What Is Claim Submission in Medical Billing and Why Most Practices Leave Money in the Process
The Qualigenix Editorial Team consists of certified billing and coding experts with over 40 years of experience across 38+ medical specialties. Our content is rigorously researched against CMS, AMA, and payer-specific guidelines to ensure total compliance and accuracy. We apply the same elite standards to our resources as we do our client work, consistently delivering high claim accuracy and significant reductions in AR days.
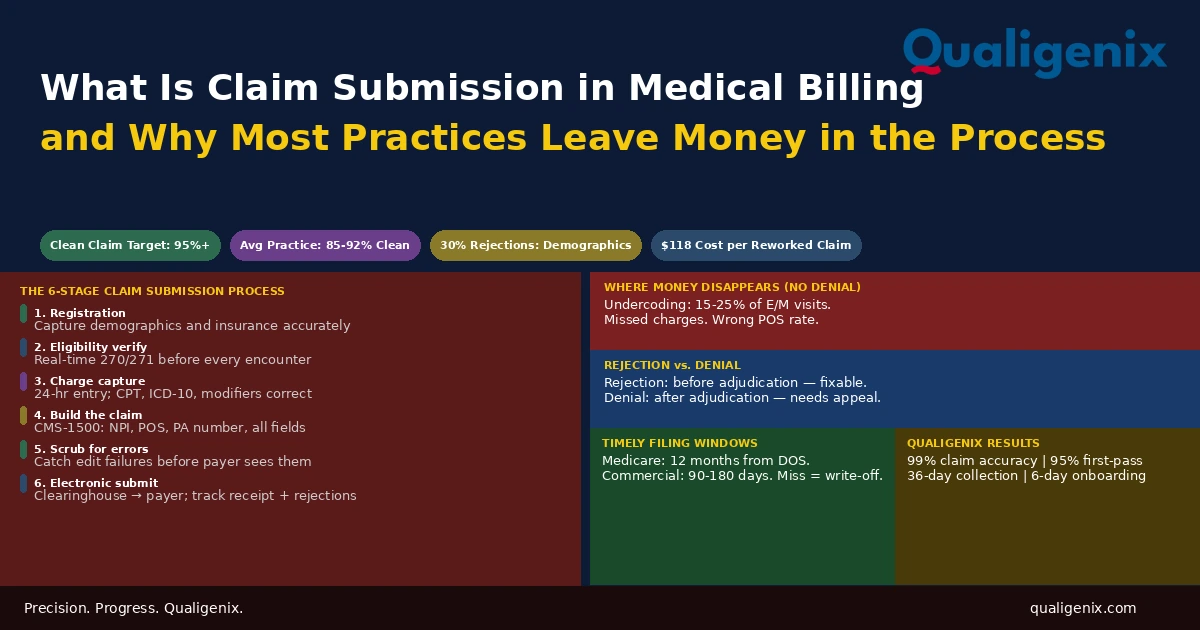
Claim submission in medical billing is the process of translating a patient encounter into a coded claim, scrubbing it for errors, and transmitting it to a payer for reimbursement. Most practices think of it as a single step. It is six. And the revenue losses that most practices attribute to payer denials are more often the product of errors introduced long before the claim reaches a payer, in registration, in coding, in charge entry, and in the submission workflow itself. Fixing those upstream errors improves collections faster than working any denial queue.
The moment a payer receives a clean claim, the hard part is mostly over. A claim that is correctly coded, completely filled out, submitted under an enrolled provider, and transmitted within the timely filing window will be paid. Not always at the rate a practice wants. Not always without a follow-up question. But paid. The system works when the inputs are right.
The inputs are rarely right by accident. They’re right because someone built a process that catches errors before the claim goes out, checks registration data before the visit, verifies eligibility before the service is delivered, and monitors charge entry to ensure nothing is missing. In practices without that process, the claim submission step is where problems that originated two or three steps earlier get discovered, either by a scrubber internally or by a payer denial externally. Either way, revenue waits.
