Technical Denials in Medical Billing 2026: Why Claim Rejection Rates Are Rising and How to Fight Back
The Qualigenix Editorial Team consists of certified billing and coding experts with over 40 years of experience across 38+ medical specialties. Our content is rigorously researched against CMS, AMA, and payer-specific guidelines to ensure total compliance and accuracy. We apply the same elite standards to our resources as we do our client work, consistently delivering high claim accuracy and significant reductions in AR days.

Claim denial rates are climbing in 2026, and the culprit isn’t clinical. It’s technical. Practices that haven’t updated their billing workflows for the 2026 CPT and ICD-10 code changes are getting hit with rejections they don’t see coming. The cost adds up fast — and most of these denials are entirely preventable.
Technical denials — rejections caused by administrative errors, not clinical ones — are surging in 2026. The 2026 CPT update brought 288 new codes and 84 deletions. CMS added 614 new ICD-10-CM codes. Prior authorization requirements rose 30% in three years. Practices that don’t update billing workflows and adopt front-end verification are losing recoverable revenue every single day.
What are technical denials in medical billing? Technical denials occur when a payer rejects a claim due to administrative or data errors — missing modifiers, incorrect NPI, duplicate submissions, expired prior authorizations, or wrong patient demographics. They’re not about whether the care was appropriate. They’re about whether the paperwork was right. In 2026, they account for a growing share of the industry’s 10–15% average denial rate.
Key Statistics: Technical Denials and Claim Rejection Trends in 2026
| Statistic | Figure | Source |
|---|---|---|
| Industry average claim denial rate | 10–15% | Healthcare Finance News, 2026 |
| Providers reporting denial rates over 5% | 20% (up from 12%) | MGMA Survey, 2026 |
| Prior authorization requirements increase (last 3 years) | +30% | Healthcare Finance News, 2026 |
| 2026 CPT total code-set changes | 418 (288 new, 84 deleted, 46 revised) | AMA / zHealth, 2026 |
| New ICD-10-CM codes effective Oct 1, 2025 | 614 new codes + 28 deletions | CMS.gov, 2025–2026 |
| April 1, 2026 ICD-10 procedure code updates | Additional codes effective Apr 1–Sep 30, 2026 | CMS.gov, 2026 |
| Practices with no AI/automation in RCM | 59% | RCM Trends Report, 2026 |
| Practices with fully integrated AI across RCM | 2% | RCM Trends Report, 2026 |
| Denied claims that are recoverable | ~76% | Industry RCM Benchmarks, 2026 |
| Denied claims actually appealed by practices | ~63% | Industry RCM Benchmarks, 2026 |
| Cost to rework a single denied claim | $25–$118 per claim | HFMA Benchmarks, 2026 |
| Hospitals planning to expand RCM outsourcing | 70% | Auxis Healthcare RCM Report, 2026 |
| U.S. RCM market value in 2026 | $72.96 billion | Towards Healthcare Market Report, 2026 |
| Medical group leaders increasing workforce investment | 37% | MGMA Poll, 2026 |
| Payer enrollment write-offs exceeding $500K | Nearly 12% of organizations | HealthStream Provider Enrollment Report, 2026 |
What Exactly Is a Technical Denial?
A technical denial isn’t about the care. It’s about the claim. Payers reject these claims because something in the paperwork doesn’t match their requirements — not because the service wasn’t medically necessary.
Common technical denial triggers include missing or incorrect procedure modifiers, wrong or missing NPI numbers, duplicate claim submissions, authorization numbers not included on the claim, and patient demographic mismatches between the claim and the payer’s records. Any one of these errors can stop a clean claim dead before a human reviewer ever looks at it.
That’s what makes them so frustrating. You delivered the care. The patient was covered. But the claim bounced because of a data entry issue at registration or a modifier your billing team didn’t know was required for that payer.
Why Technical Denials Are Spiking in 2026
Three forces are colliding right now, and practices that haven’t adapted are getting hit from all sides.
The 2026 CPT Code Overhaul
The American Medical Association released 418 total CPT code changes for 2026 — 288 brand-new codes, 84 deleted codes, and 46 revisions. That’s one of the largest single-year updates in recent memory. Practices billing with outdated code sets are submitting claims with codes that simply don’t exist in payers’ systems anymore. Automatic rejection.
