Accounts Receivable In Medical Billing: How to Reduce Days in AR Without Hiring More Staff
The Qualigenix Editorial Team consists of certified billing and coding experts with over 40 years of experience across 38+ medical specialties. Our content is rigorously researched against CMS, AMA, and payer-specific guidelines to ensure total compliance and accuracy. We apply the same elite standards to our resources as we do our client work, consistently delivering high claim accuracy and significant reductions in AR days.
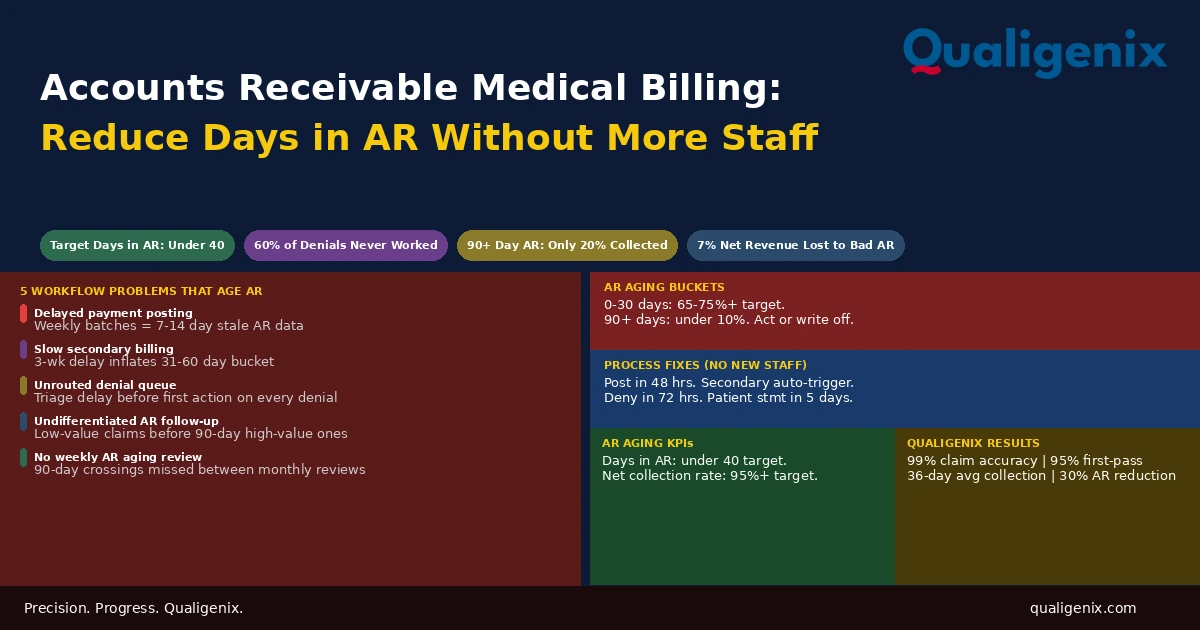
Days in AR in medical billing is not primarily a staffing problem. It is a workflow problem. The practices with the lowest days in AR don’t have more billing staff than average. They have faster payment posting, faster denial turnaround, automatic secondary billing triggers, systematic follow-up by aging bucket, and weekly AR reviews that catch aging balances before they cross the 90-day threshold. Each of these changes is operational. None requires adding headcount to produce a measurable improvement in AR performance.
When days in AR creeps above 50, the instinct in most practices is to look at staffing. Someone needs to work the denial queue more aggressively. Someone needs to follow up on aging claims. Someone needs to post payments faster. All of that is true. The instinct to hire misses the more important question: why are there so many denials to work, why is posting falling behind, and why are claims aging without follow-up in the first place?
The answer almost always traces to workflow design, not capacity. Denials pile up because no one defined how quickly they must be worked or who is responsible for each type. Posting falls behind because it runs on a weekly batch schedule that made sense when claims volume was lower. Claims age without follow-up because the follow-up process is reactive rather than calendar-driven. These are process problems. Hiring more staff to manage a broken process produces a marginal improvement at significant cost. Fixing the process produces a larger improvement at no additional cost.
This blog identifies the specific workflow inefficiencies that cause AR to age in medical billing and the targeted changes that move days in AR downward without adding a single billing position.
