No Surprises Act Compliance: What Your Good Faith Estimate Process Is Actually Missing
The Qualigenix Editorial Team consists of certified billing and coding experts with over 40 years of experience across 38+ medical specialties. Our content is rigorously researched against CMS, AMA, and payer-specific guidelines to ensure total compliance and accuracy. We apply the same elite standards to our resources as we do our client work, consistently delivering high claim accuracy and significant reductions in AR days.

The good faith estimate rule has been enforced since 2022, but most practices still run it as a price quote instead of a compliant document. The common gaps: quoting at check-in instead of scheduling, skipping required codes, missing self-pay patients who carry insurance, letting recurring estimates expire, and mishandling co-provider charges. Each gap opens the door to a $400 dispute or a $10,000 penalty.
A price you texted a patient isn’t a good faith estimate. Neither is a number your front desk read off a fee schedule. Since January 1, 2022, the No Surprises Act has required a specific written document for every uninsured and self-pay patient, with set fields and hard deadlines. Most practices assume they’re covered because they quote prices. They’re not. That gap is where the penalties and disputes live. Here’s what your process is probably missing.
A compliant good faith estimate is a written document a provider must give every uninsured or self-pay patient at scheduling. It lists itemized services, diagnosis and service codes, expected charges, provider details, and dispute-rights disclaimers. A verbal quote or a bare price doesn’t meet the standard and won’t defend you in a dispute.
The numbers that define good faith estimate compliance
These are the figures that decide whether your process holds up under scrutiny. Every deadline, threshold, and penalty below is a place where a loose workflow costs money.
| Requirement | Detail | Source |
|---|---|---|
| GFE requirement effective | January 1, 2022 | CMS / No Surprises Act |
| Who must receive one | All uninsured and self-pay patients | CMS, 45 CFR 149.610 |
| Specialties exempt | None; no site of service is exempt | CMS |
| Due (scheduled 3 to 9 business days out) | Within 1 business day | CMS |
| Due (scheduled 10+ days out or on request) | Within 3 business days | CMS |
| No GFE required when | Service scheduled under 3 business days out | CMS |
| Dispute (PPDR) trigger | Bill exceeds GFE by $400+ per provider | CMS, 45 CFR 149.620 |
| Patient window to file | 120 calendar days from bill date | CMS |
| Patient dispute fee | $25 administrative fee | CMS |
| Civil monetary penalty | Up to $10,000 per violation | CMS |
| Recurring-services GFE limit | Up to 12 months | CMS |
| Co-provider charge bundling | Under enforcement discretion (as of 2026) | HHS / CMS guidance |
| Insured-patient GFE + Advanced EOB | Enforcement deferred; unimplemented in 2026 | Federal Register RFI; HFMA |
| During an active dispute | Collections paused, late fees suspended | CMS |
| Qualigenix first-pass acceptance | 95% | Qualigenix |
| Qualigenix average onboarding | 6 days | Qualigenix |
What a compliant estimate actually requires
A compliant good faith estimate is a document with named fields, not a friendly number. It has to list the patient’s name and date of birth, an itemized list of the items and services you expect to provide, the diagnosis codes, the service codes, and the expected charge for each line. It also carries your identifying details and two disclaimers: one telling the patient about the dispute process, and one stating the estimate isn’t a contract.
That last part trips up practices that quote prices well. A front desk can be accurate to the dollar and still fail, because accuracy isn’t the test. The test is whether a written, coded, dated document sits in the chart. When an auditor or a dispute resolver asks for it, “we told them the price” is not an answer. The document is the answer.
Most enforcement actions so far have hit practices with no estimate on file at all. The fix costs almost nothing and prevents almost everything.
Does a compliant estimate need codes? Yes. Diagnosis codes and service codes are required elements. An estimate without them is incomplete, even if the dollar figure is right.
The clock starts at scheduling, not at the visit
This is the deadline most practices miss without realizing it. The estimate is tied to the scheduling event, not the appointment. Schedule a self-pay patient three to nine business days out, and the estimate is due within one business day. Schedule ten or more days out, and you have three business days. A patient can also request an estimate without booking anything, which also starts a three-business-day clock.
Practices that generate the estimate at check-in are already late by design. By the time the patient walks in, the window closed days ago. The estimate needed to leave your office long before the visit.
The one carve-out: if care is scheduled fewer than three business days ahead, no estimate is required for that visit. That exception is narrow, and leaning on it as a strategy is a poor bet.
The $400 dispute trap most practices never see coming
Here’s the mechanism that turns a sloppy estimate into a real cost. If a final bill from a single provider runs $400 or more above that provider’s estimate, the patient can open a federal patient-provider dispute. They have 120 days and pay a $25 fee. While the dispute runs, you can’t send the bill to collections, you can’t charge late fees, and you can’t retaliate.
