What Is Medicaid Billing and How It Actually Works
The Qualigenix Editorial Team consists of certified billing and coding experts with over 40 years of experience across 38+ medical specialties. Our content is rigorously researched against CMS, AMA, and payer-specific guidelines to ensure total compliance and accuracy. We apply the same elite standards to our resources as we do our client work, consistently delivering high claim accuracy and significant reductions in AR days.
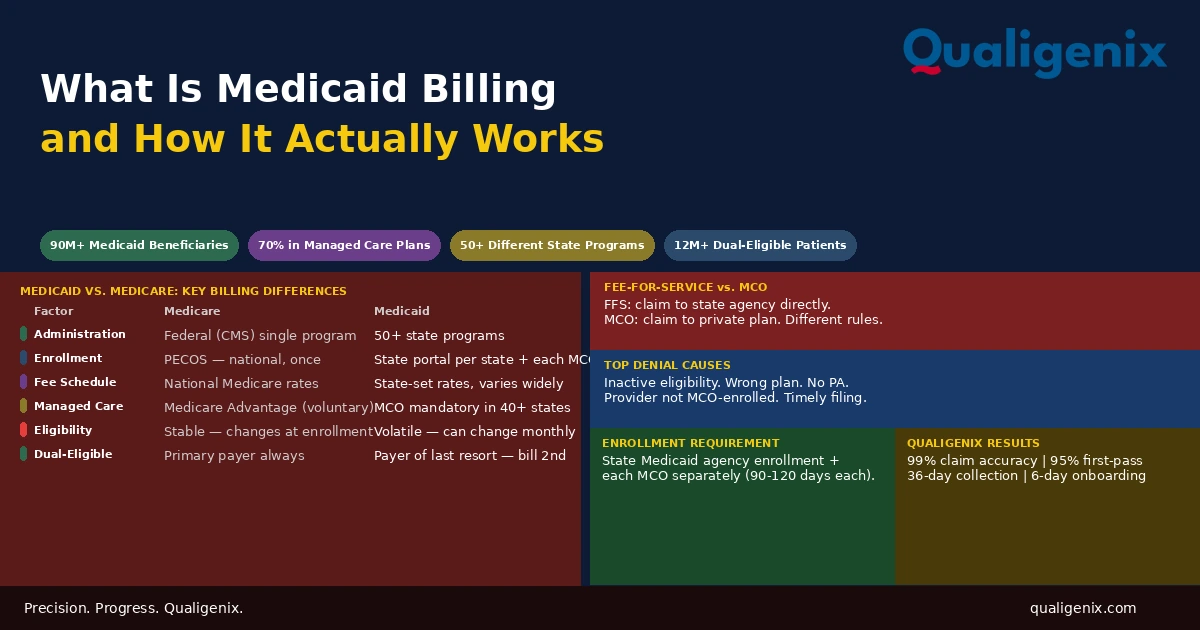
Medicaid billing is not a single process. It is 50 or more different processes, one per state, each with its own fee schedule, enrollment requirements, managed care structure, prior authorization rules, and timely filing windows. A provider credentialed with Medicare can bill Medicare claims anywhere in the country. A provider enrolled in one state’s Medicaid program cannot bill another state’s program without separate enrollment there. Practices that treat Medicaid billing the same as commercial or Medicare billing will produce Medicaid denials at higher rates than any other payer in their mix.
Medicare is a federal program. The rules are national. The fee schedule is national. The enrollment process runs through one federal system, PECOS. Learn Medicare billing once and it works the same in Texas as it does in New York.
Medicaid is not that. Medicaid is a joint federal-state program where the federal government sets broad eligibility and coverage standards and each state administers its own program. Texas Medicaid and New York Medicaid are not the same payer. They have different enrollment portals, different fee schedules, different managed care structures, different prior authorization requirements, and different denial reason codes. A billing team that knows how to bill one state’s Medicaid program knows how to bill that state’s program. The next state is a different education.
This blog explains what Medicaid billing is, how the fee-for-service and managed care models work differently, what enrollment requires at both the state and plan level, where practices consistently generate avoidable Medicaid denials, and what it takes to build a billing process that handles Medicaid correctly across every patient and every plan.
Medicaid billing is the process of submitting claims to a state Medicaid program or Medicaid managed care organization for covered services provided to Medicaid-eligible patients. Unlike Medicare, Medicaid is administered separately by each state with its own rules, fee schedule, and enrollment system. Approximately 70% of Medicaid enrollees nationally are in managed care plans, meaning most Medicaid claims go to private managed care organizations rather than directly to the state agency. Providers must be enrolled separately with each managed care plan they participate with, in addition to the state program itself.