Accounts receivable in medical billing is the total outstanding amount owed for services delivered but not yet collected. Days in AR measures how long it takes, on average, to collect after service delivery. The target benchmark is under 40 days. Reducing days in AR without adding staff requires: posting payments within 48 hours, triggering secondary billing automatically on primary adjudication, working denials within 72 hours using root cause routing, following up on aging claims by bucket and dollar value, and running weekly AR aging reviews before balances cross 90 days.
Accounts Receivable Medical Billing: Key Benchmarks
| Metric | Target / Benchmark | Warning Level |
|---|---|---|
| Days in AR | Under 40 days | Above 50 days |
| High-performing practice days in AR | 30 to 35 days | Above 60 days is critical |
| AR in 0-30 day bucket | 65% to 75% or higher | Below 60% |
| AR past 90 days collection probability | Target: under 10% of total AR | Above 20% of total AR |
| Net collection rate | 95% or higher | Below 90% |
| Denial rate | Under 5% of submitted claims | Above 10% |
| Denied claims never reworked | Target: under 10% of denials | Industry average: approx. 60% |
| Payment posting turnaround | Within 48 hours of ERA receipt | Beyond 5 business days |
| Secondary claim submission turnaround | Within 5 days of primary adjudication | Beyond 14 days |
| Patient statement turnaround after adjudication | Within 5 business days | Beyond 14 days |
| Revenue lost to uncollected AR annually | Target: under 2% of net revenue | Up to 7% in poor-performing practices |
| Qualigenix average collection cycle | 36 days | N/A |
| Qualigenix AR days reduction for clients | 30% improvement | N/A |
| Qualigenix claim accuracy rate | 99% | N/A |
What Days in AR Actually Measures
Days in AR is the single most useful summary metric in medical billing. It captures the combined effect of every upstream process in the revenue cycle: registration accuracy, claim submission timeliness, denial management responsiveness, payment posting speed, and patient collections follow-through. If any of these stages is underperforming, days in AR will reflect it before any other metric does.
The formula is straightforward: divide total AR by average daily charges. A practice with $500,000 in outstanding AR and $15,000 in average daily charges has approximately 33 days in AR, which is excellent. The same practice with $900,000 in AR has 60 days in AR, which signals a serious systemic problem somewhere in the cycle.
Days in AR doesn’t tell you where the problem is. It tells you there is one. The AR aging report tells you where. A practice with high days in AR and most of the excess in the 31-to-60-day bucket has a different problem than one whose excess is concentrated past 90 days. The first likely has a denial management or secondary billing delay. The second has claims that were allowed to age without intervention until they became near-uncollectable.
The 90-day threshold deserves particular attention. Research consistently shows that only about 20% of AR past 90 days is ultimately collected without extraordinary intervention. Every dollar that crosses that line is substantially impaired. A practice with 25% of its AR in the 90-plus bucket is not just having a slow collection quarter. It is carrying a write-off liability that will materialize over the next few months whether or not anyone takes action on it.
The 5 Workflow Problems That Age AR
Before prescribing fixes, it helps to understand precisely what causes AR to age. In the practices Qualigenix works with across 38+ specialties, days in AR problems almost always trace to one or more of five specific workflow failures. None of them requires more staff to fix. All of them require a process change.
Workflow Problem 1: Delayed Payment Posting
When a payer adjudicates a claim and sends an ERA (Electronic Remittance Advice), that payment needs to be posted to the practice management system promptly. Posting closes the claim on the payer side and either triggers the next step, secondary billing or patient billing, or confirms the account as collected.
Practices that post payments weekly, or in manual batches whenever someone has time, are operating with AR data that is 5 to 10 business days stale at any given point. The AR report shows claims as outstanding that have actually been paid. Follow-up staff contact payers about claims that have already been adjudicated. Reports show higher days in AR than the practice is actually experiencing. Every management decision made from that data is made with distorted information.
The fix is a 48-hour posting standard. Every ERA received must be posted within 48 hours. This is not a request or a best effort. It is an operational requirement with named accountability. For practices using electronic ERAs with automated posting rules configured in their practice management system, much of this happens without manual intervention. For those without automated posting, the 48-hour standard still applies and is achievable with current staff if posting is prioritized as a daily function rather than a weekly batch task.
Workflow Problem 2: Delayed Secondary Billing
Approximately 80% of Medicare patients carry secondary coverage, and dual-eligible Medicaid patients carry secondary by definition. When a primary claim is adjudicated, a secondary claim must follow promptly. The secondary claim must include the primary EOB showing what was paid, adjusted, or denied. It cannot be submitted until the primary adjudication is complete. But once it is complete, there is no justification for delay.
