What Is RCM in Healthcare? A Breakdown for Practice Managers
The Qualigenix Editorial Team consists of certified billing and coding experts with over 40 years of experience across 38+ medical specialties. Our content is rigorously researched against CMS, AMA, and payer-specific guidelines to ensure total compliance and accuracy. We apply the same elite standards to our resources as we do our client work, consistently delivering high claim accuracy and significant reductions in AR days.

RCM in healthcare, short for revenue cycle management, is the complete process your practice uses to get paid. It starts when a patient books an appointment and ends when you collect the final dollar owed. There are eight distinct stages. Get any one of them wrong and you lose revenue, often without realizing where the leak is.
Most practice managers know their clinical workflow cold. They can walk you through every step a patient takes from check-in to discharge. But when it comes to what happens after the patient leaves, it gets murky fast.
That’s where RCM lives. And that’s where a lot of practices bleed money without realizing it.
This breakdown covers every stage of the revenue cycle in plain language, no billing jargon required. You’ll also find benchmarks to compare your practice against, a detailed look at what poor RCM actually costs, and a clear explanation of where most practices go wrong before they even submit a claim.
RCM in healthcare is the end-to-end process of tracking, managing, and collecting revenue for every patient encounter. It covers patient registration, insurance verification, medical coding, claims submission, payment posting, denial management, and patient collections. All eight steps must work together. A failure at any single stage means lost or delayed revenue.
Key RCM Statistics for 2026
| Metric | Industry Average | Qualigenix |
|---|---|---|
| Claim denial rate | 10-15% | <5% |
| First-pass acceptance rate | ~85% | 95% |
| Average collection cycle | 45-60 days | 36 days |
| Denied claims never reworked | 35% (MGMA) | Near 0% |
| Claim accuracy rate | Varies widely | 99% |
| Revenue lost to billing errors (US, annually) | $125 billion+ | N/A |
| Cost to rework one denied claim | $25-$118 | N/A |
| Practices reporting better collections after outsourcing | 73% | N/A |
| Top denial cause (coding errors) | 62% of practices | N/A |
| Reduction in AR days with outsourced RCM | Up to 30% | 30%+ |
| Specialties served by Qualigenix | N/A | 38+ |
| Average Qualigenix onboarding time | N/A | 6 days |
| Clean claim rate target (HFMA benchmark) | 98%+ | 99% |
| Target AR days (HFMA benchmark) | Under 40 days | 36 days avg |
Sources: MGMA 2025 Revenue Cycle Report; HFMA Revenue Cycle Benchmarks; CMS; Qualigenix internal performance data.
RCM vs. Medical Billing: Clearing Up the Confusion
These two terms get used interchangeably in almost every conversation about healthcare finance. They’re not the same thing. Understanding the difference matters before you can evaluate where your practice’s revenue process is actually breaking down.
Medical billing is one step inside the revenue cycle, specifically the claims submission and payer follow-up piece. If you hire a billing-only company, they’re handling claim creation, submission, and possibly denial follow-up. Everything before and after that is still on your team.
RCM is the full picture. It starts the moment a patient contacts your practice and ends when every dollar for that encounter has been collected, whether from the payer or the patient. A true RCM partner takes ownership of all eight stages. A billing-only vendor handles maybe two or three of them.
This distinction matters when you’re evaluating vendors. A company that advertises “medical billing services” isn’t necessarily offering the same scope as one that offers “full-cycle RCM.” Ask specifically which stages they own before signing anything.
The Eight Stages of RCM in Healthcare
Each stage feeds directly into the next. A problem at Stage 2 creates a denial at Stage 5. A missed charge at Stage 3 means no claim at Stage 5 at all. Here’s what each stage actually involves and where the failure points are.
Stage 1: Pre-Registration
Before a patient walks through the door, your team collects their name, date of birth, insurance ID, group number, and referring provider information. It sounds administrative. It is. But the accuracy of this data determines whether your claim will process cleanly weeks later.
A transposed digit in an insurance ID. A missing referral authorization. A name that doesn’t match what’s on file with the payer. Any of these creates a denial, and by the time it surfaces, your team has already provided the care. You’re now chasing reimbursement for something you could have caught in 90 seconds at registration.
