Why Your Clean Claim Rate Is Stuck Below 95% – How to Fix It
The Qualigenix Editorial Team consists of certified billing and coding experts with over 40 years of experience across 38+ medical specialties. Our content is rigorously researched against CMS, AMA, and payer-specific guidelines to ensure total compliance and accuracy. We apply the same elite standards to our resources as we do our client work, consistently delivering high claim accuracy and significant reductions in AR days.

The HFMA benchmark for high-performing billing operations is 98%. Most practices sit between 75–85%. The gap comes down to five fixable problems: front-end eligibility failures, coding errors, missing prior authorizations, timely filing misses, and no claim scrubbing before submission. Fix these systematically and most practices hit 95%+ within 90 days.
Your revenue cycle has a number you should check right now. Not your denial rate, not your AR days. Your clean claim rate: the percentage of claims your payers accept and pay on the first try, without a single correction.
The Healthcare Financial Management Association (HFMA) sets 98% as the benchmark for top-tier billing performance. According to 2026 benchmark data from Revenue Synergy, the minimum for efficient operations is 95%. Most independent and group practices sit between 75% and 85%.
That gap isn’t a rounding error. It’s delayed cash, rework labor, write-offs, and AR days past 45. Every cause of a low clean claim rate is preventable. Here’s what’s keeping your rate stuck and how to fix each one.
A clean claim rate below 95% is caused by five things: front-end eligibility errors, CPT coding mistakes, missing prior authorizations, timely filing violations, and no pre-submission claim scrubbing. More than 60% of denials are front-end errors that happen before a claim reaches the payer. Fix the front end first. That’s where the money goes.
Clean Claim Rate Benchmarks at a Glance (2026)
| Metric | Industry Average | Top Performers | Source |
|---|---|---|---|
| Clean Claim Rate | 75–85% | 97–99% | HFMA / Revenue Synergy 2026 |
| Minimum efficient rate | 95% | 98%+ | HFMA Benchmark 2026 |
| Denial Rate (Average) | 8–12% | Below 5% | Revenue Synergy 2026 |
| Days in AR (Average) | 30–40 days | Under 25 days | Revenue Synergy 2026 |
| Annual lost revenue (unrecovered denials) | $30,000 avg per practice | — | Malakos Healthcare Solutions 2025 |
| Front-end preventable denials | 60%+ of all denials | — | Pana Healthcare Solutions 2026 |
| Prior auth as denial trigger | 35% of practices | — | Experian Health State of Claims 2025 |
| AI scrubbing improvement in first-pass rate | — | Up to 30% improvement | Medical Billers and Coders 2026 |
| Practices with rejection rate above 15% | Some practices | — | Malakos Healthcare Solutions 2025 |
| Staff time spent on prior auth processes | 95% of practices report increase | — | AHA / Conifer Health 2025 |
| Practices still reviewing claims manually | ~50% | — | RevenueMemo Industry Report 2026 |
| Qualigenix clean claim accuracy | — | 99% | Qualigenix Healthcare |
Reason 1: Front-End Eligibility Errors Are the Biggest Drain
More than 60% of denied claims come from front-end errors: problems that happened before the claim was ever submitted. A misspelled name, a wrong date of birth, an outdated insurance ID, or an incorrect group number kicks a claim back immediately.
Eligibility errors hit just as hard. If a patient’s coverage has lapsed, changed, or doesn’t cover a specific service, and your team doesn’t catch that before the appointment, you’ve already lost the claim. The fix is real-time 270/271 eligibility verification, run at scheduling and again at check-in. Not once. Twice. Payer coverage can change between those two touchpoints.
Practices that run real-time eligibility checks see the largest single improvement in clean claim rate. It’s the highest-return fix on this list, and it costs less to implement than the rework it prevents.
What’s the #1 fix for a low clean claim rate? Run real-time eligibility verification at two points: scheduling and check-in. This single change addresses more than 60% of preventable denials. These are front-end errors that happen before a claim reaches the payer.