In many practices, secondary billing happens when a billing coordinator gets to it, which can be anywhere from the same day to three weeks after the primary ERA is received. A three-week secondary billing delay means a claim that should have been fully resolved in 30 days is still open at 50 days. Multiply that across the practice’s Medicare and dual-eligible population and it produces a consistent elevation in days in AR that looks like a payer problem but is actually an internal workflow problem.
Warning: Secondary claim delays compound when practices don’t have secondary insurance captured correctly at registration. A patient with Medicare primary and a Medigap secondary where the Medigap information is missing from the patient record will never generate a secondary claim automatically. The primary claim resolves. The patient balance sits in AR. No secondary is ever sent. The Medigap revenue that would have eliminated or reduced the patient balance is permanently lost because a registration field was empty when it shouldn’t have been.
Workflow Problem 3: Slow Denial Working
This is the most impactful single driver of elevated days in AR in most practices. A denied claim remains in AR as an outstanding balance from the date of service until it is either recovered or written off. The longer it sits unworked, the less likely recovery becomes. Appeal windows close. Documentation gets harder to produce. The account ages through the buckets.
The industry data on this is stark: approximately 60% of denied claims are never reworked by practices. That is not a small inefficiency. It is the majority of denied claims simply sitting in the denial queue until they are written off or until a periodic AR review finds them, often too late. The reason most denials go unworked is not lack of effort. It is lack of a structured workflow that assigns responsibility, sets deadlines, and tracks resolution.
Denial working must have a defined turnaround standard. Every denial received must be assigned to the appropriate staff member within 24 hours and worked within 72 hours. Not reviewed. Not queued for review. Actually worked: the denial reason identified, the response determined, and the corrected claim or appeal initiated. A 72-hour working standard applied consistently produces a measurable reduction in days in AR within 60 days of implementation.
Workflow Problem 4: Undifferentiated AR Follow-Up
In practices without a structured AR follow-up process, follow-up happens in whatever order the staff member opens accounts, which is usually either chronological by date of entry or alphabetical by patient name. Neither approach prioritizes the accounts that are closest to becoming uncollectable or represent the highest revenue value at risk.
Effective AR follow-up is prioritized by two variables: aging bucket and dollar value. Claims in the 61-to-90-day bucket must be addressed before they cross 90 days and their collection probability drops to 20%. Within each aging bucket, higher-value claims receive follow-up before lower-value ones. A $2,500 claim at 65 days old is a much higher priority than a $150 claim at the same age. Following up on them in the reverse order wastes staff capacity and allows high-value accounts to slip past recovery windows while staff are occupied with accounts that don’t justify the effort.
Workflow Problem 5: No Weekly AR Aging Review
Many practices review AR monthly. Some do it quarterly. Both are too infrequent to catch accounts moving toward the 90-day threshold in time to do something about them. A balance that is at 62 days during a monthly review is at 92 days by the next one. It crossed the threshold between reviews. No one intervened because no one knew it was approaching.
Weekly AR aging reviews are not optional in a well-run billing operation. They are the mechanism by which the billing team identifies accounts that need escalation before they become write-offs. The review doesn’t need to be a comprehensive audit of every account every week. It needs to flag every account crossing from 60 days to 90 days, every account that has been unresponsive to follow-up attempts, and any new denial category that is appearing with unusual frequency.
Fix 1: The 48-Hour Payment Posting Standard
Implement a written policy: all ERAs received are posted within 48 hours. This applies whether the ERA arrived on a Monday or a Friday. The 48-hour clock starts at receipt, not at the next available posting window.
For practices already using electronic ERA with auto-posting capability in their practice management system, this is largely a configuration exercise. Most modern billing systems can post standard payment and adjustment transactions automatically based on payer-specific rules configured in the system. Manual posting is required for exceptions: claims where the ERA amount differs from the expected contractual amount, denial lines that require routing to the denial queue, and credits or recoupments that need review before posting.
Auto-posting eliminates the volume problem. Manual review handles the exceptions. The result is a daily posting cycle that keeps AR data current, triggers secondary billing and patient statements on a predictable schedule, and gives the AR team accurate information to act on rather than a view that lags collection reality by a week or more.
Fix 2: Automatic Secondary Billing on Primary Adjudication
Secondary billing should not require a staff member to notice that the primary claim was adjudicated and manually initiate the secondary. It should trigger automatically. When a primary ERA posts and the patient record shows active secondary coverage, the billing system should queue a secondary claim for submission without human initiation.
