ABA Billing for Growing Practices: What Changes When You Add More BCBAs and RBT
The Qualigenix Editorial Team consists of certified billing and coding experts with over 40 years of experience across 38+ medical specialties. Our content is rigorously researched against CMS, AMA, and payer-specific guidelines to ensure total compliance and accuracy. We apply the same elite standards to our resources as we do our client work, consistently delivering high claim accuracy and significant reductions in AR days.
ABA billing is already more complex than general medical billing at any size. When a practice adds BCBAs and RBTs, that complexity multiplies across every active payer contract, every supervision assignment, and every patient authorization. The billing infrastructure that works for three BCBAs and ten RBTs will not hold at eight BCBAs and thirty RBTs without deliberate process changes.
Most ABA practice owners understand that billing is complicated. The CPT codes are specific. The authorization requirements are demanding. Payers audit supervision documentation with more scrutiny than most other specialties. But when a practice is small, these challenges are manageable. One billing coordinator can track authorizations for 20 active patients. One BCBA can confirm their supervision logs before the end of the week. The system holds because the volume is low enough that gaps get noticed quickly.
Then the practice grows. A second location opens. Two new BCBAs join. The RBT count doubles. Suddenly there are 60 active patients, four BCBAs with staggered payer credentialing timelines, and 25 RBTs generating daily session notes that all need to flow correctly into a billing system that’s still running the way it did when the practice had a quarter of the volume. That’s when ABA billing problems stop being occasional and start being systemic.
This blog covers exactly what changes in ABA billing as a practice scales, where the breakdowns happen, and what a billing infrastructure that actually holds at growth looks like.
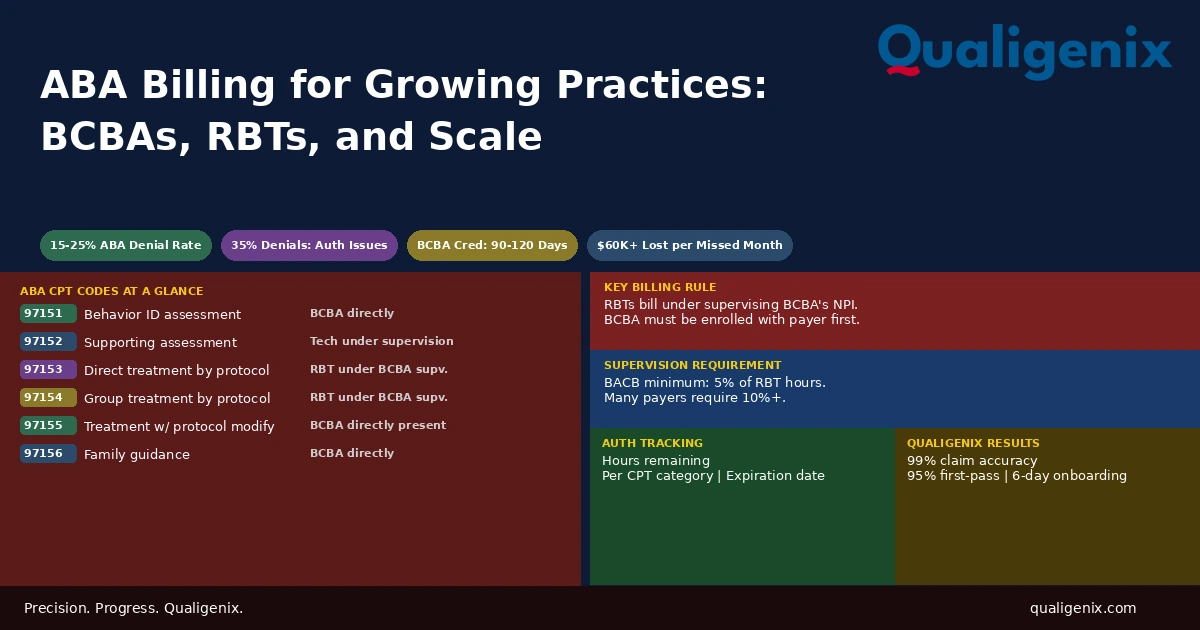
ABA billing uses CPT codes 97151 through 97158 to distinguish between assessment, supervision, and direct treatment services. In a growing practice, billing complexity increases because each new BCBA must be individually credentialed with every payer, RBT services can only be billed under a credentialed supervising BCBA, supervision documentation must meet both BACB standards and individual payer requirements, and authorizations must be tracked per patient per BCBA per payer with no overlap or overrun.