Reason 2: Coding Errors That Slip Through Every Year
The AMA updates CPT codes annually. In 2025, those updates changed codes across surgical, E/M, and several specialty categories. Practices that don’t refresh coding protocols after each update submit claims with deleted codes, wrong modifiers, or bundled procedures that payers reject automatically.
The most common coding problems aren’t obscure edge cases. They’re unbundled procedures that should be billed together, missing modifiers on bilateral services, and upcoding or downcoding patterns that trigger payer edit flags. These are systemic failures, not one-off mistakes. The same coder making the same error on 50 claims a week is what keeps a clean claim rate stuck at 82%.
A quarterly coding audit by specialty fixes this. Audit against your top 20 CPT codes by volume. Flag where your denial-by-code report shows repeating patterns. Then retrain on those specific codes, not a broad annual refresher, but targeted correction on the actual problem codes for your payer mix.
Reason 3: Prior Authorization Is Being Tracked Too Late
Experian Health’s 2025 State of Claims survey found that 35% of practices identify prior authorization as a top denial trigger. According to the American Hospital Association, 95% of practices report staff spending more time on prior authorization processes than in previous years. It’s still not working.
The problem isn’t that practices skip prior auth entirely. They track it too late. An authorization valid at scheduling may expire before the appointment. A procedure added during the visit may fall outside the original auth. In specialty care, prior auth requirements have expanded: procedures that didn’t need pre-approval two years ago now do.
The fix is a proactive authorization log that flags expiring approvals 30 days in advance. Pair it with automated workflows that trigger auth requests by procedure code and payer, and the reactive scramble that causes most prior auth denials disappears.
How do prior authorization issues affect clean claim rate? Experian Health’s 2025 data shows 35% of practices cite prior auth as a top denial trigger. The three most common failure points: expired authorizations, missing auth for newly required procedures, and auth that doesn’t match the rendered service.
Reason 4: Timely Filing Deadlines Are Being Missed
Each payer sets its own claim submission window. The range runs from 15 days to one year from the date of service, and it varies by payer type. Medicare, Medicaid, and commercial payers all operate differently. Miss the window and you get an automatic denial. There’s no appeal path for a timely filing violation. The revenue is gone.
This is a systems failure, not a people failure. Practices without automated deadline tracking rely on billing staff to remember payer-specific windows across dozens of contracts. That doesn’t scale. A clearinghouse-integrated deadline tracker that flags claims approaching their window eliminates this denial category entirely.
Warning: Timely filing denials are the only category where no recovery is possible. Once the filing window closes, that claim cannot be appealed or resubmitted. Build automated deadline tracking into your billing workflow before this becomes a pattern.
Reason 5: Claims Are Going Out Without Pre-Submission Scrubbing
About 50% of providers still review claims manually, according to 2026 industry data from RevenueMemo. Manual review misses the exact errors automated scrubbers catch: payer-specific edit rules, modifier compatibility, place-of-service mismatches, and eligibility gaps that a human reviewer won’t spot in a queue of 200 claims.
AI-driven claim scrubbing catches eligibility, coding, and modifier errors before transmission. Medical Billers and Coders 2026 data shows it improves first-pass rates by up to 30%. The scrubber needs payer-specific edits configured. A generic scrubber is better than nothing, but a payer-specific one is what moves the needle.
The difference between a practice at 82% and one at 97% is pre-submission scrubbing. The claim doesn’t reach the payer until it’s clean. That one workflow change restructures the entire revenue cycle.
Does claim scrubbing really make a difference? Yes, measurably. AI-driven scrubbing improves first-pass claim rates by up to 30%. Practices that move from manual review to payer-specific automated scrubbing see clean claim rate improvements within the first billing cycle after implementation.
What a 99% Clean Claim Rate Looks Like in Practice
At Qualigenix, we work with 275+ practices across 38+ specialties. Practices that come to us with clean claim rates in the low 80s share the same profile: manual eligibility checks, no pre-submission scrubbing, and prior auth tracking that runs behind the appointment schedule.
Our process starts with a full billing audit that identifies exactly which of the five problems above are driving denials, broken down by payer, provider, and code. We implement real-time 270/271 eligibility verification, payer-specific claim scrubbing rules, and a proactive prior auth tracking workflow. Practices typically see clean claim rate gains within 60 to 90 days. Most hit 95%+ before the quarter closes.