Most modern practice management systems support this workflow. The configuration requires that secondary insurance is correctly captured at registration for every patient who has it, that the system’s secondary billing rules are configured to trigger on primary adjudication, and that the secondary claim generation is reviewed for exceptions before batch submission rather than reviewed claim by claim.
The productivity gain from automatic secondary billing is immediate and measurable. Staff who were manually initiating secondary claims can redirect that time to denial working and follow-up, which moves days in AR on two dimensions simultaneously: secondary claims resolve faster, and denial follow-up gets more attention.
Fix 3: Root Cause Routing for Denials
The traditional denial management workflow routes all denials to a single queue where staff work them in whatever order they’re accessed. This creates a triage step before every denial action: the staff member must read the denial reason, determine the correct response, and either work the denial themselves or route it to someone else. That triage step adds time to every denial and means that denials requiring physician involvement, such as clinical or medical necessity denials, sit in a general queue until a billing coordinator notices they need to be escalated.
Root cause routing eliminates triage by sorting denials at intake based on denial reason code. Administrative denials go directly to the billing team. Medical necessity denials go directly to the clinical review queue for physician attention. Credentialing denials go to the credentialing team. Eligibility denials go back to registration for verification and correction. Each denial arrives in the right queue for the right staff member on the day it’s received, not after someone works backward through a mixed queue to figure out who should handle it.
Root cause routing also enables root cause analysis. When administrative denials are grouped by reason code in their own queue, patterns become visible immediately. If 30 denials in a single week share the same reason code, that’s a systemic issue, not 30 individual problems. Identifying and fixing the upstream process that generated those 30 denials prevents the next 30. Denial management without root cause analysis treats symptoms indefinitely. Root cause routing makes the pattern impossible to miss.
Fix 4: Tiered Follow-Up by Aging Bucket and Dollar Value
Replace undifferentiated AR follow-up with a tiered protocol that directs effort toward the accounts where it produces the most value. The structure is simple: every week, the AR aging report is reviewed and accounts are triaged into three follow-up tiers.
Tier 1 covers claims in the 61-to-90-day bucket, regardless of dollar value. These accounts are approaching the threshold where collection probability drops significantly. Every one of them needs an action this week: a status call to the payer, an appeal submission, or a corrected claim resubmission if a correctable error was identified. The goal is to prevent any claim from crossing 90 days without a documented follow-up action in the last 14 days.
Tier 2 covers high-value claims in the 31-to-60-day bucket. Define a dollar threshold, for example all claims over $500, and ensure follow-up is initiated if the expected payment window has passed. Claims in this tier are not yet at risk of being uncollectable but represent enough revenue to justify proactive contact rather than waiting for the aging bucket to trigger Tier 1 urgency.
Tier 3 covers the 0-to-30-day bucket and lower-value claims in older buckets. These receive follow-up on a standard cycle, typically one contact at 30 days post-submission and another at 45 days if the claim is still unresolved. The 30-day contact is not a phone call for every claim. It is a batch status check through the payer portal or clearinghouse to identify which claims have not been adjudicated on the expected timeline.
Fix 5: Patient Statements Within 5 Days of Adjudication
Patient balance billing is the final stage of the AR cycle for most encounters. After the payer adjudicates and the patient’s cost-sharing obligation is established, the practice bills the patient for the remaining balance. How quickly that statement goes out affects both how quickly it gets paid and how likely the patient is to pay it.
Research on patient billing consistently shows that patients who receive a statement within a few days of their insurance processing the claim are more likely to pay promptly and in full than those who receive a statement weeks later. The encounter is still recent. The connection between the service and the bill is clear. The patient hasn’t assumed the bill was lost or already resolved. A 5-business-day turnaround from adjudication to statement generation is achievable with automatic statement generation triggered by payment posting and doesn’t require manual review for straightforward balances.
Patient balances that sit unstatted for two to four weeks accumulate in AR unnecessarily. They aren’t denied. They aren’t disputed. They just haven’t been billed because no one has gotten to them. Automating the trigger eliminates that delay entirely.
Fix 6: Weekly AR Aging Reviews With Escalation Thresholds
A weekly AR aging review is a 30-to-45-minute structured review of the AR aging report with three specific outputs: a list of accounts crossing into 90-plus days for immediate escalation decision, a list of new denial categories for root cause analysis, and a comparison of this week’s aging distribution against last week’s to confirm the trend is moving in the right direction.