ABA Billing at Scale: Key Numbers
| Metric | Data Point | Source |
|---|---|---|
| Commercial payer BCBA credentialing timeline | 90 to 120 days per payer | Payer credentialing benchmarks |
| ABA claim first-submission denial rate | 15% to 25% | ABA billing industry surveys |
| ABA denials related to authorization issues | Up to 35% of denials | ABA revenue cycle data |
| ABA denials related to supervision documentation | Up to 20% of denials | ABA payer audit data |
| BACB minimum supervision requirement | 5% of supervised RBT hours per billing period | BACB Ethics Code |
| CAQH re-attestation requirement per BCBA | Every 120 days | CAQH ProView requirements |
| Typical ABA authorization period | 3 to 6 months per cycle | Payer authorization policies |
| Authorization renewal lead time needed | 14 to 21 days before expiration | ABA practice management benchmarks |
| Revenue lost per uncredentialed BCBA month | $20,000 to $60,000+ depending on caseload | ABA revenue analysis |
| Payer applications required per new BCBA | 8 to 15 per provider | Multi-payer practice analysis |
| Qualigenix first-pass acceptance rate | 95% | Qualigenix performance data |
| Qualigenix claim accuracy rate | 99% | Qualigenix performance data |
| Qualigenix average collection cycle | 36 days | Qualigenix performance data |
| Qualigenix client onboarding time | 6 days | Qualigenix operations data |
What Makes ABA Billing Different From the Start
Before covering what changes at scale, it helps to understand why ABA billing is structurally more complex than most medical billing even at a small practice size. The complexity isn’t incidental. It’s built into how the CPT codes work and how payers evaluate ABA claims.
ABA CPT codes are provider-type-specific. The code used on a claim signals not just what service was delivered, but who delivered it and under what supervision arrangement. CPT 97153 says a technician delivered direct treatment under a BCBA’s supervision. CPT 97155 says the BCBA was present and actively modifying the protocol. CPT 97151 is an assessment conducted by the BCBA directly. Each code carries its own documentation requirements, its own authorization category, and its own payer-specific rules about what constitutes acceptable billing.
RBTs cannot bill insurance. They have no billing credentials. Every session an RBT delivers must be billed under the supervising BCBA’s NPI and credentials. If that BCBA is not credentialed with the patient’s payer, the session cannot be billed at all. The BCBA’s credentialing status is the billing prerequisite for every RBT in their supervision caseload.
Most payers also treat ABA as a specialty requiring specific medical necessity documentation and prior authorization. Authorizations specify which CPT codes are approved, how many hours per week or per month, and for what diagnosis. Claims that fall outside any of those parameters deny without exception. That authorization structure is manageable for 15 patients. It’s a full-time tracking function for 80.
The ABA CPT Code Structure Every Billing Team Must Know
Getting ABA billing right at any size starts with understanding which code applies to which service context. Misapplying these codes is the most common source of ABA claim errors, and the errors don’t always produce immediate denials. Some result in post-payment audits and recoupment requests months after services were delivered.