The biggest areas of change are digital health services, remote patient monitoring (including new codes for short-duration monitoring episodes of 2–15 days), and AI-augmented diagnostic services like coronary plaque assessment. Specialties that haven’t updated their fee schedules and superbills are especially exposed.
The ICD-10-CM Update Wave
CMS released 614 new ICD-10-CM codes effective October 1, 2025. Then, on April 1, 2026, CMS released another round of procedure code updates effective through September 30, 2026. That’s two major coding updates in less than a year. Practices that don’t stay current with both sets are billing with stale diagnosis codes that don’t map to the new specificity requirements payers now expect.
The coding error doesn’t have to be dramatic to cause a denial. A single digit off, a deleted code still in your system, or a new specificity level your team didn’t know about is enough.
The Prior Authorization Squeeze
Prior authorization requirements have increased 30% over the past three years. More services require auth. Auth processes take longer. And when an auth expires — or wasn’t obtained in the first place because your workflow didn’t flag it — the resulting denial is technical, not clinical. The payer doesn’t care that the service was necessary. If the auth isn’t on file, the claim fails.
Q: Are technical denials more common than clinical denials?
In most practices, yes. Technical denials — from eligibility issues, missing information, and administrative errors — make up the majority of first-level rejections. Clinical denials based on medical necessity determinations tend to be less frequent but harder to appeal. The good news: technical denials are almost entirely preventable with the right front-end workflow.
The Hidden Financial Damage
Each denied claim costs $25 to $118 to rework — and that’s before you count the time your billing team spends tracking it down, pulling documentation, and resubmitting. For a practice receiving 50 denials a week, that’s $1,250 to $5,900 in rework costs every single week. Over a year, that’s a serious problem.
The gap between recoverable and recovered denials makes it worse. About 76% of denied claims can be appealed and paid. But only around 63% of denied claims actually get appealed. The rest get written off — often because the billing team is too busy handling new claims to go back and fight old ones. That’s not a small number. For a mid-sized practice, that gap represents tens of thousands of dollars in lost annual revenue.
Q: How quickly do I need to appeal a denied claim?
Payer timelines vary, but most require appeals within 60 to 180 days of the denial date. Some Medicare Advantage plans have shorter windows — as few as 30 days. Missing an appeal deadline means that revenue is gone permanently. Setting internal appeal SLAs of 30 days from denial date gives your team a buffer and maximizes recovery rates.
Where the Denials Are Coming From: Root Cause Categories
Not all technical denials have the same origin. Understanding the root cause is the only way to fix the pattern — not just the individual claim. Here are the most common categories billing teams are seeing in 2026:
Registration and Eligibility Errors
Wrong date of birth, misspelled name, incorrect insurance ID — these get flagged the moment the claim hits the clearinghouse. Real-time eligibility verification at every patient interaction catches these before the claim is even built. Still, 59% of practices haven’t implemented any AI or automation in their RCM workflows, which means most are still catching these errors manually — or not at all until the denial arrives.
Missing or Incorrect Modifiers
Modifier requirements vary by payer, by specialty, and by service. What Cigna requires for a bilateral procedure may differ from what UnitedHealthcare expects. Without payer-specific editing rules in your billing system, these mismatches slip through at scale. The 2026 CPT changes include revisions to how certain modifier combinations should be applied, adding new layers of complexity.
Prior Authorization Gaps
This is the category growing fastest in 2026. With prior auth requirements up 30% in three years, practices that don’t have a dedicated auth tracking workflow are constantly playing catch-up. An authorization that was valid for 90 days expires before the service is delivered. Or the authorization was obtained for a slightly different procedure code than the one actually billed. Either way, the claim fails.
Q: Should I invest in AI to prevent technical denials?
AI denial prediction tools are genuinely useful — they can flag high-risk claims before submission based on historical payer behavior and coding patterns. But only 2% of practices have fully deployed AI across their RCM operations, and 59% haven’t started at all. If you’re not ready to implement AI internally, partnering with an RCM firm that already has these tools deployed is a faster and more cost-effective path to reducing denials.
What High-Performing Billing Teams Are Doing Differently
The practices holding denial rates well below the 10–15% industry average aren’t doing anything exotic. They’ve built disciplined front-end processes, and they enforce them consistently. Here’s what separates them from the rest.
Front-End Verification Is Non-Negotiable
Real-time eligibility verification — run at scheduling, at check-in, and again on the day of service — catches most demographic and coverage errors before the claim is ever built. This single step eliminates a significant portion of technical denials that originate at registration. It’s not glamorous, but it works.