We deliver 99% claim accuracy, a 95% first-pass acceptance rate, and a 30% reduction in AR days. We onboard in as few as 6 days.
In-House Billing vs. Qualigenix: Clean Claim Rate Comparison
| Metric | Typical In-House Billing | Qualigenix |
|---|---|---|
| Clean claim rate | 75–85% | 99% |
| First-pass acceptance | Varies | 95% |
| Pre-submission scrubbing | Often manual or generic | Payer-specific automated |
| Eligibility verification | Often once (at scheduling) | Real-time: scheduling + check-in |
| Prior auth tracking | Reactive | Proactive: 30-day advance flag |
| AR days | Often 45+ days | 30% reduction from baseline |
| Onboarding time | N/A | As few as 6 days |
| Specialties supported | Varies | 38+ specialties |
10-Point Clean Claim Rate Checklist for 2026
Run your billing workflow against this checklist. Any “No” is a direct cause of revenue leakage.
- Real-time eligibility verification runs at scheduling AND check-in
- Patient demographics are confirmed at every visit, not assumed from the last visit
- CPT codes are audited against 2026 AMA code updates for your top specialties
- Prior authorization tracking log flags expiring approvals 30 days in advance
- Billing team has payer-specific prior auth requirements documented by procedure
- Timely filing deadlines are tracked by payer with automated alerts before windows close
- Pre-submission claim scrubbing is configured with payer-specific (not generic) edit rules
- Denial reports are reviewed weekly by payer, provider, and code
- Coding team receives targeted retraining on top denial codes, not broad annual refreshers
- Clean claim rate, first-pass rate, and AR days are tracked on a live dashboard
Frequently Asked Questions
What is a good clean claim rate in medical billing?
The HFMA benchmark for high-performing operations is 98%. A clean claim rate of 95% or higher is the minimum for efficient billing. Most practices sit between 75% and 85%, which means revenue is bleeding out through rework, write-offs, and extended AR days every single billing cycle.
How do I calculate my clean claim rate?
Divide the number of claims accepted on first submission without errors by total claims submitted, then multiply by 100. Example: 185 clean claims ÷ 200 total claims × 100 = 92.5%. Pull 90 days of data for the most accurate baseline reading.
What’s the difference between a rejection and a denial?
Rejections come back before adjudication. They’re fixable immediately and can be corrected and resubmitted same day. Denials are post-adjudication and require a formal appeals process, which takes longer and costs more staff time. Clean claim rate tracks rejections. Denial rate tracks what happens after adjudication.
How quickly can a practice improve its clean claim rate?
With the right billing partner and front-end eligibility protocols in place, most practices see clean claim rate gains within 60 to 90 days. AI-driven claim scrubbing improves first-pass rates by up to 30%, often visible within the first billing cycle after it’s configured.
What financial impact does a low clean claim rate have?
Practices lose an average of $30,000 annually on denied claims that are never resubmitted. Beyond write-offs, a low clean claim rate pushes AR days past 45, adds rework labor hours, and lowers net collection rate. A 10-percentage-point improvement in clean claim rate shows up in cash flow within one billing quarter.
Does outsourcing medical billing improve clean claim rate?
Yes, consistently. Professional billing partners run payer-specific scrubbing rules, keep coding teams current on annual CPT updates, and use real-time eligibility tools most in-house teams don’t have. They routinely hit clean claim rates above 95%, compared to the 75–85% average for in-house billing.
A Free Audit Shows You Exactly Where Your Rate Is Dropping
Most practices that come to us don’t know which of the five problems is costing them the most. After the audit, they do. Qualigenix has worked with 275+ practices across 38+ specialties. We break down your denial rate by payer, provider, and code — and show you the dollar figure attached to each one.
We deliver 99% claim accuracy, a 95% first-pass acceptance rate, a 30% reduction in AR days, and onboarding in as few as 6 days.
Precision. Progress. Qualigenix.