The escalation decision for accounts crossing 90 days is one of three options: escalate to a collections partner, write off as bad debt, or authorize one final appeal investment if the balance is large enough to justify it. Practices that allow accounts to sit passively past 90 days without making one of these three decisions are not managing AR. They are allowing it to age into permanent write-offs without even extracting the option value of an escalation decision.
The weekly cadence matters because it provides the feedback loop that shows whether the process changes above are working. If days in AR is declining week over week and the 90-plus bucket is shrinking as a percentage of total AR, the process is working. If the numbers are stable or worsening, the review identifies which specific bucket or denial category is responsible and where to apply corrective effort.
The Revenue Impact of Improving Days in AR
For practices that are skeptical about the financial return on these process changes, the math is straightforward. Days in AR improvement translates directly to accelerated cash flow. For a practice generating $5 million in annual net revenue, reducing days in AR from 55 to 40 days releases approximately $206,000 in previously slow or stuck collections, based on the daily revenue rate. That is not new revenue. It is revenue the practice had already earned that is now collected faster and less of it written off.
The improvement in net collection rate that typically accompanies days in AR reduction adds further impact. A practice collecting 91% of collectible net revenue versus 95% is losing approximately $200,000 annually on $5 million in net revenue. The 4-percentage-point improvement in collection rate that comes from working denials faster, billing secondaries promptly, and catching 90-day accounts before they write off produces a real and recurring revenue improvement every year.
| Process Change | Primary Impact on AR | Secondary Benefit | Implementation Effort |
|---|---|---|---|
| 48-hour payment posting | Accurate AR data daily | Faster secondary and patient billing triggers | Low (policy + auto-posting config) |
| Automatic secondary billing | Eliminates 31-60 day secondary delay | Frees staff time for denial work | Low (system configuration) |
| 72-hour denial working standard | Reduces denial dwell time in AR | Enables root cause identification | Medium (workflow redesign + policy) |
| Root cause denial routing | Faster denial resolution per type | Reveals systemic upstream issues | Medium (routing rule configuration) |
| Tiered AR follow-up protocol | Prevents accounts from crossing 90 days | Higher staff efficiency per hour | Low (protocol document + training) |
| 5-day patient statement turnaround | Reduces patient balance AR age | Higher patient payment rates | Low (auto-statement trigger) |
| Weekly AR aging reviews | Catches deterioration before write-off | Management visibility into trends | Low (scheduled meeting + report) |
How Qualigenix Manages Accounts Receivable in Medical Billing
At Qualigenix, every one of the workflow standards described in this blog is built into our standard operating process. Payment posting runs on a 48-hour cycle. Secondary claims are triggered automatically on primary adjudication. Denials are routed by reason code at intake and worked within 72 hours. AR follow-up is tiered by aging bucket and dollar value. Weekly AR aging reviews are conducted for every client with escalation decisions made at the 90-day threshold rather than after it.
We also manage the credentialing and payer enrollment infrastructure that prevents the upstream credentialing denials that add to AR unnecessarily. A claim that denies because a provider isn’t enrolled with the payer isn’t a billing problem. It’s a credentialing problem. We manage both so that the claims reaching the AR follow-up stage are claims with legitimate reimbursement opportunities, not credentialing gaps that no amount of AR management can recover.
Our results reflect these processes operating consistently: 99% claim accuracy rate, 95% first-pass acceptance rate, an average 36-day collection cycle, and a 30% reduction in AR days for practices we take over from in-house or less systematic billing operations. We onboard new clients in as few as 6 days.
Related: What Is RCM in Medical Billing | What Is Claim Submission in Medical Billing | What Is Physician Billing
AR Management Readiness Checklist
- Payment posting standard set at 48 hours from ERA receipt with named accountability
- Automated posting rules configured for standard ERA transactions in practice management system
- Secondary insurance captured at registration for every patient with coverage
- Secondary billing triggered automatically on primary adjudication in billing system
- Denial routing configured by reason code to appropriate staff queue at intake
- 72-hour denial working standard established and tracked per staff member
- Root cause analysis run monthly on top denial reason codes
- AR follow-up protocol documented: Tier 1 (61-90 days), Tier 2 (high-value 31-60), Tier 3 (standard)
- Patient statements generated within 5 business days of insurance adjudication
- Weekly AR aging review scheduled with named owner and escalation decision framework
- 90-day threshold accounts reviewed for collection, write-off, or final appeal decision
- Days in AR tracked weekly and trended against benchmark of under 40 days
Frequently Asked Questions: Accounts Receivable Medical Billing
What is accounts receivable in medical billing?