The fix is a standardized pre-registration checklist, verified by your front desk for every patient, every visit. Not just new patients.
Stage 2: Insurance Eligibility Verification
Eligibility verification confirms that the patient’s coverage is active, that your practice is in-network, and that the planned services fall within the patient’s benefit plan. It also surfaces the patient’s deductible status, copay, and whether a prior authorization is required for the visit.
Many practices run eligibility checks only for new patients, or only once at the start of a care relationship. That’s a gap. Insurance coverage changes constantly. Patients change jobs, age into Medicare, or lose Medicaid eligibility without telling you. MGMA research consistently shows eligibility failures in the top five denial causes across all specialties.
Run eligibility checks before every encounter, not once per patient relationship. Most practice management systems can automate this the night before an appointment is scheduled.
Does prior authorization affect eligibility? Yes. Some services require advance approval from the payer before they’re covered. If a prior authorization is required and you don’t have one, the claim will be denied even if the patient’s coverage is active and in-network. Always check authorization requirements at this stage, not after the service is delivered.
Stage 3: Charge Capture
Charge capture is the process of recording every billable service delivered during an encounter, including procedures, labs, injections, supplies, and time-based evaluation and management (E&M) services. If a service isn’t captured, it won’t be coded. If it isn’t coded, it won’t be billed. You’ve provided care for free.
Charge capture failures are uniquely damaging because they’re invisible. A denial at least generates a code you can respond to. A missed charge generates nothing. There’s no alert, no denial code, no workflow trigger. The revenue simply doesn’t exist in your AR until someone audits the encounter documentation and finds the gap.
Practices with high patient volume are especially vulnerable. The faster the pace of care, the higher the risk that some charges slip through undocumented. Regular charge capture audits, at minimum weekly, are the only way to catch these before they become permanent losses.
Stage 4: Medical Coding
Medical coding converts clinical documentation into the standardized codes payers use to process claims. ICD-10 codes describe the patient’s diagnosis. CPT codes describe the procedure or service performed. Payers cross-reference these to determine coverage and reimbursement rates.
Coding is where 62% of claim denials originate, according to MGMA survey data. An incorrect CPT code, a missing modifier, a diagnosis code that doesn’t support medical necessity, or an invalid ICD-10 and CPT combination will trigger a denial or an underpayment. Both cost you money.
Coding accuracy also has compliance implications. Upcoding, billing for a higher-level service than what was actually provided, is a violation of the False Claims Act and can trigger audits, recoupments, and penalties. Downcoding, billing for less than you delivered, is legal but costs you revenue. Accurate coding to the highest level supported by documentation is the only defensible practice.
Warning: Payer coding requirements change regularly. CMS updates ICD-10 codes annually each October. CPT code changes take effect each January. A code that was valid last year may be discontinued, bundled, or require a new modifier this year. Coding teams must stay current or claim denial rates will climb without an obvious cause.
Stage 5: Claims Submission
A clean claim is one submitted with no errors, no missing fields, and supporting documentation for every code billed. Payers process clean claims faster and at a higher acceptance rate. The industry standard for clean claim rate, per the Healthcare Financial Management Association (HFMA), is 98% or better.
Most payers require electronic submission using the ANSI X12 837P format (professional claims) or 837I (institutional). Claims should go out within 24 to 48 hours of the encounter. Most payers have a timely filing window of 90 to 365 days, but the sooner a claim is submitted, the sooner it gets paid. And if a claim gets rejected, you need time to correct and resubmit before the window closes.
Your first-pass acceptance rate is the single most important indicator of submission quality. If your rate is below 90%, something is wrong upstream: pre-registration errors, eligibility gaps, or coding mistakes. The submissions stage itself doesn’t create problems. It reveals them.
What’s the difference between a rejection and a denial? A rejection means the claim didn’t make it into the payer’s system at all because of a data error (wrong payer ID, formatting issue, missing required field). A denial means the payer received the claim, reviewed it, and decided not to pay for a specific reason. Rejections are fixed at submission. Denials require a correction and appeal process.
Stage 6: Payment Posting and Reconciliation
When a payer processes a claim, they send back an Explanation of Benefits (EOB) that details what was billed, what was allowed, what was adjusted, and what remains as the patient’s responsibility. Payment posting is the process of recording these payments in your practice management system and reconciling them against what you expected to receive.