What’s Next
Denial Management in 2026: The Top 10 Codes and the Appeal Playbook for Each
Denials cluster around a small set of codes, and each one has a different correct response. Some need a...
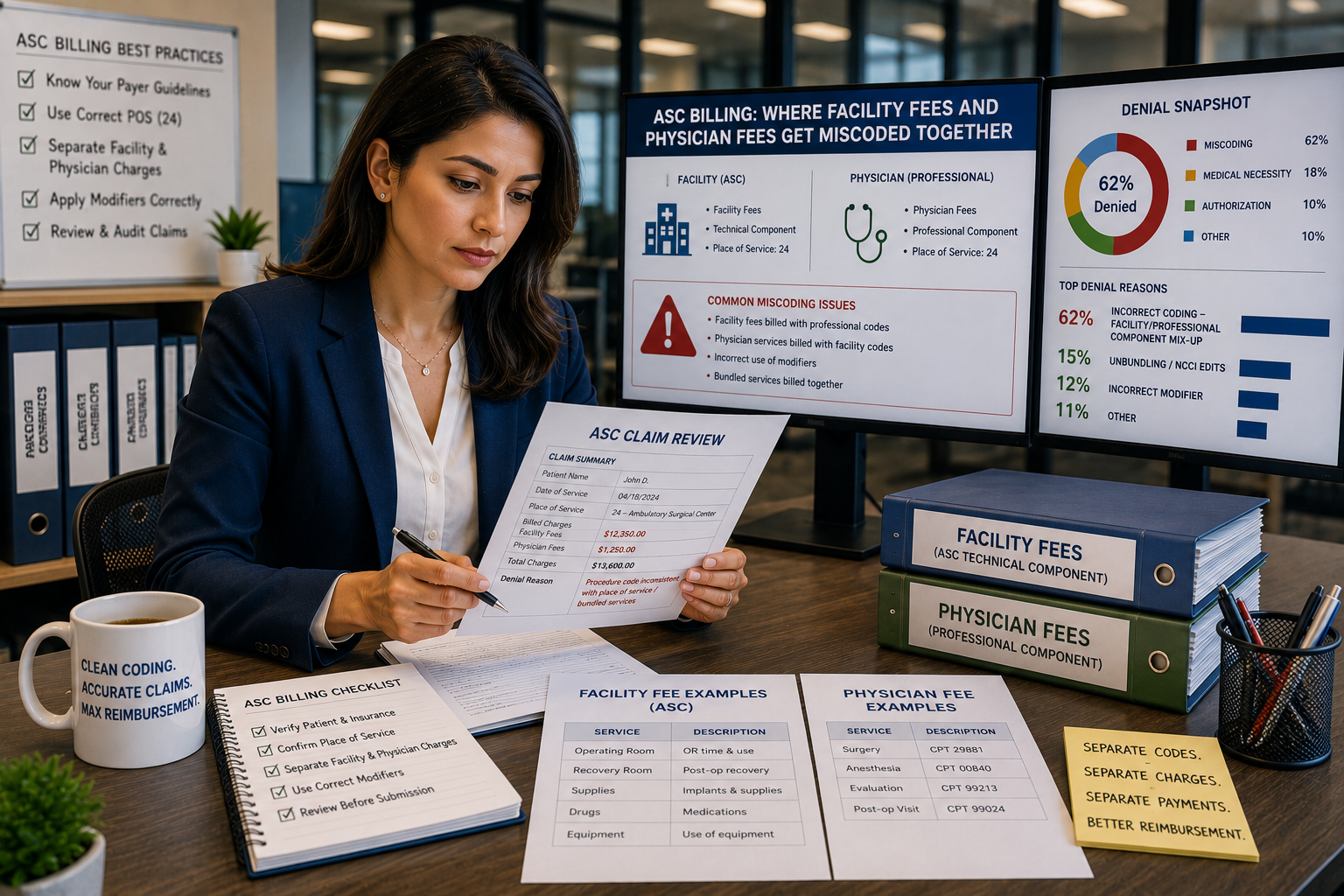
ASC Billing: Where Facility Fees and Physician Fees Get Miscoded Together
ASC facility and physician claims both go out on a CMS-1500 form with the same CPT code and place...
