Understanding the Medical Billing Process: End-to-End Workflow
The Qualigenix Editorial Team consists of certified billing and coding experts with over 40 years of experience across 38+ medical specialties. Our content is rigorously researched against CMS, AMA, and payer-specific guidelines to ensure total compliance and accuracy. We apply the same elite standards to our resources as we do our client work, consistently delivering high claim accuracy and significant reductions in AR days.
A doctor’s visit doesn’t begin or end with the patient walking through the door. Even before the appointment, a detailed sequence begins, which includes turning clinical notes into codes, building claims, and securing payment. This sequence is the healthcare billing process, and it directly shapes how quickly providers get paid and how clearly patients understand their bills. The stakes are high. Nearly 11.8% of claims are denied on first submission, a jump from 10.2% just a few years ago. Each denial delays revenue and adds stress for patients as well as providers already navigating care. So, read on to get the healthcare billing process explained in a step-by-step manner. Along the way, you will also learn KPIs that matter and where automation can reduce errors, speed up cash flow, and improve transparency.
Healthcare Billing Process Explained: End-to-End Overview
The medical billing cycle follows a clear structure. Each stage plays a role in moving a claim from patient intake to insurer approval. Errors at any point ripple downstream, creating denials or delayed revenue. Here’s the healthcare billing process explained for you in detail:
Front-End: Patient Registration & Insurance Eligibility
This is where accuracy starts. Staff collect demographics, insurance IDs, and consent forms. Validate eligibility, benefits and coverage before billing begins to catch expired plans or prior authorization requirements. Even small mistakes here, like a wrong DOB or invalid insurance ID, often trigger denials. A reliable front-end process protects revenue and prevents patients from facing unexpected bills.
Mid-Cycle: Charge Capture & Accurate Coding (ICD-10/CPT)
Once care is provided, every service, supply, or test must be documented and converted into billable items. This is called charge capture. The next step is assigning the right ICD-10 codes for diagnoses and CPT/HCPCS codes for procedures. The coding must reflect documentation exactly and meet payer rules. If a code is vague, deprecated, or doesn’t support medical necessity, payers may reject or down-adjust. Strong coding practices ensure services are billed correctly and support compliance.
Back-End: Claim Scrubbing & Submission (837 via Clearinghouse)
At this stage, all the details come together into a standardized claim file (often the 837 format). Before it ever reaches a payer, most claims go through a clearinghouse. Here, “scrubbing” includes automated and manual checks for missing modifiers, invalid codes, or demographic mistakes. A “clean” claim passes through payer systems more smoothly, which raises your first-pass yield, reduces rework and saves staff time.
Medical Billing Workflow: Payer Adjudication & Payment Posting
After a claim is submitted, the insurance company takes over. Here’s what happens next in the medical billing workflow:
ERA/EOB, Adjustments, Reconciliation
After a claim is sent, the payer runs it through adjudication to decide what gets paid, what doesn’t, and why.
- They check eligibility, coverage rules, and medical necessity, then send back the results as an electronic remittance advice (ERA) or explanation of benefits (EOB).
- Billing staff then post the payments, apply contractual adjustments, and flag any denials.
Reconciling payments also highlights issues, like underpayments or frequent denial codes. This protects revenue and gives providers insight into where the process needs to be tightened.
Patient Billing vs. Payment Posting
These two terms often get mixed up when you understand the end-to-end medical billing process, but they’re different.
- Payment posting is internal. This involves updating the system with what the insurance company paid, adjusted, or denied.
- Patient billing is external. This includes sending a statement to the patient for anything left unpaid.
Posting keeps the accounts accurate, whereas billing gives patients a clear explanation of what they owe. When both are done well, you prevent confusion and build trust with patients at the end of the process.
Denial Management & AR Follow-Up
Even with clean claims, denials still happen. In fact, nearly 12% of claims are denied on the first submission, costing providers time and revenue. That’s why denial management and accounts receivable (AR) follow-up are critical parts of the billing steps.
Top Denial Buckets and Fast Fixes (Checklist)
Most denials fall into a few common categories:
Eligibility Errors
One of the most common issues. A patient’s plan may have expired, or their coverage may not include the service provided. For example, a claim for physical therapy could be denied if the plan doesn’t cover outpatient rehab.
Fix: Always run real-time eligibility checks before every visit, even for returning patients.
Authorization Issues
Many procedures, imaging tests, or surgeries require prior approval from the payer. If the authorization wasn’t requested or expired before the visit, the claim will likely be denied.
Fix: Use a pre-authorization checklist for services that typically require it and confirm the approval number is documented in the chart.
Coding Mistakes
Errors like mismatched medical coding ICD-10 and CPT codes, outdated codes, or missing modifiers can stop a claim cold. For instance, coding for a diagnosis of “diabetes” without linking it to the specific treatment provided can trigger a denial.
Fix: Make sure coders have complete provider notes, run coding edits before submission, and stay updated on code changes.