Claim Scrubbing Before Every Submission
Automated claim scrubbing tools review every claim for errors before it goes to the payer. They check for missing modifiers, NPI validation, diagnosis code specificity, and duplicate submission flags. The best tools apply payer-specific rules — so what passes for Medicare doesn’t get scrubbed the same way as a commercial plan. This is where the 2026 CPT and ICD-10 updates get caught before they become denials.
Denial Tracking by Root Cause
High-performing billing teams don’t just work individual denied claims. They track every denial by root cause category, payer, and provider. When the data shows that 40% of denials from one payer involve a specific modifier combination, they fix the systemic issue — not just the latest claim. That’s how you actually bend the denial rate curve downward.
How Qualigenix Healthcare Reduces Technical Denial Rates
Qualigenix Healthcare specializes in medical billing and revenue cycle management for practices, hospitals, and multi-specialty groups across the United States. Their team’s performance metrics speak directly to the denial problem.
Qualigenix achieves a 99% claim accuracy rate and a 95% first-pass acceptance rate — meaning 95 out of every 100 claims submitted are accepted and processed on the first attempt. That’s not a lucky outcome. It’s the result of payer-specific editing rules, real-time eligibility verification, updated code libraries that reflect every 2026 CPT and ICD-10 change, and a dedicated team monitoring denials by root cause daily.
Their results also include a 30% reduction in accounts receivable days and an average 36-day collection cycle. Practices that have moved their billing to Qualigenix report dramatically fewer denial-related write-offs and faster cash flow. For practices that need to get started quickly, Qualigenix offers a 6-day onboarding timeline.
On the credentialing side, Qualigenix’s provider credentialing and payer enrollment services ensure providers are enrolled correctly with every relevant payer before claims are ever submitted — eliminating one of the most common sources of avoidable denials.
Technical Denial Prevention Checklist for 2026
Use this checklist to assess your current denial prevention posture. Every unchecked item is a potential denial waiting to happen.
- Code libraries updated for all 2026 CPT changes (288 new codes, 84 deletions, 46 revisions)
- ICD-10-CM system updated for October 2025 and April 2026 CMS releases
- Real-time eligibility verification running at scheduling, check-in, and day of service
- Automated claim scrubbing tool active with payer-specific editing rules
- Prior authorization tracking workflow in place for all services requiring auth
- Authorization expiration alerts set up in your scheduling or billing system
- Denial root cause tracking and reporting by payer and provider
- Appeal SLA defined and enforced (recommended: 30 days from denial date)
- Front-desk staff trained on the impact of registration errors on billing
- Monthly denial trend review with billing leadership or RCM partner
FAQ: Technical Denials in Medical Billing 2026
Q: What is a technical denial in medical billing?
A technical denial occurs when a payer rejects a claim due to administrative or data errors — things like missing modifiers, incorrect patient demographics, duplicate claim submissions, or missing prior authorization numbers. They’re not about medical necessity. They’re about billing execution, which means they’re also almost entirely preventable.
Q: Why are technical denials increasing in 2026?
Three factors are driving the surge: the 2026 CPT update introduced 288 new codes and 84 deleted ones, creating significant room for coding errors; CMS released 614 new ICD-10-CM codes effective October 2025, plus another update round in April 2026; and prior authorization requirements increased 30% in the last three years, adding administrative complexity that leads directly to more technical rejections.
Q: What is the average claim denial rate in 2026?
The industry average sits at 10–15% in 2026. The percentage of providers reporting denial rates above 5% has nearly doubled — from 12% to 20% — in recent years. Some specialties with complex payer mixes or high prior authorization volume face even higher rates.
Q: How much does a denied claim cost to rework?
Industry benchmarks put the rework cost at $25 to $118 per denied claim. For a practice managing 50 denials per week, that’s up to $5,900 weekly — or more than $300,000 annually — in rework costs alone, before accounting for any revenue that goes uncollected.
Q: Can technical denials be appealed?
Yes — most technical denials can be corrected and resubmitted rather than formally appealed. Once the error is fixed (wrong modifier, updated demographic, added auth number), the claim can be resubmitted and typically paid. Formal appeals are more often needed for clinical denials. The key is having a billing workflow that catches and resubmits corrected technical denials quickly — before payer timelines close.
Q: What CPT changes in 2026 are causing the most denials?