Medicaid Billing: Key Numbers and Program Data
| Metric | Data Point | Source |
|---|---|---|
| Total Medicaid and CHIP enrollment (2026) | Over 90 million beneficiaries | CMS enrollment data |
| Medicaid enrollees in managed care nationally | Approximately 70% | MACPAC Medicaid managed care data |
| States with mandatory Medicaid managed care | Over 40 states | CMS managed care state data |
| Dual-eligible beneficiaries (Medicare + Medicaid) | Over 12 million | CMS dual-eligible data |
| Medicaid as share of US healthcare spending | Approximately 19% | CMS National Health Expenditure data |
| Medicaid timely filing window range by state | 90 to 365 days from date of service | State Medicaid program policies |
| Medicaid managed care credentialing timeline | 90 to 120 days per plan | Managed care credentialing benchmarks |
| Most common Medicaid billing denial cause | Eligibility verification failure | Medicaid claims denial analysis |
| Number of distinct state Medicaid programs | 50 states plus DC and territories | CMS Medicaid program directory |
| Medicaid managed care plans per state (average) | 3 to 8 plans per state depending on program | MACPAC managed care enrollment data |
| Qualigenix first-pass acceptance rate | 95% | Qualigenix performance data |
| Qualigenix claim accuracy rate | 99% | Qualigenix performance data |
| Qualigenix average collection cycle | 36 days | Qualigenix performance data |
| Qualigenix client onboarding time | 6 days | Qualigenix operations data |
What Makes Medicaid Billing Different From Everything Else
The fundamental distinction between Medicaid and every other payer a practice works with is that Medicaid is a state program, not a national one. The federal government provides funding and sets minimum standards through the Social Security Act and CMS guidance. But the program design, the benefits package, the payment rates, the managed care structure, and the administrative rules are all state-level decisions within that federal framework.
This means that billing a Medicaid patient in California requires knowing California’s Medicaid program, which is called Medi-Cal. Billing a Medicaid patient in Texas requires knowing Texas Medicaid, which operates under its own Vendor Drug Program and managed care structure. Billing a Medicaid patient in Florida requires understanding Florida Medicaid’s statewide managed care program. None of these programs works exactly like the others.
The practical consequence for billing is that every assumption a billing team brings from commercial or Medicare billing must be verified against state-specific Medicaid rules before it’s applied to a Medicaid claim. Prior authorization requirements that don’t apply in one state may be mandatory in another. Fee schedules that are reasonable for a service in one state may be substantially lower in another. Enrollment processes that take two months in one state may take four in another. Medicaid billing requires state-specific knowledge, not general billing expertise applied uniformly.
Fee-for-Service Medicaid vs. Managed Care: Two Different Billing Workflows
The first thing to know about any specific Medicaid claim is whether the patient is in the state’s fee-for-service program or enrolled in a Medicaid managed care plan. These are not interchangeable. They require completely different billing workflows, go to completely different entities, and operate under different rules even within the same state.
Fee-for-Service Medicaid Billing
In the fee-for-service model, the state Medicaid agency acts as the direct payer. The provider submits a claim to the state’s claims processing system, the state adjudicates it against the state Medicaid fee schedule, and the state pays the provider directly. The state’s fee schedule sets the reimbursement rate for every covered service. Unlike commercial payers, where a practice negotiates a contract rate, Medicaid fee-for-service rates are set by the state and are not negotiable for most providers.
Fee-for-service Medicaid is still the primary model for certain populations and services in most states, including many long-term services and supports, certain waiver programs, and populations not yet transitioned to managed care. For practices treating these populations, understanding the state’s fee schedule and the state’s specific billing requirements is the foundation of accurate fee-for-service Medicaid billing.
Medicaid Managed Care Billing
In managed care Medicaid, the state contracts with private managed care organizations to administer benefits for enrolled members. The state pays the MCO a monthly capitation rate per enrolled member. The MCO then manages provider networks, sets reimbursement rates for in-network providers, processes claims, and handles prior authorization for covered services.
From a billing perspective, this changes everything. The claim goes to the MCO, not the state. The MCO’s fee schedule applies, not the state’s. The MCO’s prior authorization requirements apply, not the state’s. The MCO’s network requirements apply, which means the provider must be credentialed and enrolled with each MCO separately. A provider enrolled with the state Medicaid program for fee-for-service billing is not automatically enrolled with any MCO. Each MCO enrollment is a separate credentialing application with a separate 90-to-120-day processing timeline.