| CPT Code | Service Description | Who Delivers | Unit |
|---|---|---|---|
| 97151 | Behavior identification assessment | BCBA directly | 15 min |
| 97152 | Behavior identification supporting assessment | Technician under BCBA supervision | 15 min |
| 97153 | Adaptive behavior treatment by protocol | Technician under BCBA supervision | 15 min |
| 97154 | Group adaptive behavior treatment by protocol | Technician under BCBA supervision | 15 min |
| 97155 | Adaptive behavior treatment with protocol modification | BCBA directly present | 15 min |
| 97156 | Family adaptive behavior treatment guidance | BCBA directly | 15 min |
| 97157 | Multiple-family group adaptive behavior treatment guidance | BCBA directly | 15 min |
| 97158 | Group adaptive behavior treatment with protocol modification | BCBA directly present | 15 min |
The distinction between 97153 and 97155 trips practices up consistently. 97153 is for RBT-delivered sessions where the BCBA is supervising but not present in the room during the session. 97155 is for sessions where the BCBA is directly there and actively changing the protocol in real time. Billing 97155 for sessions where the BCBA was not directly present is an overcoding error. Billing 97153 for sessions where the BCBA was present and modifying the protocol is an undercoding error. Both create problems, one financial and one compliance-related.
What Changes When a Second BCBA Joins
When a practice adds its second BCBA, the billing impact is immediate and often underestimated. The new BCBA needs to be credentialed with every payer the practice participates with before they can supervise RBTs and have those sessions billed. That process takes 90 to 120 days per payer for commercial plans and 60 to 90 days for Medicare if applicable.
During that window, the new BCBA can work. They can assess patients, develop treatment plans, and supervise RBTs. But sessions delivered under an uncredentialed BCBA cannot be billed to the payers where enrollment is still pending. The revenue gap that results is not a billing error. It’s a credentialing timing failure that could have been avoided if the application process had started the day the hire was confirmed.
A second issue appears at the patient assignment level. Patients who transfer from the original BCBA to the new BCBA require authorization updates at most payers. The authorization was issued to the original BCBA as the responsible clinician. When a new BCBA takes over a case, the payer needs to know about the change. Billing sessions under the new BCBA’s NPI against an authorization still associated with the original BCBA is a documentation mismatch that produces denials or audit flags.
Warning: Practices that allow new BCBAs to begin supervising RBT sessions before credentialing is confirmed with the patient’s payer are generating unbillable claims. These sessions can’t be recovered retroactively with most payers. The financial impact accumulates silently until billing staff notice the denial pattern and trace it back to an enrollment that was never completed before the BCBA started supervising.
What Changes When the RBT Count Doubles
Adding RBTs doesn’t create new credentialing obligations since RBTs don’t bill under their own credentials. But it creates two compounding problems: supervision documentation burden and authorization volume.
Supervision Documentation at Volume
Every RBT session billed under a BCBA’s credentials must be supported by supervision documentation showing the BCBA’s active oversight of that RBT’s work. The BACB requires a minimum of 5% supervision of total RBT hours. Many commercial payers require 10% or more. Some payers specify the type of supervision contact: direct observation, review of session data, or individual supervision meeting.
When a BCBA is supervising four RBTs each delivering 25 hours per week of direct treatment, that BCBA is responsible for documenting supervision across 100 hours of RBT service per week. At 5%, that’s a minimum of 5 documented supervision hours per week. At 10%, it’s 10. Each contact must be documented with the date, duration, RBT name, patients reviewed, and nature of the contact.
When the practice grows to six BCBAs each supervising five RBTs, the volume of supervision documentation being generated weekly is enormous. If documentation quality drops because BCBAs are rushed, or if records aren’t retained in a format that supports payer audits, the practice is accumulating audit risk across hundreds of sessions per week. Payers conducting retrospective audits of ABA claims request this documentation routinely. Practices that can’t produce it face recoupment demands on paid claims.
The Supervision Ratio Risk at Scale
As practices grow and add RBTs faster than BCBAs, supervision ratios become harder to maintain. A BCBA who was comfortably supervising four RBTs at a 10% supervision ratio starts to struggle when their caseload expands to seven RBTs without additional BCBA support. The math changes. The hours needed to meet the required ratio increase. The BCBA’s schedule doesn’t accommodate it. Supervision documentation gets thinner. Payers auditing the ratio see a gap and initiate a review.
Growing practices need a supervision ratio monitor built into their operations. This isn’t just a compliance function. It’s a billing function. Claims that can’t be supported by adequate supervision documentation are claims at risk of recoupment. And in ABA billing, recoupment requests can reach back months or even years if the documentation gap is systemic.