The threshold is per provider, measured against the estimate you gave. Most practices never reconcile the two. They issue an estimate, bill whatever the visit actually cost, and never check the gap. When the bill lands $500 or $900 high, the patient has a clean path to dispute, and the practice has no defense on file.
Reconciling estimate to bill before the claim goes out is the single control that closes this. It’s also a revenue cycle function, not a front-desk task.
Is the $400 threshold based on the total bill or per provider? Per provider. Each provider’s bill is measured against that provider’s own estimate, not the combined total.
The self-pay patient you’re not screening for
Self-pay isn’t the same as uninsured. The rule counts anyone who chooses not to submit a claim to their plan as self-pay, even if they carry active coverage. A fully insured patient who says “I’ll just pay cash for this one” is now entitled to a written estimate.
Practices that screen only for the uninsured miss this group entirely. It’s a common gap in cash-pay services, elective procedures, and anything a patient prefers to keep off their insurance record. The question at scheduling can’t be “do you have insurance.” It has to be “are you using insurance for this visit.”
That single change to the intake script catches a population most estimate workflows ignore.
Recurring estimates that quietly expire
A single estimate can cover recurring care for up to 12 months, which is a gift for therapy, behavioral health, and any ongoing treatment. It has to state the frequency, the number of expected visits, and the per-visit cost. Issue it once at intake, and you’re covered for the year.
The catch is the refresh. You need a new estimate at the 12-month mark, or sooner if the schedule changes, a service is added, or the price moves. Practices set up the rolling estimate and then forget it exists. Twelve months later, the coverage lapsed and nobody noticed.
The clean pattern is to attach the refresh to annual intake paperwork so it can’t slip.
The co-provider trap door, and why discretion isn’t exemption
The original rule imagined a convening provider bundling co-provider charges into one estimate: lab work, anesthesia, ancillary services, all in a single document. HHS placed that bundling requirement under enforcement discretion in 2022 and, as of 2026, still hasn’t lifted it. So today you must issue your own estimate, but you’re not penalized for leaving a co-provider’s charges off it.
Two things make this a trap rather than a break. First, the moment you choose to list a co-provider’s charges, those charges become eligible for a patient dispute. Voluntarily bundling can expand your exposure, not reduce it. Second, discretion can end. HHS has extended it more than once, and the day it lifts, every convening practice needs a working data pipeline between providers already in place.
Treating “not enforced yet” as “handled” is how practices get caught flat when the rule catches up.
What’s coming: insured-patient estimates and the Advanced EOB
The No Surprises Act also requires providers to send estimates to health plans for insured patients, so plans can issue an Advanced Explanation of Benefits before care. That piece has never been enforced. Regulators deferred it in 2022 and it remains unimplemented in 2026.
It isn’t dead, though. In 2025, bipartisan members of Congress pressed the agencies to finish the rulemaking, and health finance groups expect movement. When it lands, the workflow gets heavier: estimates will need to flow from your systems to payers, tied into EHRs, patient accounting, and clearinghouses.
Practices running estimates as a manual front-desk task now will feel that shift hard. The ones with a structured, system-level process will absorb it. Building the workflow before the deadline is the difference between a smooth transition and a scramble.
Price quote versus compliant estimate
The distance between what most practices do and what the rule requires is easy to see side by side.
| Element | Typical price quote | Compliant estimate |
|---|---|---|
| Format | Verbal or a texted number | Written, dated document |
| Codes | None | Diagnosis and service codes |
| Disclaimers | None | Dispute rights + not-a-contract notice |
| Timing | At check-in | Within the deadline from scheduling |
| Defends a dispute | No | Yes |
Can a good-faith error be corrected? Yes. If you act in good faith and fix an omission as soon as practicable, that correction counts. A missing document, though, is much harder to defend.
Where Qualigenix closes the gap
Good faith estimate compliance breaks down at the workflow level, and that’s where we work. Qualigenix builds estimate generation and reconciliation into the revenue cycle instead of leaving it on the front desk. We screen for self-pay correctly at scheduling, produce coded written estimates on time, and reconcile every estimate against the final bill before it goes out, so per-provider variance stays under the $400 line.
We also handle the parts that quietly fail: refreshing recurring estimates on schedule, keeping a written record in the chart for every self-pay account, and preparing your data flow for the insured-patient rules when they arrive. See our revenue cycle management and medical billing services, and pair them with denial management to protect the back end too. We onboard in as few as six days and hold a 95% first-pass acceptance rate.