Warning: A Medicaid patient may be enrolled in a managed care plan whose network does not include your practice. Submitting a claim to the fee-for-service program for a patient enrolled in an MCO will produce a denial because the MCO is responsible for that patient’s claims. Submitting to the MCO when the provider is not enrolled with that MCO will also deny. Medicaid eligibility verification must confirm not just that a patient has Medicaid coverage but which specific plan they are enrolled in and whether the provider is in-network with that plan before the encounter.
Medicaid Eligibility: The Most Volatile Verification in Billing
Medicaid eligibility is more volatile than any other payer type a practice encounters. Commercial insurance typically changes at plan enrollment periods, usually once a year. Medicare enrollment, once established, is stable for years. Medicaid eligibility can change monthly based on changes in a patient’s income, employment, household size, or other qualifying factors.
A patient who had active Medicaid coverage at their appointment last month may have lost it this month because their household income increased, because they got a job, or because a redetermination was triggered by a change the state identified in their records. They may not even know their coverage has lapsed. They will present at the front desk with the same Medicaid card they’ve always carried. Without a real-time eligibility check, the claim goes out to an inactive enrollment and denies.
The eligibility verification process for Medicaid must confirm three things at every visit: that the patient’s Medicaid coverage is currently active, which specific plan the patient is enrolled in (fee-for-service or a specific MCO), and whether the provider is currently in-network with that plan. Missing any of these three confirmations creates a billing error that shows up as a denial after the service has been delivered.
Post-Pandemic Medicaid Redeterminations
The continuous enrollment protection that kept Medicaid enrollees from losing coverage during the COVID-19 public health emergency ended in 2023. States have been processing Medicaid redeterminations since then, reviewing eligibility for their full Medicaid populations. Millions of individuals who had been continuously enrolled without recertification have had their eligibility reviewed, and a significant number have been disenrolled due to income changes, failure to respond to redetermination notices, or administrative processing errors.
For practices with significant Medicaid patient panels, the redetermination period has created a persistent eligibility verification challenge. Patients who have been Medicaid patients for years may now have lapsed or changed coverage. Practices that updated their eligibility verification processes in response to this environment have maintained their Medicaid billing accuracy. Those that haven’t have seen elevated denial rates on Medicaid claims that trace back to eligibility status changes the practice wasn’t tracking.
Medicaid Provider Enrollment: State Agency and Managed Care Plans
Medicaid provider enrollment operates on two parallel tracks in managed care states. Both must be complete before a provider can bill Medicaid patients in that state without denials.
State Medicaid Agency Enrollment
Every provider who wants to participate in a state’s Medicaid program must be enrolled with the state Medicaid agency. This enrollment is completed through the state’s provider enrollment portal, which varies by state. Some states use a unified online system. Others use paper applications or a combination. The information required is consistent with other provider enrollment processes: NPI, licensure, Tax ID, specialty, practice address, and attestation of any adverse history.
State Medicaid enrollment timelines vary significantly. Some states process enrollments in 30 to 45 days. Others take 90 to 120 days. Some states have backlogged enrollment queues that extend timelines further. A provider who sees Medicaid patients before their state enrollment is active will have every Medicaid claim denied for the duration of the enrollment gap, with no retroactive payment at most states once enrollment is approved.
Medicaid Managed Care Plan Enrollment
In states where most Medicaid patients are in managed care, state Medicaid agency enrollment is necessary but not sufficient. The provider must also be credentialed and enrolled separately with each MCO whose members they want to treat as in-network.
Each MCO conducts its own credentialing review. Most commercial MCOs use CAQH for some or all of their verification, but state-specific requirements often supplement CAQH data with additional forms and documentation. The credentialing timeline is 90 to 120 days per plan. A state with four active MCOs requires four separate credentialing applications, each processed independently, each taking up to four months.
For a new provider joining a practice in a managed care Medicaid state, this means the full timeline from enrollment start to in-network status across all relevant plans can extend to six months or longer if applications are not submitted simultaneously. Every Medicaid patient seen during that window who is enrolled in an MCO the provider isn’t yet credentialed with generates an uncompensated encounter that cannot be recovered retroactively.