Authorization Tracking: The Highest-Risk Function at Scale
Prior authorization is required by most payers for ABA services. Each authorization covers a specific patient, specifies which CPT codes are approved, sets a maximum number of hours per week or per month, and runs for a defined period, typically three to six months. When the authorization expires or when hours are exhausted, claims for subsequent sessions deny automatically.
For a small practice with 20 active patients, an authorization spreadsheet is manageable. A billing coordinator can review it weekly and flag expirations in advance. For a practice with 80 active patients spread across four BCBAs and multiple payers, each with different authorization periods and different hour limits by CPT category, a spreadsheet stops being adequate. Authorizations expire unnoticed. RBTs deliver sessions against exhausted hour banks. The practice bills. The claims deny. By the time the denial pattern is investigated, several weeks of sessions may be unrecoverable.
Authorization tracking for ABA billing must be managed at three levels simultaneously: total approved hours remaining for each patient, approved hours remaining per CPT code category (since some payers authorize 97153 hours separately from 97155 hours), and the expiration date of the authorization. Tracking only one of these three dimensions misses the other two ways a claim can deny on authorization grounds.
Authorization Renewals and the 14-Day Rule
Most payers require an updated clinical assessment and a new authorization request when the current authorization expires. The renewal process takes time. Payers may request additional clinical documentation before approving the renewal. If a practice submits the renewal request after the current authorization has already expired, there will be a gap period where sessions are delivered without active authorization.
Sessions delivered during an authorization gap deny. Some payers allow bridge periods with documented pending renewal requests. Most don’t. The standard that works is initiating every authorization renewal 14 to 21 days before the current authorization expires. At scale, this means the billing team has multiple renewals in process at any given time, each with its own payer, its own clinical documentation requirement, and its own pending timeline to track.
BCBA Turnover: The Billing Disruption Nobody Plans For
Provider turnover in an ABA practice isn’t just an HR event. Every BCBA departure creates an immediate billing question for every patient in that BCBA’s caseload: who is the supervising provider of record going forward, and is that provider credentialed with the patient’s payer?
If the incoming BCBA is already credentialed with the payer, the transition is administratively complex but billingwise manageable. Authorization records need to reflect the new BCBA. Supervision documentation needs to identify the new supervisor for every session going forward. Claims need to reflect the new rendering provider NPI. All of this can be handled without a billing gap if the transition is planned.
If the incoming BCBA is new to the practice and not yet credentialed with the patient’s payer, the billing gap is unavoidable until credentialing completes. For every patient assigned to that BCBA, RBT sessions cannot be billed to the payer during the credentialing window. This is why BCBA credentialing must start the moment a hire is confirmed, not after they’ve settled into the role and started building a caseload.
The departing BCBA also needs to be terminated from payer panels. Leaving an inactive BCBA on active payer rosters creates compliance exposure and potential issues if their credentials are accidentally used on claims after their departure.
Building a Billing Infrastructure That Holds at Growth
The practices that scale ABA billing successfully share one characteristic: they treat billing infrastructure as a priority that grows alongside clinical operations, not a back-office function that catches up when it gets overwhelmed. Here’s what that infrastructure requires.
A Live Credentialing Tracker for Every BCBA
Every active BCBA in the practice needs an enrollment status record showing which payers they are credentialed with, when each credentialing was approved, and when re-credentialing is due. This tracker must also show which payers have pending applications for BCBAs currently in the enrollment process, so the billing team knows which patients and payers cannot be billed for sessions under that BCBA yet.
An Authorization Management System by Patient and Code
Authorization tracking must show, for every active patient: the current authorization number, the approving payer, the approved CPT codes, the approved hours per code category per week or month, the hours used to date, the hours remaining, and the expiration date. Renewals should be flagged automatically at 21 days out. Any patient whose authorization is within two weeks of expiration without a renewal in process is a billing risk.