Accounts receivable in medical billing is the total outstanding amount owed to a practice for services delivered but not yet collected, including amounts pending from payers and patients. It is tracked in aging buckets from 0-30 days through 90-plus days. Days in AR, the average number of days to collect after service delivery, is the most useful summary metric of revenue cycle health. A target of under 40 days indicates a well-functioning billing operation.
What is days in AR and what is a good benchmark?
Days in AR measures how long it takes on average to collect after service delivery, calculated by dividing total AR by average daily charges. A healthy benchmark is under 40 days. High-performing practices achieve 30 to 35 days. Days in AR above 50 indicates a systemic billing problem. Above 60 signals denial management failures or AR that has been allowed to age without intervention. Qualigenix averages a 36-day collection cycle across client practices.
What causes AR to age in medical billing?
AR ages when claims are not actively followed up, when denials sit unworked past appeal windows, when payment posting is delayed so AR doesn’t reflect actual collections, when secondary claims aren’t submitted promptly, and when patient balances aren’t followed up systematically. These are all workflow failures rather than capacity problems. Adding staff to a broken process produces marginal improvement. Fixing the process produces larger improvement at no additional cost.
How does payment posting speed affect days in AR?
Delayed payment posting inflates AR by keeping paid claims on the outstanding balance report, distorting follow-up prioritization and making AR data unreliable for management decisions. A 48-hour posting standard keeps AR data current and triggers secondary billing and patient statements on a predictable schedule. Practices posting weekly are making every follow-up decision based on data that is 5 to 10 business days stale, which means they’re contacting payers about claims that are already resolved and missing accounts that genuinely need attention.
What is the 90-day AR threshold and why does it matter?
The 90-day threshold is the point at which AR collection probability drops to approximately 20%. Every dollar past 90 days without active intervention is moving toward write-off. Practices should make an explicit decision on every account crossing 90 days: escalate to a collection partner, write off as bad debt, or authorize a final appeal investment. Allowing accounts to sit passively past 90 days is not a neutral choice. It is a decision to let collectible revenue deteriorate without extracting any of the remaining option value.
How does denial management affect accounts receivable in medical billing?
Unworked denials are the single largest contributor to AR aging. A denied claim stays in AR until it is recovered or written off, and approximately 60% of denied claims are never reworked. Those balances age through the AR buckets and become write-offs that could have been avoided. A 72-hour denial working standard with root cause routing by denial reason code is the process change that has the most direct and immediate impact on days in AR in most practices.
How can a practice reduce days in AR without hiring more staff?
Reducing days in AR without adding staff requires fixing specific workflow inefficiencies: 48-hour payment posting, automatic secondary billing on primary adjudication, 72-hour denial working with root cause routing, tiered AR follow-up by aging bucket and dollar value, 5-day patient statement turnaround, and weekly AR aging reviews with escalation decisions at the 90-day threshold. Each change redirects existing staff effort toward the actions that produce the most AR improvement rather than adding volume to an inefficient process.
What percentage of AR should be in the 0-30 day bucket?
A well-run practice keeps 65% to 75% or more of total AR in the 0-30 day bucket. When this percentage drops below 60%, AR is accumulating in older buckets, which signals claim submission delays, unworked denials, or insufficient follow-up. Monitoring the AR aging distribution weekly rather than just tracking the total AR dollar amount gives earlier warning of deteriorating performance than waiting for days in AR to tick up in the monthly report.
What is secondary billing and how does it affect AR?
Secondary billing submits a claim to a patient’s secondary insurer after the primary payer adjudicates, and delays in it are a consistent source of AR aging in the 31-to-60-day bucket. For practices with high Medicare patient panels and Medigap coverage, secondary billing delays inflate AR unnecessarily. Automatic secondary billing triggered by payment posting eliminates this delay entirely and frees staff time for denial management, which has a compounding positive effect on days in AR.
Related Resources from Qualigenix
- What Is RCM in Medical Billing
- What Is Claim Submission in Medical Billing
- What Is Physician Billing
- Provider Credentialing Services
- Payer Enrollment Services
- CAQH Profile Management
- Re-credentialing Services
- Charge Capture in Medical Billing
High Days in AR Is a Process Problem. We Fix the Process.