Related: Provider Credentialing Services
Medicaid Fee Schedules: What Practices Need to Understand
Medicaid reimburses at lower rates than Medicare and most commercial payers for most services in most states. This is a structural feature of the program, not an anomaly. Medicaid fee-for-service rates are set by state legislatures as part of the state budget process, and they reflect the political and fiscal constraints of each state’s Medicaid budget. In some states, Medicaid rates for certain services are 50% to 60% of Medicare rates. In others, specific specialty services may be closer to Medicare parity.
Understanding Medicaid fee schedules matters for two billing-related reasons. First, the practice needs accurate expected payment data for Medicaid claims to identify when a payment is incorrect. A Medicaid payment that is 20% below the fee schedule rate is a contractual underpayment, the same as any other payer. Second, managed care MCOs set their own rates for in-network providers, and these rates are negotiable within the range the state contract allows. MCO rates may be higher or lower than the state fee-for-service schedule depending on the plan and the market.
Managed Care Rate Negotiation
Unlike fee-for-service Medicaid where rates are fixed by the state, MCO participation agreements include negotiated rates. These negotiations are similar in structure to commercial payer contracting, though the leverage dynamics are different. Providers with high Medicaid patient volumes or specialty services that are in short supply in a managed care network may have more negotiating position with Medicaid MCOs than with commercial payers.
Practices that accept the first rate offer from a Medicaid MCO without review leave money on the table in the same way they would with any commercial payer. The rate negotiation step is often skipped because Medicaid enrollment feels like an administrative process rather than a contracting opportunity. It is both.
Prior Authorization in Medicaid Billing
Prior authorization requirements for Medicaid vary significantly between the fee-for-service program and individual managed care plans, and they vary between states. A service that requires PA under one state’s Medicaid program may not require it under another’s. A service that is covered without PA under the state fee-for-service program may require PA under an MCO in the same state.
The administrative challenge this creates is that a practice with a significant Medicaid patient panel may be managing PA requirements across the state fee-for-service program and three or four MCOs simultaneously, each with different PA lists, different clinical criteria, and different submission processes. There is no single Medicaid PA checklist that covers all of these. PA requirements must be verified for each service under each specific Medicaid payer for each patient.
Missing prior authorization for a Medicaid-covered service produces the same outcome as it does with any payer: the claim denies. The difference with Medicaid is that the appeal process varies by state and by plan, timely filing windows may be shorter than commercial payers, and the administrative cost of the appeal often approaches or exceeds the Medicaid reimbursement amount for lower-value services.
Dual-Eligible Patients: Medicaid as Payer of Last Resort
Over 12 million Americans are enrolled in both Medicare and Medicaid. These dual-eligible patients represent the highest-cost, highest-need population in both programs. For billing purposes, the coordination rule is straightforward: Medicare is always the primary payer. Medicaid is the payer of last resort.
This means a claim for a dual-eligible patient must be submitted to Medicare first. Medicare adjudicates and pays its portion. The remaining balance, which may include the deductible, copayment, or coinsurance, is then submitted to Medicaid as a secondary claim. Medicaid may pay all, part, or none of the remaining balance depending on the state’s Medicaid coverage rules for dual-eligible patients and the specific cost-sharing structure that applies.
Practices that bill dual-eligible patients to Medicaid first violate the payer of last resort rule and will receive a Medicaid denial. The denial is correct. Medicaid does not cover services for dual-eligible patients until Medicare has been billed and has adjudicated. Reversing the billing order is not a fixable error on the Medicaid claim. It requires starting over with Medicare primary submission, which may create timely filing issues depending on how much time has passed.
Dual-eligible patients also have a more complex managed care landscape than single-coverage Medicaid patients. Many states have specific managed care programs for dual-eligible patients, including Dual Eligible Special Needs Plans (D-SNPs) that coordinate both Medicare and Medicaid benefits. For practices with high dual-eligible patient populations, understanding the coordination rules for each specific plan type is a billing-critical knowledge area.
Medicaid Billing Denial Patterns and How to Prevent Them
Medicaid billing denial patterns are predictable. The same categories of errors appear consistently across practices that haven’t built Medicaid-specific process controls. Understanding the pattern allows the practice to prevent the denial before it occurs.