What practice managers say about working with Qualigenix
“We were issuing verbal quotes and had three self-pay disputes in a single quarter. Qualigenix rebuilt our intake so every self-pay patient gets a coded, written estimate at scheduling. We’ve had zero disputes in eight months.”
Danielle Marsh
Practice Manager, Orthopedics, Texas
“Our final bills were drifting $600 to $900 over what we quoted. Qualigenix set up estimate-to-bill reconciliation, and the variance dropped under the $400 line on 97% of our self-pay accounts.”
Marcus Reilly
Billing Director, Gastroenterology, Florida
“We didn’t realize insured patients paying cash still needed an estimate. Qualigenix caught it in the audit and closed the gap before it cost us. Onboarding took six days.”
Priya Nandakumar
Revenue Cycle Lead, Dermatology, Arizona
“Recurring therapy estimates were expiring and nobody was refreshing them. Qualigenix built a 12-month rolling estimate workflow into our EHR. Compliance stopped being a quarterly scramble.”
Kevin Osei
Operations Manager, Behavioral Health, Ohio
Your good faith estimate audit checklist
Run your current process against these ten checks. Every “no” is exposure.
- ☐ We ask “are you using insurance for this visit,” not just “do you have insurance.”
- ☐ Every self-pay estimate is a written, dated document, not a verbal quote.
- ☐ Each estimate includes diagnosis codes and service codes.
- ☐ Each estimate carries the dispute-rights and not-a-contract disclaimers.
- ☐ Estimates go out within the deadline measured from scheduling, not check-in.
- ☐ We reconcile every final bill against its estimate before it goes out.
- ☐ Per-provider variance stays under the $400 dispute threshold, or the reason is documented.
- ☐ Recurring-services estimates are refreshed at 12 months or when terms change.
- ☐ A written estimate sits in the chart for every self-pay account.
- ☐ We have a plan for the insured-patient estimate rules before they take effect.
Frequently asked questions
Is a verbal price quote a good faith estimate?
No. It has to be a written document with itemized services, diagnosis and service codes, expected charges, provider details, and dispute disclaimers. A verbal quote or a bare price won’t defend you in a dispute.
When is a good faith estimate due?
The clock starts at scheduling. If care is booked 3 to 9 business days out, it’s due within 1 business day. If booked 10 or more days out, or requested on demand, it’s due within 3 business days.
What triggers a patient-provider dispute?
A final bill from one provider that runs $400 or more above that provider’s estimate. The patient has 120 days and pays a $25 fee. Collections and late fees pause while the dispute is open.
Do insured patients ever need a good faith estimate?
Yes, whenever they choose not to bill insurance for a visit. That makes them self-pay under the rule, even with active coverage. The separate provider-to-plan estimate for insured patients is not yet enforced.
Do we have to include co-provider charges?
Not as of 2026. HHS is still exercising enforcement discretion on bundling. You must issue your own estimate. If you do list a co-provider’s charges, those charges become eligible for a patient dispute.
What’s the penalty for a missing estimate?
Up to $10,000 per violation. Most enforcement actions so far involved practices with no written estimate on file at all, which makes the missing document the biggest single source of risk.
How long can one estimate cover recurring care?
Up to 12 months, if it states the frequency, visit count, and per-visit cost. You reissue at the 12-month mark, or sooner if the schedule, service, or price changes.
Related resources
- Revenue cycle management services
- Medical billing services
- Denial management and appeals
- CMS No Surprises Act guidance
Turn compliance into an intake checklist, not a fire drill
Qualigenix builds good faith estimate generation and reconciliation into your revenue cycle, so disputes and penalties stop starting with a missing document.
Our team delivers 99% claim accuracy, a 95% first-pass acceptance rate, an average 36-day collection cycle, and a 30% reduction in AR days. We onboard in as few as 6 days.
Precision. Progress. Qualigenix.