Supervision Documentation Standards Across All BCBAs
All BCBAs in the practice must document supervision using the same format and the same level of detail. Practices where each BCBA has their own informal documentation style will struggle during payer audits because the records don’t meet a consistent standard. Supervision logs must capture date, time, duration, BCBA name and credentials, RBT name, patients reviewed, type of contact, and any clinical decisions made. They must be retained in a retrievable format for the lookback period each payer requires.
How Qualigenix Supports ABA Billing for Growing Practices
At Qualigenix, we work with ABA practices at multiple stages of growth, from practices adding their second BCBA to established groups managing 10 or more providers across multiple locations. We understand that ABA billing isn’t just medical billing with different codes. It requires knowledge of BACB supervision standards, payer-specific ABA medical necessity criteria, authorization structures, and the credential-to-billing chain that ties every RBT session to a specific BCBA’s enrollment status.
Our credentialing team starts BCBA enrollment applications the day a new hire is confirmed. We manage CAQH profiles, submit payer applications in priority order by patient volume, and track every application through to approval. When a BCBA joins, we build the credentialing timeline against their anticipated start date and flag any payers where the enrollment will still be pending when they begin supervising.
Our billing team manages ABA CPT code accuracy, authorization tracking by patient and by code category, supervision documentation review before claim submission, and denial management with root cause analysis. When a denial pattern appears, we trace it to the source: an expired authorization, a supervision documentation gap, a credentialing status mismatch, or a code assignment error, and fix the upstream process, not just the individual claim.
Our results hold at scale: 99% claim accuracy rate, 95% first-pass acceptance rate, 30% reduction in AR days, and an average 36-day collection cycle. We onboard new clients in as few as 6 days.
Related services: Provider Credentialing | Payer Enrollment | CAQH Profile Management
ABA Billing Readiness Checklist for Growing Practices
- BCBA credentialing started for every new hire on day of offer acceptance
- CAQH profile built and completed before any payer applications are submitted for new BCBAs
- Live tracker showing which BCBAs are credentialed with which payers and pending enrollment status
- RBT supervision assignments only made to BCBAs with active enrollment for the patient’s payer
- Authorization tracker showing hours used, hours remaining, and expiration date per patient per CPT category
- Authorization renewal process initiated 14 to 21 days before every expiration
- Supervision documentation logged per BACB standards and retained in audit-ready format
- Monthly supervision ratio audit comparing BCBA supervision hours to RBT session hours per BCBA
- CPT code selection reviewed against session type: RBT-delivered vs. BCBA-present protocol modification
- BCBA departure protocol includes immediate payer termination notification and incoming BCBA enrollment start
Frequently Asked Questions: ABA Billing
What is ABA billing?
ABA billing is the process of coding and submitting insurance claims for applied behavior analysis services using CPT codes 97151 through 97158. Each code maps to a specific service type and provider context. The BCBA must be credentialed and enrolled with the payer. RBT services bill under the supervising BCBA’s credentials. Prior authorization is required by most payers, and supervision documentation must support every claim that bills technician-delivered services.
What CPT codes are used for ABA billing?
The primary ABA billing CPT codes are 97151 (behavior identification assessment by BCBA), 97152 (supporting assessment by technician), 97153 (direct treatment by technician under supervision), 97154 (group treatment by technician), 97155 (treatment with protocol modification by BCBA), 97156 (family guidance by BCBA), 97157 (multiple-family group guidance), and 97158 (group treatment with protocol modification by BCBA). Each code carries its own documentation requirements and provider type specifications.
Can an RBT bill insurance directly for ABA services?
No. RBTs cannot bill insurance directly. All RBT-delivered services must be billed under the supervising BCBA’s credentials and NPI. The BCBA must be credentialed and enrolled with the patient’s payer before any session supervised by that BCBA can be billed. If the BCBA is not enrolled, the claim denies regardless of how accurately the session was documented or coded.
What supervision documentation is required for ABA billing?
Supervision documentation must include the date and duration of the contact, the supervising BCBA’s name and credentials, the RBT’s name, the patients or programs reviewed, and the type of supervision contact. BACB requires a minimum of 5% of total RBT service hours be supervised. Many payers require 10% or more and specify the acceptable forms of supervision contact. Documentation must be retained in a format that supports payer audit requests.