| Denial Type | Root Cause | Prevention |
|---|---|---|
| Inactive eligibility on date of service | Coverage lapsed between visits without verification | Real-time eligibility check before every visit |
| Wrong plan — claim to FFS for MCO patient | Eligibility check didn’t identify MCO enrollment | Confirm specific plan, not just Medicaid status |
| Provider not enrolled with MCO | Credentialing not complete for that specific plan | Start MCO credentialing on hire confirmation |
| Missing prior authorization | PA not obtained or PA for wrong plan type | Verify PA requirements per service per plan |
| NPI not linked to Medicaid enrollment | NPI in claim doesn’t match state enrollment record | Confirm NPI consistency at enrollment and billing |
| Timely filing violation | State or plan deadline passed before submission | Track Medicaid-specific timely filing by state and plan |
| Dual-eligible billed in wrong order | Medicaid billed before Medicare primary | Verify dual-eligibility and bill Medicare first |
| Non-covered service billed to Medicaid | Service not on state Medicaid covered services list | Check state coverage list before billing |
Medicaid Revalidation: The Enrollment Renewal Most Practices Miss
Like Medicare, Medicaid requires providers to periodically revalidate their enrollment. Federal regulations require revalidation at least every five years for most Medicaid provider types. States may require more frequent revalidation for certain provider categories or in response to compliance concerns.
Missing a Medicaid revalidation deadline results in deactivation of Medicaid billing privileges, producing the same consequence as missing a Medicare revalidation: all Medicaid claims submitted after the deactivation date deny until the revalidation is completed and billing privileges are restored. For practices in states where Medicaid represents a significant portion of patient volume, a revalidation lapse can produce a material revenue disruption.
The difference between Medicaid and Medicare revalidation tracking is that Medicaid revalidation must be managed at the state level for each state the provider is enrolled in, rather than through a single federal system. A provider enrolled in multiple state Medicaid programs has multiple independent revalidation deadlines to track.
How Qualigenix Manages Medicaid Billing
At Qualigenix, we manage Medicaid billing as a payer-specific discipline, not an extension of general billing practices. We maintain state-specific knowledge of Medicaid program structures, fee schedules, managed care plan configurations, and prior authorization requirements for the states where our clients operate. When a new provider joins a practice, we initiate both state Medicaid agency enrollment and MCO credentialing simultaneously, in priority order by patient volume, so the billing gap between start date and active Medicaid enrollment is as short as possible.
Our eligibility verification workflow confirms Medicaid plan enrollment at the encounter level, not just Medicaid status. We identify MCO enrollment, confirm provider in-network status with the specific plan, and flag any dual-eligible patients for Medicare primary billing. We track Medicaid-specific timely filing deadlines by state and plan alongside commercial payer windows so Medicaid claims are never written off for a deadline that could have been met.
Our denial management team routes Medicaid denials to staff with state-specific Medicaid knowledge rather than general denial working queues. Medicaid denial codes are state-specific and require different resolution paths than commercial or Medicare denials. Working them effectively requires knowing the specific state’s system, not just general medical billing appeal procedures.
Our results hold across Medicaid-heavy practices: 99% claim accuracy rate, 95% first-pass acceptance rate, 36-day average collection cycle, and 30% reduction in AR days. We onboard new clients in as few as 6 days.
Related: What Is RCM in Medical Billing | Verify Medicare Eligibility for Providers
Medicaid Billing Readiness Checklist
- Real-time eligibility check before every Medicaid patient visit confirming active coverage and specific plan
- Billing workflow identifies whether patient is in fee-for-service or managed care before claim build
- Provider enrolled with state Medicaid agency for all states where Medicaid patients are seen
- Provider credentialed and enrolled with all active Medicaid MCOs in each operating state
- MCO credentialing started simultaneously with state enrollment for every new provider hire
- Prior authorization requirements verified per service per Medicaid plan before encounter
- Dual-eligible patients flagged for Medicare primary billing before Medicaid secondary submission
- Medicaid-specific timely filing deadlines tracked by state and by MCO plan
- NPI linkage verified in state Medicaid enrollment record matches NPI used on claims
- Medicaid revalidation deadlines tracked per state with renewal initiated 90 days in advance
- State Medicaid covered services list confirmed for any service not routinely billed
- Medicaid denials routed to staff with state-specific Medicaid billing knowledge
Frequently Asked Questions: Medicaid Billing
What is Medicaid billing?
Medicaid billing is the process of submitting claims to a state Medicaid program or Medicaid managed care organization for reimbursement of services provided to Medicaid-eligible patients. Unlike Medicare, Medicaid is administered by each state under broad federal guidelines, meaning billing requirements, fee schedules, enrollment processes, and managed care structures vary by state. Practices must understand the specific Medicaid program rules in each state where they operate rather than applying a single national billing standard.
How does Medicaid billing differ from Medicare billing?