This blog explains what claim submission actually covers, what each stage requires, where most practices consistently lose money before a denial ever happens, and what a clean claim operation looks like in a practice that has built the process correctly.
Claim submission in medical billing is the process of coding patient services, building a complete claim on the CMS-1500 or UB-04 form, scrubbing it for errors, and transmitting it electronically to a payer through a clearinghouse for reimbursement. A clean claim passes payer edits on first submission and proceeds directly to adjudication. The industry benchmark clean claim rate is 95% or higher. The average practice achieves 85% to 92%, leaving significant revenue in correction, resubmission, and rework workflows that clean submission would have prevented.
Claim Submission in Medical Billing: Key Benchmarks
| Metric | Data Point | Source |
|---|---|---|
| Industry benchmark clean claim rate | 95% or higher | MGMA revenue cycle benchmarks |
| Average practice clean claim rate | 85% to 92% | Healthcare billing industry data |
| Electronic claim reach time to payer | 24 to 48 hours via clearinghouse | Clearinghouse processing standards |
| Medicare clean claim payment timeline | 14 to 30 days | CMS claims processing standards |
| Commercial payer clean claim payment timeline | 14 to 45 days | Payer contract benchmarks |
| Medicare timely filing window | 12 months from date of service | CMS claims processing manual |
| Commercial payer timely filing window | 90 to 180 days from date of service | Payer contract standards |
| Cost to rework one rejected or denied claim | $25 to $118 | MGMA administrative cost data |
| Revenue lost to timely filing violations annually | Up to 3% of net revenue | RCM industry benchmarks |
| Claims rejected due to demographic or eligibility errors | Approx. 30% of all rejections | Clearinghouse rejection analysis |
| E/M visits billed below documented level | 15% to 25% of encounters | Coding audit benchmarks |
| Qualigenix claim accuracy rate | 99% | Qualigenix performance data |
| Qualigenix first-pass acceptance rate | 95% | Qualigenix performance data |
| Qualigenix average collection cycle | 36 days | Qualigenix performance data |
| Qualigenix AR days reduction | 30% | Qualigenix performance data |
What Claim Submission Actually Is
Claim submission is the pivot point in the medical billing revenue cycle. Before it, the practice delivers care. After it, the payer decides what to pay. Claim submission is the act of creating the record that connects those two events and presenting it to the payer in a format they can process.
That description sounds straightforward. In practice, it depends on six preceding steps being executed correctly: patient demographics captured accurately at registration, insurance eligibility verified before the visit, charges captured and coded after the encounter, a claim built on the correct form with all required fields, a scrubbing process that catches errors before transmission, and electronic delivery through a clearinghouse within the payer’s timely filing window. Each step creates either the foundation for a clean claim or a problem that the next step inherits.
Claim submission is not a billing department task. It is the output of a revenue cycle that starts at patient registration and runs through charge entry and coding before anyone in billing touches it. Most claim submission failures originate outside the billing department, in the front-end process that feeds data into the claim. Billing staff can only work with what the upstream process gives them. If the upstream process is unreliable, the claims will reflect it.
Most practices that struggle with clean claim rates focus their attention on the billing and coding steps because those are visible. The errors that show up in the denial queue often trace back to registration data that was wrong when it was entered, eligibility that was never checked, or charges that were coded from memory rather than from documentation review. Fixing the submission step without fixing the upstream steps produces incremental improvement at best.
Stage 1: Patient Registration — Where Claim Errors Begin
The first data that goes into a claim is entered at registration: the patient’s name, date of birth, insurance member ID, group number, and secondary coverage. If any of this is wrong, the claim will fail payer edits before a human reviewer ever sees it.
Approximately 30% of all claim rejections trace back to demographic or insurance data errors entered at registration. A transposed digit in a member ID. An insurance card from a prior plan year. A name that doesn’t exactly match the payer’s enrollment record. None of these errors are caught during the clinical encounter. All of them are caught by the payer’s claims system at submission.
