How often is recredentialing required?
Commercial payers typically require recredentialing every two to three years. Medicare and Medicaid revalidation is required every five years for most provider types. CAQH ProView requires re-attestation every 120 days regardless of payer cycles. A provider with 10 active payer contracts has 10 independent recredentialing cycles running simultaneously, each on its own timeline set by each individual payer’s participation agreement.
What happens if a provider misses a recredentialing deadline?
A missed recredentialing deadline triggers payer termination of the provider’s network participation status. Claims submitted after the termination date deny as non-participating provider services. Getting back onto the panel requires a full reinstatement application treated as new credentialing, which takes 90 to 120 days. Revenue lost during this window is not recoverable retroactively. Patients may also receive unexpected balance bills for services delivered during the gap.
How long does recredentialing take to complete?
Recredentialing typically takes 60 to 120 days depending on the payer and the completeness of the application. Starting 90 days before the deadline gives the renewal enough time to process before participation expires. Applications started at 30 days or less risk not completing before the deadline, which turns a routine renewal into a reinstatement with a 90-to-120-day gap in billing.
What documents are required for recredentialing?
Recredentialing typically requires a current medical license, DEA certificate, malpractice insurance certificate with active policy dates, board certification documentation, NPI confirmation, and attestation of any changes in malpractice history or adverse actions. The provider’s CAQH profile must also be current and attested before submission. Some payers additionally require a current CV, hospital privileges verification, and attestation of criminal history changes since the last cycle.
What is the difference between recredentialing and Medicare revalidation?
Recredentialing is the commercial payer process of renewing network participation every two to three years. Medicare revalidation is the CMS process of confirming enrollment eligibility every five years through PECOS. Missing commercial recredentialing terminates network participation. Missing Medicare revalidation deactivates billing privileges, stopping all Medicare payments until revalidation completes. Both result in denied claims during the gap period with no retroactive payment recovery.
Does CAQH affect recredentialing?
Yes. Most commercial payers query CAQH ProView during recredentialing. An expired or incomplete CAQH profile delays the review and increases the risk of missing the deadline. CAQH requires re-attestation every 120 days. In multi-provider practices, multiple providers have staggered re-attestation windows throughout the year. Tracking and completing these re-attestations before they expire is a prerequisite for any smooth recredentialing process.
Can a provider still bill during recredentialing?
Yes, as long as the current participation status has not yet expired. A provider whose recredentialing application is in process can continue billing normally while the renewal processes. The billing disruption begins only if the renewal does not complete before the current participation term ends. Starting recredentialing 90 days before the deadline is specifically designed to prevent this overlap from occurring.
What is reinstatement after a recredentialing lapse?
Reinstatement is the process of reapplying to a payer network after participation has been terminated due to a missed recredentialing deadline. Most payers treat it as a new credentialing application taking 90 to 120 days. Revenue lost during the reinstatement window is not recoverable retroactively. The total cost of a missed deadline includes the revenue gap, staff time on the new application, patient balance billing disputes, and potential patient attrition to other in-network providers.
Should a practice outsource recredentialing management?
Most practices benefit from outsourcing recredentialing because tracking renewal cycles across multiple providers and payers requires consistent follow-through that in-house staff managing multiple responsibilities consistently cannot deliver reliably. A credentialing partner maintains a live renewal calendar, flags deadlines 90 days in advance, keeps CAQH profiles current, handles document collection and application submission, and follows up on in-flight renewals until confirmed approval. The cost of this service is a fraction of the revenue lost in a single missed deadline.
Related Resources from Qualigenix
- Re-credentialing Services
- Provider Credentialing Services
- Payer Enrollment Services
- CAQH Profile Management
- Insurance Credentialing for Multi-Provider Practices
- Telehealth Provider Credentialing
- CMS Medicare Revalidation Information (CMS.gov)
Recredentialing Deadlines Don’t Wait. Neither Should You.
Qualigenix tracks every recredentialing deadline, every CAQH re-attestation window, and every Medicare revalidation due date for every provider in your practice. We start renewals 90 days out so participation never lapses and billing never stops.
Our team delivers 99% claim accuracy, a 95% first-pass acceptance rate, an average 36-day collection cycle, and a 30% reduction in AR days. We onboard in as few as 6 days.
Precision. Progress. Qualigenix.
What’s Next

Vendor Credentialing Management for Healthcare Organizations: Keeping Compliance Current Across Every Vendor
Vendor credentialing is the process by which healthcare facilities verify that vendors, sales representatives, and third-party service providers meet...
CAQH Credentialing and Payer Enrollment: How One Expired Profile Blocks Every Application Behind It
CAQH credentialing is the process of building and maintaining a provider’s profile in the CAQH ProView database, which...
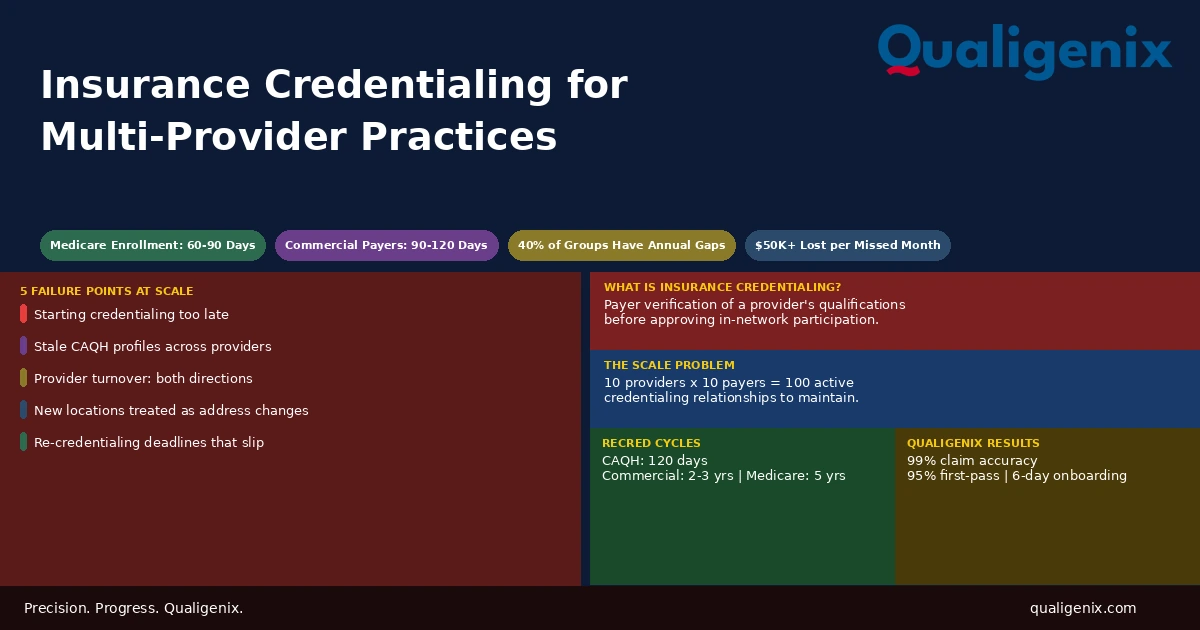
Insurance Credentialing for Multi-Provider Practices: What Breaks Down at Scale
Insurance credentialing is manageable for one or two providers. For practices with five, ten, or twenty providers across multiple...