Why do ABA billing claims deny more often than other specialties?
ABA claims deny at 15% to 25% on first submission due to the complexity of authorization requirements, supervision documentation standards, credential-specific CPT code rules, and payer-by-payer variation in ABA medical necessity criteria. Authorization issues account for up to 35% of ABA denials. Supervision documentation gaps account for up to 20%. The combination makes ABA one of the highest-denial-rate specialties in behavioral health billing.
What happens to ABA billing when a BCBA leaves the practice?
When a BCBA leaves, all RBT sessions in that BCBA’s supervision caseload must transition to another credentialed BCBA before billing continues. If the incoming BCBA is not yet credentialed with the patient’s payer, sessions cannot be billed during the credentialing window. Authorization records must be updated to reflect the new supervising BCBA. The departing BCBA must be terminated from payer panels to avoid compliance exposure.
How does prior authorization work for ABA billing?
Most payers require prior authorization for ABA services specifying approved CPT codes, maximum hours per week or month, and an authorization period of three to six months. Claims exceeding authorized hours or submitted after authorization expiration deny immediately. Growing practices must track authorization status at three levels: total hours remaining, hours remaining per CPT code category, and expiration date. Renewal requests should be submitted 14 to 21 days before expiration.
What is the difference between 97153 and 97155 in ABA billing?
CPT 97153 is for direct treatment delivered by an RBT under BCBA supervision when the BCBA is not present in the session. CPT 97155 is for sessions where the BCBA is directly present and actively modifying the treatment protocol in real time. Using 97155 when the BCBA was not present is overcoding. Using 97153 when the BCBA was present modifying the protocol is undercoding. Both are errors, one creating compliance risk and the other leaving revenue on the table.
Does a BCBA need to be credentialed separately with each insurance payer?
Yes. Each BCBA must be individually credentialed and enrolled with each payer before ABA services can be billed under their NPI with that payer. A BCBA credentialed with one payer is not automatically enrolled with others. Commercial payer credentialing takes 90 to 120 days per payer. For a practice with 10 active payer contracts adding a new BCBA, that’s up to 10 simultaneous applications running in parallel before the BCBA can fully supervise billable sessions across all payers.
Should an ABA practice outsource its billing as it grows?
Most growing ABA practices benefit from outsourcing billing because ABA-specific coding, supervision ratio tracking, authorization management, and BCBA credentialing require specialized knowledge that general billing staff don’t typically have. ABA billing errors compound at scale. A billing partner with ABA experience manages code-level accuracy, authorization limits, supervision documentation review, and credentialing timelines simultaneously, which is the combination that prevents the systemic denial patterns that emerge as patient and provider counts increase.
Related Resources from Qualigenix
- Provider Credentialing Services
- Payer Enrollment Services
- CAQH Profile Management
- Re-credentialing Services
- Insurance Credentialing for Multi-Provider Practices
- Telehealth Provider Credentialing
- BACB Ethics Code and Supervision Standards (BACB.com)
Your ABA Practice Is Growing. Your Billing Should Keep Up.
Qualigenix manages ABA billing, BCBA credentialing, authorization tracking, and supervision documentation review for growing applied behavior analysis practices. We close the gaps before they become denial patterns.
Our team delivers 99% claim accuracy, a 95% first-pass acceptance rate, an average 36-day collection cycle, and a 30% reduction in AR days. We onboard in as few as 6 days.
Precision. Progress. Qualigenix.
What’s Next

Underpayments vs. Denials: Which One Is Draining Your Practice More?
Denials get attention because they stop cash flow outright. Underpayments don’t stop anything, they just quietly shrink it....
Your AR Days Are Too High. Here’s What That Actually Means for Revenue
AR days over 50 usually means claims are aging into buckets that are hard to collect, not that payers...
From 6-Day Onboarding to First Clean Claim: How Qualigenix Transitions Practices
Most billing transitions take 30 to 90 days and stall revenue in the gap. Qualigenix compresses that timeline to...