Practices that verify insurance information at every visit, not just at initial intake, catch coverage changes before they become submission problems. A patient’s employer may have changed insurance plans since their last visit. Their Medicare Advantage plan may have changed. They may have lost coverage entirely. A real-time eligibility check before the encounter costs seconds. Resubmitting a claim that was sent to the wrong payer because coverage changed and no one checked costs days.
The Secondary Insurance Gap
Registration errors involving secondary insurance are particularly expensive because they compound. A patient with Medicare primary and a Medigap secondary has two payers that must be billed in sequence. If the secondary is missing from the registration record, the primary claim is submitted correctly and paid, but no secondary claim is ever generated. The patient’s Medigap plan never receives a claim. The copay or deductible that would have been covered sits as an open patient balance or gets written off. This is revenue the practice was contractually entitled to collect that simply disappeared because a field wasn’t populated at registration.
Stage 2: Insurance Eligibility Verification
Eligibility verification confirms the patient’s coverage is active, identifies the plan type and tier, and surfaces cost-sharing information before the encounter. It should happen before every visit, not just for new patients, and it should use real-time HIPAA 270/271 electronic transactions rather than phone IVR checks or assumptions based on prior visit data.
A claim submitted to a payer for a patient whose coverage was inactive on the date of service will deny. The denial is accurate from the payer’s perspective. The patient didn’t have active coverage. But from the practice’s perspective, the denial is the result of a front-end process failure, not a billing error. If eligibility had been verified before the visit, the practice would have known about the coverage gap and could have either collected upfront or directed the patient to resolve their insurance before receiving non-emergency care.
Warning: With Medicare Advantage enrollment now above 54% of all Medicare beneficiaries, eligibility verification for Medicare patients must identify whether the patient is on traditional Medicare or a specific Advantage plan before each visit. A claim submitted to traditional Medicare for a patient enrolled in a Medicare Advantage plan will deny. The 271 response from a real-time HETS query includes a Medicare Advantage coordination flag. Practices that skip this check generate a predictable and avoidable denial category every time an Advantage patient is billed under traditional Medicare.
Stage 3: Charge Capture and Medical Coding
After care is delivered, every billable service must be recorded and coded accurately. Charge capture is the act of recording what was done. Coding is the act of assigning CPT procedure codes, ICD-10 diagnosis codes, and any required modifiers to that record. Both must be accurate for the claim to be correct.
Two specific failures in this stage create revenue loss that doesn’t show up as a denial. The first is undercoding: assigning a lower-level CPT code than the documentation supports. A physician who consistently bills 99213 when their notes document a level that supports 99214 is leaving reimbursement on the table at every undercoded encounter. The claim gets paid. It gets paid at the wrong rate. There is no denial to work. The revenue loss is invisible without a code distribution audit.
The second is missed charges: services or procedures that were delivered but never entered into the billing system. A procedure performed during a visit that isn’t captured doesn’t generate a claim. It generates nothing. It’s not a denial. It’s a gap. For high-volume practices, even a small percentage of missed charges compounds into significant uncollected revenue over a full year.
Modifier Accuracy
Modifiers are two-digit codes that provide payers with additional context about how a service was delivered. Modifier 25 tells the payer that a significant, separately identifiable E/M service was performed on the same day as a procedure. Modifier 59 indicates a distinct procedural service. Modifier 26 identifies the professional component of a diagnostic service. Missing a required modifier or applying one incorrectly produces a denial that has nothing to do with the clinical service being appropriate.
Modifier errors are among the most consistent denial contributors in practices that don’t have a coding review step before submission. A claim for a same-day E/M and a minor procedure without modifier 25 will have the E/M bundled into the procedure payment and the separate E/M charge denied. The clinical work was done. The documentation supports billing for both. The modifier was missing. Revenue is lost.