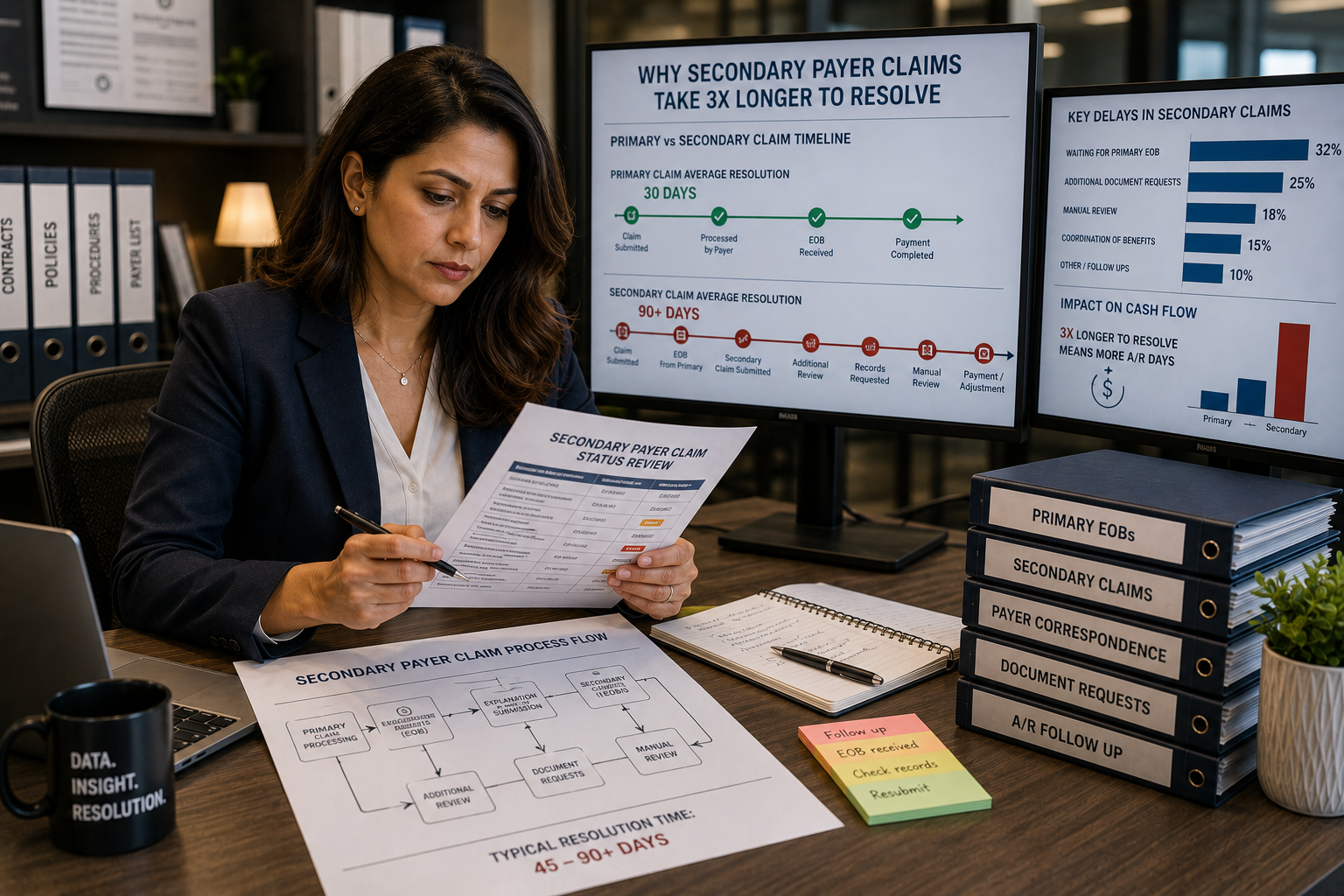
Coordination of benefits errors: why secondary payer claims take 3x longer to resolve
Secondary payer claims stall because coordination of benefits errors, wrong payer order, outdated COB records, and missing primary...