Qualigenix manages the full billing cycle for practices across 38+ specialties with built-in AR management standards that reduce days in AR by 30% and achieve a 36-day average collection cycle. We close the workflow gaps that age AR before they become write-offs.
Our team delivers 99% claim accuracy, a 95% first-pass acceptance rate, an average 36-day collection cycle, and a 30% reduction in AR days. We onboard in as few as 6 days.
Precision. Progress. Qualigenix.
What’s Next

Denial Management in 2026: The Top 10 Codes and the Appeal Playbook for Each
Denials cluster around a small set of codes, and each one has a different correct response. Some need a...
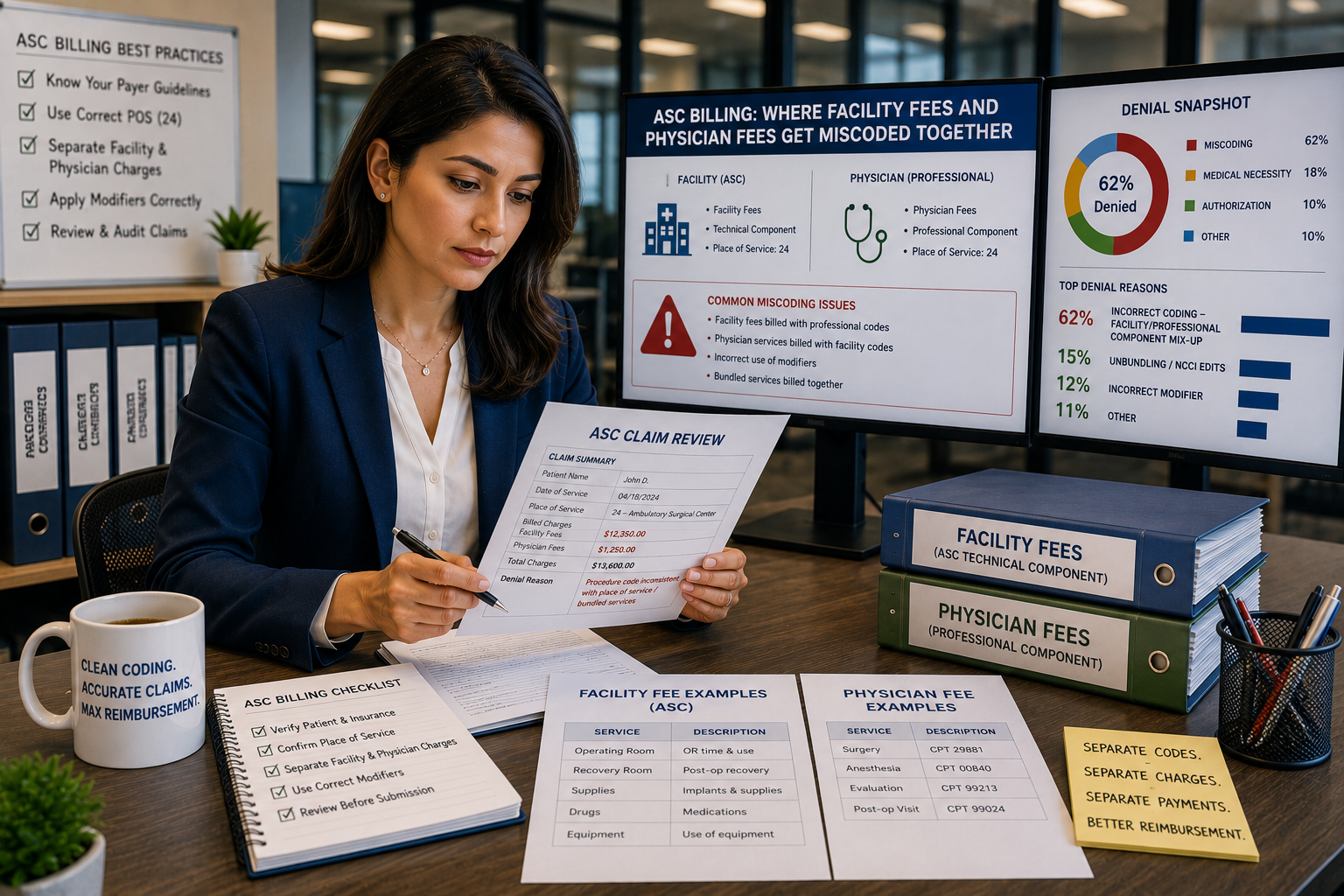
ASC Billing: Where Facility Fees and Physician Fees Get Miscoded Together
ASC facility and physician claims both go out on a CMS-1500 form with the same CPT code and place...