Stage 4: Building the Claim
The coded encounter becomes a claim when it is assembled onto the correct form with all required fields populated correctly. Professional services use the CMS-1500. Facility services use the UB-04. The CMS-1500 requires the patient’s insurance information, the rendering provider’s NPI, the billing provider’s NPI and Tax ID, the date of service, the place of service code, the CPT and diagnosis codes, any modifiers, the billed amount, and the prior authorization number if the service required one.
Place of Service: The Most Underestimated Field
Place of service is a two-digit code that identifies where a service was delivered: office (11), inpatient hospital (21), outpatient hospital (22), telehealth (02 or 10), and others. Payers reimburse at different rates depending on the setting because of how overhead is handled in each context. A physician seeing patients in a hospital outpatient department bills at the facility rate (POS 22), not the office rate (POS 11), because the hospital is separately reimbursed for overhead costs.
Billing with the wrong POS code either results in the claim being paid at the wrong rate or triggers a payer edit that rejects or audits the claim. Post-payment audits that identify systematic POS errors result in recoupment demands. A practice that has been billing POS 11 for services delivered in a hospital outpatient department faces retroactive recoupment for the overpayment difference across every claim with that error during the audit period.
The Prior Authorization Number
When a service required prior authorization, the PA number must appear on the claim. A claim submitted without the PA number for a service that required one denies automatically, even if the authorization was legitimately obtained and is active. This is one of the most frustrating denial types in billing because the clinical work was authorized, the documentation supports it, and the payer would pay it. The denial is purely administrative: the PA number field was empty or incorrect on the claim.
Practices need a PA tracking system that links each active authorization number to the patient, the service, and the billing record so the PA number flows into the claim automatically rather than requiring billing staff to manually look it up for each claim. Manual lookup creates the gap where PA numbers get missed.
Stage 5: Claim Scrubbing
Before a claim is transmitted to a payer, it should pass through a claim scrubber: software that reviews the claim against payer-specific edit rules to identify errors that would cause rejection or denial. A scrubber catches missing fields, invalid code combinations, diagnosis codes that don’t support the procedure billed, modifier issues, duplicate claim indicators, and other common errors.
The value of claim scrubbing is in catching errors internally before the payer catches them. A rejection returned from a payer takes 24 to 48 hours to receive and requires correction and resubmission. A scrubber catches the same error in seconds and allows the billing team to fix it before transmission. The claim still needs to be corrected, but the correction happens in hours rather than days, and the timely filing clock doesn’t advance while waiting for a payer rejection notice.
The effectiveness of a claim scrubber depends entirely on the currency of its edit rules. A scrubber running on rules from two years ago will not catch errors introduced by code changes, payer policy updates, or new modifier requirements that have been added since the rules were last updated. Scrubber rules must be updated at minimum quarterly, and billing staff must review the scrubber’s edit library at each update to ensure new payer requirements are captured.
Stage 6: Electronic Transmission Through a Clearinghouse
Clean claims are transmitted electronically to payers through a clearinghouse. The clearinghouse receives the practice’s claims, validates them against payer-specific formatting requirements, and routes them to the appropriate payer electronically. For most commercial payers and Medicare, electronic claim submission is the required method. Paper claims are slower, more error-prone, and cost significantly more to process on both the practice and payer side.
After transmission, the clearinghouse returns a confirmation that the claim was accepted or rejected. Claims rejected by the clearinghouse have not yet reached the payer. They were returned because the claim failed the clearinghouse’s own validation before it was transmitted. These rejections must be addressed within the payer’s timely filing window.
Timely Filing: The Deadline That Closes Permanently
Every payer sets a timely filing deadline from the date of service within which a claim must be submitted. Medicare allows 12 months. Most commercial payers set windows of 90 to 180 days. Claims submitted after this window are denied for timely filing violations. Unlike most other denial types, timely filing denials cannot be appealed except in very limited circumstances involving payer-side errors that prevented submission.