The highest-risk areas are remote patient monitoring (new codes for 2–15 day episodes), digital health and telehealth services, AI-augmented diagnostics, and specialty services that had existing codes deleted or revised. Practices still using deleted 2025 codes will get automatic rejections. Superbills and fee schedules must be updated to reflect 2026 codes before claims are submitted.
Q: Should I outsource billing to reduce technical denials?
For most practices, yes — outsourcing to a specialized RCM firm is the fastest and most cost-effective path to a lower denial rate. Specialized billing companies maintain current code libraries, use advanced claim scrubbing technology, and have denial trend data across multiple payers and specialties that an in-house team can’t match. Qualigenix Healthcare onboards new clients in as few as 6 days and achieves a 95% first-pass acceptance rate.
Q: How do I know if my current denial rate is too high?
If your overall claim denial rate is above 5%, you’re losing ground relative to well-managed practices. If it’s above 10%, you’re near the industry average — which means you’re leaving significant recoverable revenue uncollected. A first-pass acceptance rate below 90% is a clear signal that your front-end billing workflow needs attention. Pull 90-day denial data by payer and root cause — the patterns will tell you where to focus first.
Stop Losing Revenue to Preventable Denials
Technical denials are costing your practice real money — and most of them shouldn’t be happening at all. Qualigenix Healthcare fixes the root causes, not just the individual claims.
Our team delivers 99% claim accuracy, a 95% first-pass acceptance rate, an average 36-day collection cycle, and a 30% reduction in AR days. We onboard in as few as 6 days.
What’s Next
Medical Coding Errors That Cost Practices the Most (And How to Catch Them Before They Submit)
Medical Coding Errors That Cost Practices the Most (And How to Catch Them Before They Submit) Written by the...
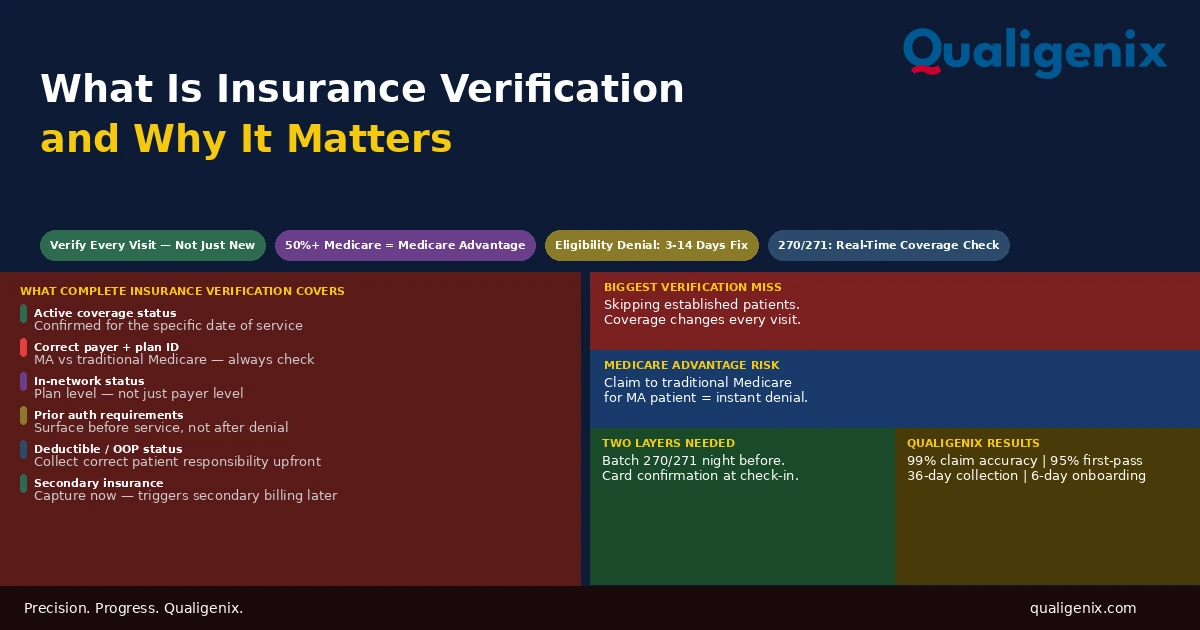
What Is Insurance Verification and Why It Matters
Insurance verification is the front-end process that determines whether a claim will be paid before the patient ever enters...

Insurance Denial Appeals: What Practices Miss
Most insurance denial appeals that fail don’t fail because the clinical case was weak. They fail because the...