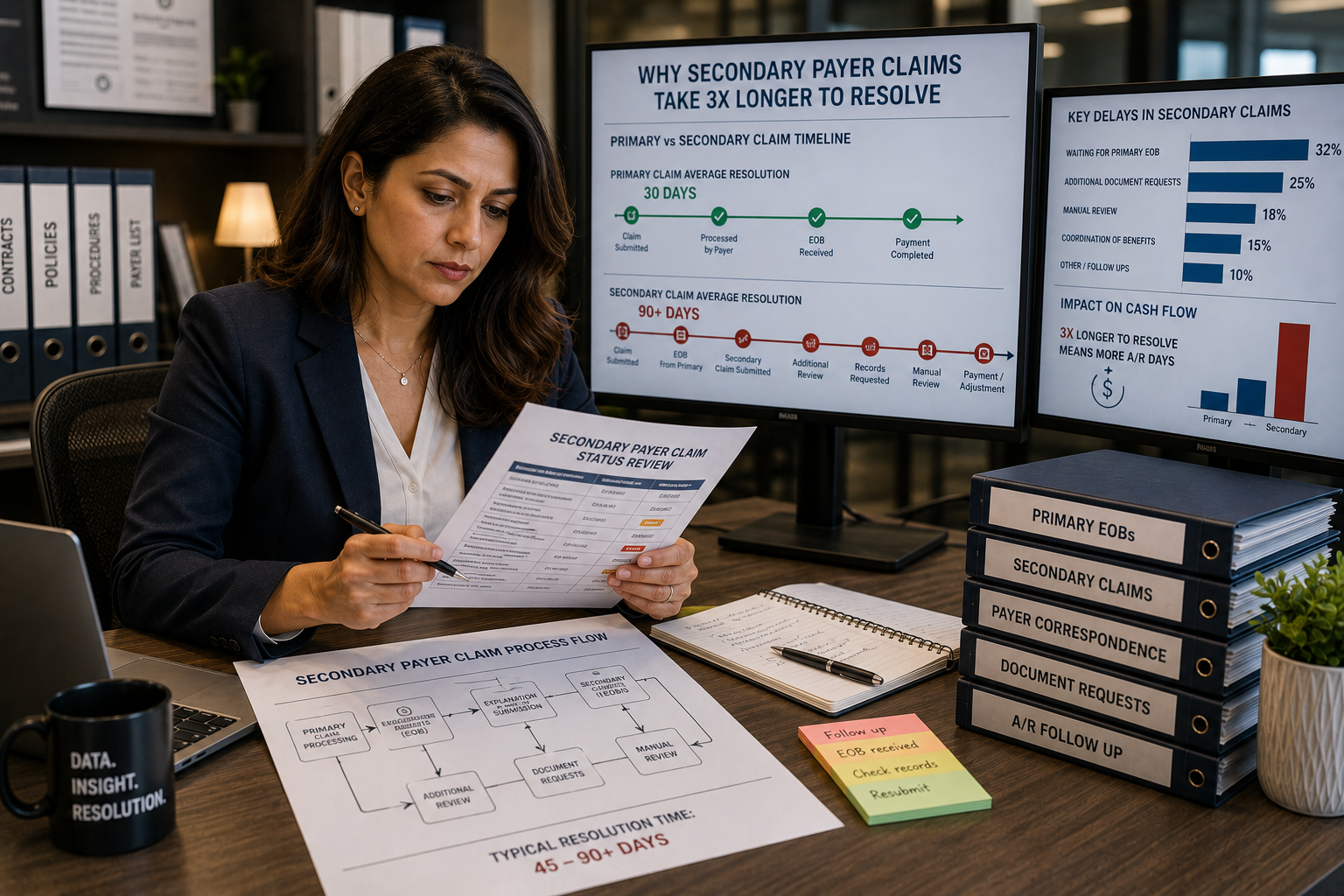
Coordination of benefits errors: why secondary payer claims take 3x longer to resolve
Secondary payer claims stall because coordination of benefits errors, wrong payer order, outdated COB records, and missing primary...