Timely filing violations are almost entirely preventable. They occur when charge lag delays submission, when claims sit in a pending status waiting for information that no one actively follows up on, or when billing backlogs push submission past the deadline. A daily charge lag report and a weekly pending claims review prevent timely filing from becoming a denial category in a well-run practice.
Rejection vs. Denial: Why the Distinction Matters for Revenue Recovery
Practices often use rejection and denial interchangeably. They are operationally different in ways that matter significantly for revenue recovery.
A rejection is returned by the clearinghouse or the payer before adjudication. The payer has not evaluated whether the claim should be paid. It has determined that the claim doesn’t meet the basic requirements to be accepted for review. Rejections are correctable. The practice fixes the error and resubmits the original claim. If the correction and resubmission happen within the timely filing window, there is no permanent revenue loss from a rejection.
A denial is issued by the payer after the claim has been adjudicated. The payer reviewed the claim and determined it does not meet coverage, medical necessity, or other payment criteria. Denials require either a corrected claim or a formal appeal, depending on the denial reason. Denials that are not worked within the payer’s appeal window become permanent write-offs.
| Event | When It Happens | Recovery Path | Revenue Risk |
|---|---|---|---|
| Clearinghouse rejection | Before payer receives claim | Fix error, resubmit | Low if corrected quickly |
| Payer technical rejection | Before adjudication | Fix error, resubmit | Low to moderate depending on timely filing proximity |
| Administrative denial | After adjudication | Corrected claim or appeal | Moderate; recoverable within appeal window |
| Clinical/medical necessity denial | After adjudication | Peer-to-peer or formal appeal | Moderate to high; requires physician involvement |
| Timely filing denial | After adjudication | Very limited appeal grounds | High; usually permanent write-off |
| Credentialing denial | After adjudication | Complete enrollment; refile | High; no retroactive payment at most payers |
The Revenue That Disappears Before Any Denial Happens
Most practices measure billing performance through their denial rate. It is a useful metric but an incomplete one. The denial rate captures revenue that was attempted and refused. It doesn’t capture revenue that was never attempted because charges weren’t captured, was collected at the wrong rate because a visit was undercoded, or was delayed past collection because the submission workflow created unnecessary lag.
Undercoding: Revenue Left in the Claim
Between 15% and 25% of physician E/M visits are billed below the level the documentation supports. This isn’t fraud risk. It’s the opposite: systematic undercollection from habit, caution, or lack of coding education. A physician who bills 99213 for every established patient visit regardless of complexity is leaving reimbursement behind on every visit that could have supported 99214. At $35 to $50 difference per visit and 18 patients per day, the annual revenue impact of systematic undercoding by a single physician exceeds $30,000 in many specialties. There is no denial to work. The claim pays. It pays less than it should have.
Charge Lag: Revenue at Risk of Permanent Loss
Charge lag is the delay between when a service is delivered and when the charge is entered. Every day of charge lag advances the claim closer to the timely filing deadline without actually submitting it. For commercial payers with 90-day filing windows, a billing team that runs two weeks behind on charge entry is operating with 75 days of effective filing time, not 90. Any disruption, a system outage, a staff illness, a period of high volume, can push a subset of charges past the deadline.
A 24-hour charge entry requirement, enforced as an operational standard rather than a preference, keeps every claim well within filing windows and reduces the exposure from unexpected delays. Practices that allow charge entry to accumulate into weekly batches are carrying timely filing risk they don’t see in their reports until a batch of claims is filed late and the denials arrive.
How Credentialing Affects Claim Submission
Provider credentialing and payer enrollment are prerequisites for successful claim submission at the payer level. A claim submitted under a provider not enrolled with the payer denies automatically. The claim may be perfectly coded, completely filled out, and submitted on time. None of that matters if the rendering provider’s NPI is not recognized as an enrolled participating provider by the payer’s adjudication system.