Duplicate Claims
Submitting the same service more than once often happens when re-billing a denied claim without correcting the original error. Payers flag these as duplicates and won’t pay.
Fix: Track claim status carefully and resubmit only corrected versions with clear references to prior submissions.
Timely Filing
Every payer sets strict deadlines (often 90–180 days from service date). Missing these windows means the claim won’t be paid, no matter how correct it is.
Fix: Monitor filing deadlines with automated reminders and process claims daily to avoid delays.
AR Worklists, Appeals, Write-off Rules
After a claim is denied, it moves into accounts receivable (AR). Instead of letting denials pile up, billing teams organize them into worklists — basically task lists that show which claims need action. Worklists are often sorted by:
- Age (how long they’ve been unpaid — e.g., 30, 60, 90 days).
- Value (a $5,000 inpatient surgery claim takes priority over a $50 lab test).
- Payer (some insurers have tighter deadlines, so those claims move to the top).
This structure helps staff focus on claims that matter most for cash flow.
When a denial is worth challenging, the team builds an appeal kit. For example, if an MRI was denied for “no prior authorization” but the approval letter is in the chart, staff will attach that letter, the original claim, and a corrected cover sheet. If a coding mismatch caused the denial, they resubmit with the corrected ICD-10 and CPT codes. These appeal kits give payers exactly what they need to reconsider.
Still, not every claim can or should be chased forever. That’s where write-off rules come in. Practices set policies like: “Don’t appeal claims under $100” or “Write off balances older than 365 days if two appeals have failed.” This prevents staff from wasting time on claims with little chance of recovery.
Automation That Moves Results

Many billing challenges come down to manual work with endless eligibility calls, claim status checks, and payment posting. Automation takes over these repetitive tasks. Let us discuss how automation results in faster payments, lower denial rates, and steadier cash flow:
High-Impact Use Cases (Eligibility, Prior Auth, Claim Status, Auto-Posting)
Automation is most useful when it removes repetitive, error-prone tasks from staff. Here’s how it plays out in real medical billing workflows:
Eligibility Checks
Instead of calling insurers one by one, software can instantly confirm if coverage is active and what benefits apply. For example, it can flag that a patient’s plan only covers 20 physical therapy visits a year, avoiding denied claims later.
Prior Authorization
Automated tools track which services require approval and can even submit requests electronically. Say a doctor orders an MRI; automation can send the request, track payer responses, and alert staff when approval is granted.
Claim Status Updates
Without automation, staff often spend hours on hold with payers. Automated status tools “ping” payers electronically and update dashboards. This means the team knows immediately if a claim is pending, approved, or denied.
Auto-posting Payments
When insurance payers send ERA files, automation posts payments directly to patient accounts. For example, if a payer reimburses $1,200 on a $1,500 claim with a $300 deductible, the system applies those adjustments automatically instead of staff entering them line by line.
These use cases save hours every week and prevent mistakes that often lead to denials or rework.
Track Results with KPIs (First-pass Yield, AR Days, DNFB, Denial Rate)
Automation shows its value when you measure the right results. Four key metrics keep billing performance on track:
First-Pass Yield
The percentage of claims paid without any manual fixes. For example, if you submit 1,000 claims and 850 are paid right away, your first-pass yield is 85%. High yield means fewer denials and faster cash.
AR Days
The average number of days it takes to collect payment. If your AR days are 45, it means payments take a month and a half to arrive. Top performers aim for 30 days or less.
DNFB (Discharged Not Final Billed)
The number of days between providing care and sending the bill. A hospital with a DNFB of 10 days is much healthier than one holding claims for 30 days, since delayed billing delays cash flow.
Denial Rate
The percentage of claims denied on first submission. If 100 out of 1,000 claims come back denied, your rate is 10%. Tracking this shows whether fixes in registration, coding, or scrubbing are paying off.
How Qualigenix Can Help with the Healthcare Billing Process?

Billing shouldn’t slow providers down. At Qualigenix, we streamline the cycle from intake to AR follow-up so practices see fewer denials, faster reimbursements, and cleaner books. Let’s discuss how we help providers focus on care while we keep revenue moving:
Clear the Bottlenecks
Most delays happen at intake, coding, or claim submission. We prevent that by verifying coverage upfront, applying rigorous coding QA, and scrubbing every claim before submission. If a denial slips through, our team reworks and resubmits immediately, keeping AR queues lean and cash flow steady.
Step-Mapped Services
Our process covers every stage: insurance verification, coding audits, custom scrubber rules, and denial playbooks. AR is tracked with worklists, so no claim ages out unnoticed. With these guardrails in place, practices stop losing revenue to avoidable errors and wasted follow-ups.
Fast, Measurable Delivery
We integrate with any Electronic Health Record (EHR) or billing system. Our 30-60-90 day onboarding model gets you up and running quickly without disrupting operations. From day one, you’ll see live dashboards with claim status, denials, and AR metrics. We back it up with Service Level Agreements (SLAs) that guarantee performance, and measurable results like fewer denials and reduced AR days.