What’s Next
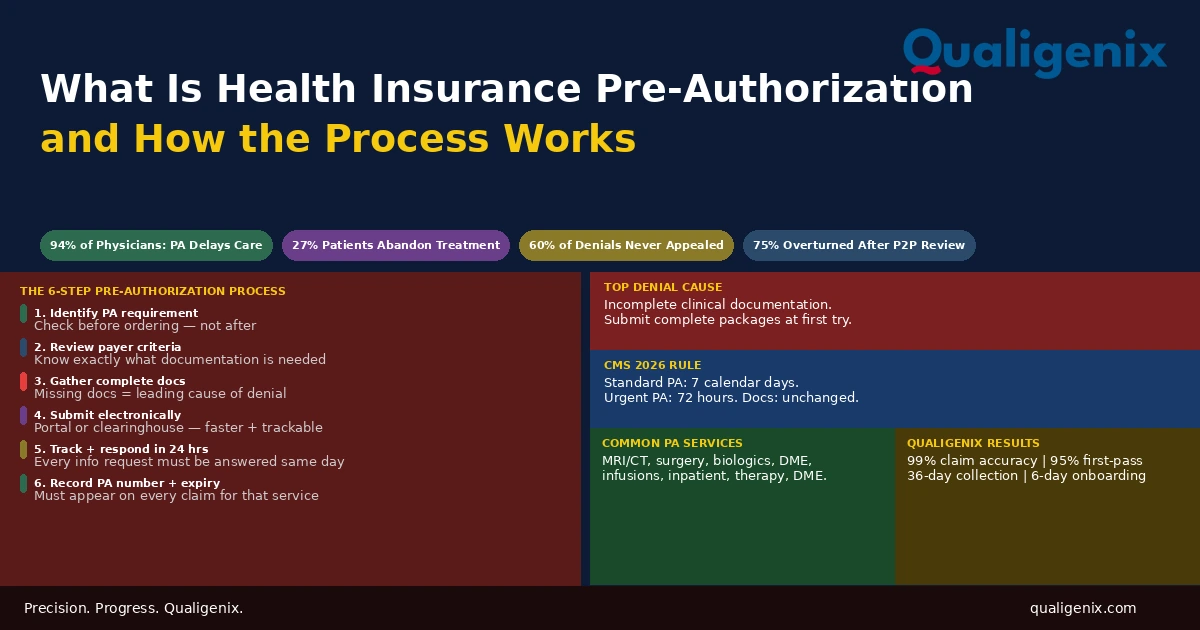
What Is Health Insurance Pre-Authorization and How It Works
Health insurance pre-authorization is the approval step that sits between a physician’s clinical decision and a patient’s access to...
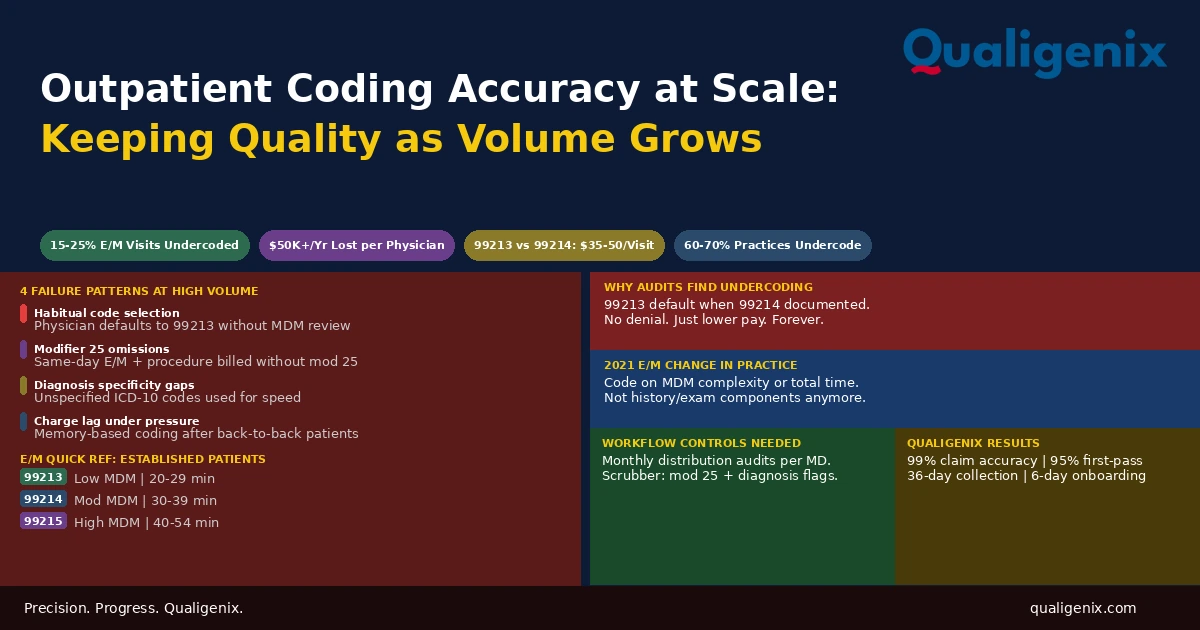
Outpatient Coding for High-Volume Practices: Keeping Accuracy at Scale
Outpatient coding accuracy is manageable when a physician sees 10 patients a day. It degrades predictably when they see...
Medicare Physician Fee Schedule 2026: What Every Practice Must Know
The 2026 Medicare Physician Fee Schedule (CMS-1832-F) introduces two separate conversion factors for the first time: $33.57 for qualifying...