Medicare is a single federal program with national billing rules. Medicaid is a state-federal partnership where each state administers its own program with distinct fee schedules, enrollment systems, managed care structures, and prior authorization requirements. A provider enrolled with Medicare can bill Medicare in any state. Medicaid enrollment must be completed separately in each state. In managed care states, enrollment must be completed with each MCO separately, adding 90 to 120 days per plan.
What is Medicaid managed care billing?
Medicaid managed care billing occurs when a state contracts with private managed care organizations to administer Medicaid benefits, meaning most Medicaid claims go to the MCO rather than the state agency. Approximately 70% of Medicaid enrollees nationally are in managed care. Providers must be separately credentialed and enrolled with each MCO in addition to the state program. The MCO’s fee schedule, prior authorization rules, and network requirements apply, not the state’s fee-for-service program rules.
How does a provider enroll in Medicaid for billing?
Medicaid provider enrollment is completed through each state’s Medicaid agency portal with the provider’s NPI, licensure, Tax ID, practice address, and specialty. State enrollment timelines range from 30 to 120 days depending on the state. In managed care states, separate credentialing applications must be submitted to each MCO, each taking 90 to 120 days. Starting all applications simultaneously on the day a hire is confirmed is the only way to minimize the billing gap.
How does Medicaid eligibility work and why does it change frequently?
Medicaid eligibility is determined by each state based on income, family status, disability, and other factors, and it can change monthly based on changes in the patient’s circumstances. A patient with Medicaid at their last visit may not have active coverage at their next one. Real-time eligibility verification before every encounter is essential for Medicaid patients. The check must confirm not just active coverage but the specific plan the patient is enrolled in to ensure the claim goes to the correct payer.
What are the most common Medicaid billing denial reasons?
The most common Medicaid billing denial reasons are inactive eligibility on date of service, claims submitted to fee-for-service for a patient enrolled in an MCO, provider not enrolled with the specific MCO, missing prior authorization, NPI not matching the state enrollment record, and timely filing violations. All of these are preventable with front-end process controls: real-time eligibility verification confirming the specific plan, pre-service PA confirmation, and provider enrollment completed before the first patient encounter.
What is the timely filing limit for Medicaid billing?
Medicaid timely filing limits vary by state, ranging from 90 to 365 days from the date of service. Individual MCOs within the same state may have different timely filing windows than the fee-for-service program. Practices with Medicaid patients in multiple states must track each state’s filing deadline separately. A universal assumption that 12 months applies as it does with Medicare will produce timely filing denials in states with shorter windows.
Can a provider bill Medicaid and Medicare for the same patient?
Yes, for dual-eligible patients enrolled in both programs. Medicare is always the primary payer. Medicaid is the payer of last resort and can only be billed after Medicare has adjudicated the claim. Billing Medicaid first for a dual-eligible patient produces a correct Medicaid denial because the rules require Medicare primary billing. The error cannot be corrected on the Medicaid claim; it requires Medicare primary submission, which may create timely filing complications if delayed.
What is Medicaid spend-down billing?
Medicaid spend-down allows individuals with income above standard eligibility thresholds to qualify for Medicaid after medical expenses reduce their net income to the eligibility level. Billing for spend-down patients requires tracking their spend-down amount for the billing period, understanding when Medicaid coverage activates after the threshold is met, and submitting claims in the correct sequence. Spend-down rules vary by state and add administrative complexity to Medicaid billing for affected patients.
Related Resources from Qualigenix
Medicaid Billing Done Right Requires State-Level Expertise.
Qualigenix manages Medicaid billing, provider enrollment, and managed care credentialing for practices across 38+ specialties. We handle the state-specific enrollment, eligibility verification, and denial management that keep Medicaid revenue from being left on the table.
Our team delivers 99% claim accuracy, a 95% first-pass acceptance rate, an average 36-day collection cycle, and a 30% reduction in AR days. We onboard in as few as 6 days.
Precision. Progress. Qualigenix.
What’s Next

The Real Cost of Billing Staff Turnover: A Practice-by-Practice Model
TL;DR — Key Takeaway: Billing staff turnover costs far more than a recruiting fee. Replacing one biller runs...

Value-based care contracts: how quality reporting gaps turn into withheld reimbursement
In a value-based care contract, part of your payment is held back until your quality reporting proves the...
CMS Prior Authorization Rules: What Every Practice Must Know to Protect Revenue
Prior authorization denial rates jumped 31% in 2026. That number alone should concern every practice manager, hospital administrator, and...