Ready to Close Billing Gaps? Partner With Qualigenix Today!
The healthcare billing process explained here should not feel like a bottleneck. With the right structure, denials drop, AR days shrink, and revenue flows faster. At Qualigenix, we help you make that shift, starting with one gap at a time. Focus on intake accuracy, coding quality, or AR discipline this month, and watch the impact build. Ready to see fewer denials and faster payments? Partner with us today.
FAQs
1. What are the core steps in the medical billing workflow?
The medical billing workflow follows a connected sequence that moves a claim from patient visit to payment. The steps include patient registration, insurance eligibility verification, charge capture, medical coding, claim submission, payer adjudication, payment posting, and denial management with AR follow up.
2. How do claim scrubbers cut first round denials?
Claim scrubbers are software tools that review claims before submission. They detect common issues such as missing modifiers, invalid diagnosis or procedure codes, and patient demographic mismatches. Identifying these errors early increases first pass yield and reduces rework by allowing more claims to get paid on the initial submission.
3. Which monthly KPIs matter most for medical practices?
Four KPIs provide a clear view of billing performance. First pass yield shows how many clean claims are paid without rework. AR days measure average collection time. Denial rate tracks the percentage of claims rejected by payers. DNFB reflects how quickly charges move from care delivery to billing. Monthly review highlights delays and process gaps.
4. Where does automation create the fastest return in medical billing?
Automation delivers quick returns in repetitive billing tasks. Eligibility checks, prior authorizations, claim status updates, and payment posting benefit the most. Automated ERA posting removes manual data entry, shortens reimbursement cycles, and allows billing staff to focus on denials and exceptions.
5. What improves first pass yield within 30 days?
Fast improvements come from strengthening front end processes. Real time eligibility checks, clear pre authorization workflows, and mandatory claim scrubbing before submission reduce avoidable errors. These actions often improve first pass yield within the first month and stabilize cash flow quickly.
What’s Next

Medical Coding Errors That Cost Practices the Most (And How to Catch Them Before They Submit)
Medical Coding Errors That Cost Practices the Most (And How to Catch Them Before They Submit) Written by the...
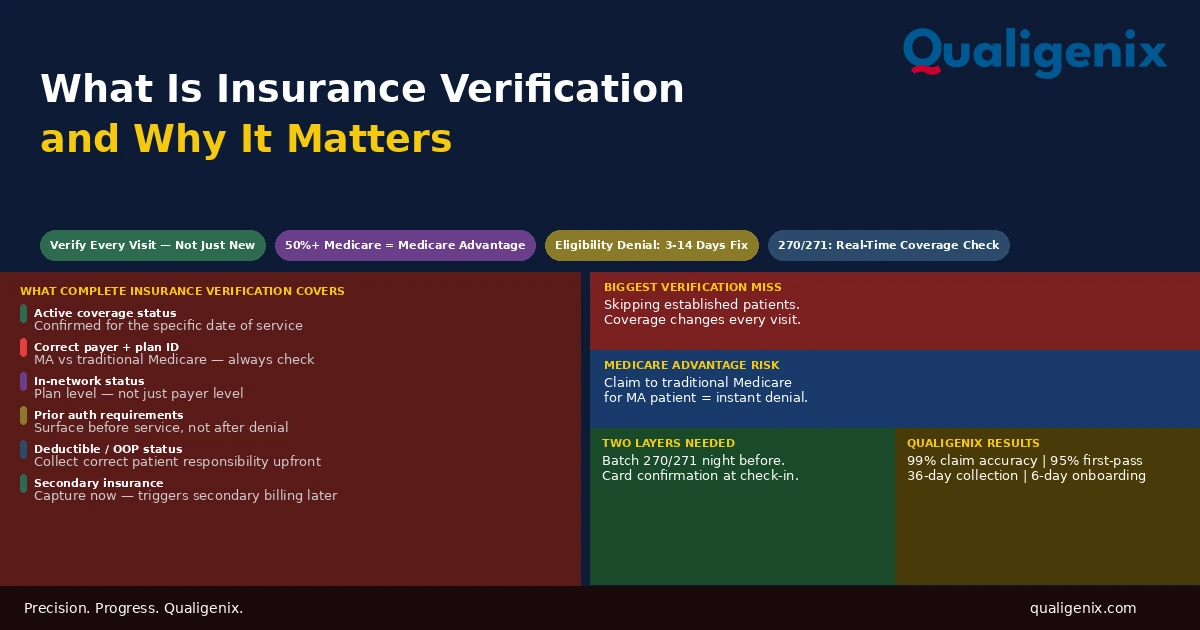
What Is Insurance Verification and Why It Matters
Insurance verification is the front-end process that determines whether a claim will be paid before the patient ever enters...

Insurance Denial Appeals: What Practices Miss
Most insurance denial appeals that fail don’t fail because the clinical case was weak. They fail because the...