This creates a specific and recurring risk in practices that allow new providers to start seeing patients before their payer enrollments are complete. Commercial credentialing takes 90 to 120 days. Every claim submitted under that provider to unenrolled payers during that window denies without any path to retroactive recovery at most payers. The practice delivers the care, submits the claim, receives the denial, and absorbs the loss.
Related: Provider Credentialing Services | Payer Enrollment Services
How Qualigenix Manages Claim Submission
At Qualigenix, clean claim submission is built on a process that starts before the claim is built. We manage the eligibility verification workflow, the charge lag monitoring, the coding accuracy review, the scrubber configuration, and the submission tracking that together produce a 99% claim accuracy rate and 95% first-pass acceptance rate across 38+ specialties.
We also manage the credentialing and enrollment infrastructure that makes submission work in the first place. A clean claim submitted under an enrolled provider gets paid. A clean claim submitted under an unenrolled provider doesn’t. We start provider enrollment the day a hire is confirmed, track revalidation deadlines, and maintain CAQH profiles so that the credentialing side of claim submission is never the reason a clean claim denies.
Our billing team monitors charge lag daily, runs denial root cause analysis monthly, and reviews E/M code distribution quarterly to identify undercoding patterns before they become revenue losses that compound across a year. Our results reflect this: 99% claim accuracy, 95% first-pass acceptance, 30% reduction in AR days, and an average 36-day collection cycle. We onboard new clients in as few as 6 days.
Related: What Is RCM in Medical Billing | What Is Physician Billing | CAQH Profile Management
Claim Submission Readiness Checklist
- Insurance eligibility verified before every patient visit using real-time 270/271 transactions
- Secondary insurance captured at registration and linked to the primary claim workflow
- Charge entry completed within 24 hours of every encounter
- E/M code distribution reviewed monthly per provider for undercoding patterns
- All required modifiers identified and applied at coding before claim build
- Place-of-service codes verified accurate for every service location
- Prior authorization numbers captured and linked to relevant claims
- Claim scrubber rules updated quarterly with current payer edit requirements
- Claims transmitted electronically through clearinghouse with receipt confirmation
- Rejection queue reviewed and actioned within 24 hours of clearinghouse return
- Timely filing exposure tracked weekly for pending claims approaching deadlines
- All rendering providers confirmed enrolled with payers before claim submission
Frequently Asked Questions: Claim Submission in Medical Billing
What is claim submission in medical billing?
Claim submission in medical billing is the process of coding patient services, building a complete claim on the CMS-1500 or UB-04 form, scrubbing it for errors, and transmitting it electronically through a clearinghouse to a payer for reimbursement. It is the pivot point between care delivery and payment. A clean claim that passes payer edits on first submission proceeds directly to adjudication and payment. Errors at any stage of the upstream process, from registration through coding, produce submission failures that delay or reduce revenue.
What is a clean claim in medical billing?
A clean claim contains all required information, passes payer edits on first submission, and proceeds directly to adjudication without correction or resubmission. The industry benchmark clean claim rate is 95% or higher. The average practice achieves 85% to 92%. The gap between those numbers represents claims that required correction, resubmission, or appeal at a cost of $25 to $118 each. Improving clean claim rate is the highest-return investment in billing operations because it reduces both the cost of rework and the time to payment.
What is the difference between a claim rejection and a claim denial?
A rejection is returned before adjudication when a claim fails basic data or formatting requirements. A denial is issued after adjudication when a payer determines the claim doesn’t meet coverage or medical necessity criteria. Rejections are correctable and resubmittable without revenue loss if addressed quickly. Denials require appeals or corrected claims and carry a higher risk of permanent write-off if not worked within the payer’s appeal window. Understanding which you received determines how to respond.
What information is required on a CMS-1500 claim?
A CMS-1500 requires patient name, date of birth, insurance member ID and group number, rendering provider NPI, billing provider NPI and Tax ID, date of service, place of service code, CPT codes, ICD-10 diagnosis codes, modifiers, billed charge amount, and prior authorization number if applicable. Errors or omissions in any of these fields cause the claim to reject before a reviewer sees it. Most rejections trace back to registration errors in the demographic and insurance fields.
What is a claim scrubber and why does it matter?
A claim scrubber reviews claims for errors before submission, checking for missing fields, invalid code combinations, modifier issues, and payer-specific edit failures. A scrubber catches errors in seconds before transmission, eliminating the 24-to-48-hour delay of waiting for a payer rejection notice before fixing the same error. The scrubber’s effectiveness depends on keeping its edit rules current. Outdated rules allow new error categories to pass through to payers rather than being caught internally.
What is timely filing in claim submission?
Timely filing is the deadline by which a claim must be submitted after the date of service. Medicare allows 12 months. Most commercial payers set 90 to 180 days. Claims past the deadline are denied and almost never appealable. Timely filing violations are almost entirely preventable with a 24-hour charge entry standard and weekly monitoring of pending claims approaching their filing windows. Practices that allow charge entry backlogs are carrying timely filing risk that surfaces as permanent write-offs.
How does provider credentialing affect claim submission?
Claims submitted under a provider not enrolled with the payer deny automatically regardless of coding accuracy or completeness. Commercial credentialing takes 90 to 120 days. Any claim submitted under a new provider during their enrollment window denies with no retroactive recovery path at most payers. Starting credentialing the day a hire is confirmed is the only way to minimize the window between a provider’s first patient encounter and their first billable claim.
What is secondary claim submission?
Secondary claim submission is the process of billing a patient’s secondary insurance after the primary payer has adjudicated the claim. The secondary claim includes the primary payer’s explanation of benefits. Common secondary payers include Medigap plans for Medicare patients and Medicaid for dual-eligible patients. Missing secondary claims leave collectible revenue unrecovered. Secondary billing begins with capturing secondary insurance at registration. A registration record without secondary coverage means no secondary claim is ever generated.
What is the most common reason claims are submitted incorrectly?
The most common causes of incorrect claim submission are registration errors in demographic or insurance data, missing or incorrect modifiers, diagnosis codes that don’t support the billed procedure, missing prior authorization numbers, incorrect place-of-service codes, and charge lag that pushes claims toward timely filing deadlines. Most of these errors originate upstream from the billing team. Fixing claim submission accuracy requires fixing the registration and charge entry processes that feed into the claim, not just the billing step itself.
Related Resources from Qualigenix
- Provider Credentialing Services
- Payer Enrollment Services
- What Is RCM in Medical Billing
- What Is Physician Billing
- CAQH Profile Management
- Re-credentialing Services
- Charge Capture in Medical Billing
- CMS Medicare Claims Processing Manual (CMS.gov)
Your Claims Should Be Paid on the First Submission. Ours Are.
Qualigenix manages the full claim submission process for practices across 38+ specialties, from eligibility verification and charge capture through scrubbing, electronic submission, and denial management. We close the gaps that cost practices money before a denial ever happens.
Our team delivers 99% claim accuracy, a 95% first-pass acceptance rate, an average 36-day collection cycle, and a 30% reduction in AR days. We onboard in as few as 6 days.
Precision. Progress. Qualigenix.
What’s Next

Underpayments vs. Denials: Which One Is Draining Your Practice More?
Denials get attention because they stop cash flow outright. Underpayments don’t stop anything, they just quietly shrink it....
Your AR Days Are Too High. Here’s What That Actually Means for Revenue
AR days over 50 usually means claims are aging into buckets that are hard to collect, not that payers...
From 6-Day Onboarding to First Clean Claim: How Qualigenix Transitions Practices
Most billing transitions take 30 to 90 days and stall revenue in the gap. Qualigenix compresses that timeline to...