Reconciliation is the step most teams skip or do superficially. If your team posts payments without comparing them to your contracted fee schedule, you could be accepting less than your contracted rate on every claim. Payers underpay. It happens regularly. But you won’t know unless someone is checking.
Underpayment recovery requires identifying the discrepancy, documenting the contracted rate, and filing a recoupment request with the payer. It’s time-consuming but the amounts add up. For a high-volume practice, even a 2-3% underpayment rate across all claims represents significant lost revenue over a year.
Stage 7: Denial Management
Denials happen in every practice. The question isn’t how to eliminate them entirely. It’s how fast you respond and how many you recover.
According to MGMA, 35% of denied claims are never reworked. That means one in three denials defaults to permanent revenue loss with no appeal attempted. The math on that is brutal. At $150 average claim value and a 12% denial rate, a practice submitting 500 claims per month is leaving over $3,000 per month on the table from denials alone, before accounting for any rework costs.
A functioning denial management process does three things. First, it logs every denial by reason code immediately. Second, it routes each denial to the right team member based on what type of correction it needs. Third, it tracks appeal deadlines and escalates anything at risk of aging out. Many payer appeal windows are 60 to 90 days. Miss the window and the denial becomes permanent, regardless of whether the original denial was justified.
Denial root-cause analysis is equally important. If the same denial code keeps appearing, that’s a process failure, not a one-off error. Fixing the upstream cause eliminates the denial category rather than treating each one individually.
Stage 8: Patient Collections
Patient financial responsibility has grown significantly over the past decade. High-deductible health plans now cover a large share of insured Americans, which means more patients owe substantial balances after insurance processes. For many specialties, patient collections now represent 20-30% of total practice revenue.
Collecting that money requires clear, accurate statements sent quickly after the EOB is posted, multiple payment options including online portals, and a structured follow-up workflow for balances that aren’t paid within 30 days. Practices that send one paper statement and wait have collection rates well below those that use automated reminders, digital statements, and payment plans.
Patient experience matters here too. Billing errors, confusing statements, or surprise balances damage trust. A patient who gets an incorrect bill or can’t reach anyone to explain it doesn’t just dispute the charge. They often don’t come back. The revenue cycle and patient retention are more connected than most practice managers realize.
The Real Cost of a Broken Revenue Cycle
Revenue cycle failures don’t announce themselves. They accumulate in quiet patterns: a few eligibility checks skipped, a handful of denials left unworked, a coding error repeated across 200 claims before anyone notices. By the time a cash flow problem is visible, the leaks have usually been running for months.
US healthcare loses over $125 billion annually to billing errors and inefficiencies. That number is made up of individual claim failures at individual practices. A 10% denial rate on 6,000 annual claims at $150 average value is $90,000 in denied revenue per year, before you account for rework costs. If 35% of those denials go unworked, that’s $31,500 in permanent annual losses from denials alone.
Add underpayment gaps, missed charges, and patient balances that age out uncollected, and the total picture of what poor RCM costs becomes clear. It’s not a billing problem. It’s a financial management problem.
In-House RCM vs. Outsourced RCM: A Direct Comparison
| Factor | In-House RCM | Outsourced RCM |
|---|---|---|
| Staffing costs | Salary + benefits + turnover costs | Fixed percentage of collections |
| Training and updates | Practice’s responsibility | Vendor’s responsibility |
| Payer policy knowledge | Limited to team’s experience | Broad, across multiple payers |
| Denial management depth | Often deprioritized due to volume | Dedicated specialists per denial type |
| Scalability | Requires hiring as volume grows | Scales without new hires |
| Technology investment | Practice buys and maintains software | Included in service |
| Reporting and visibility | Varies by system and staff capacity | Regular performance reports |
| First-pass acceptance rate | Industry avg ~85% | Qualigenix: 95% |
MGMA data shows 73% of practices that outsource RCM report improved collection rates within the first year. The gains come from specialization, not just lower cost. An outsourced team that works denials all day is faster and more thorough than an in-house biller splitting time between billing, phones, and front desk coverage.
Five RCM Metrics Every Practice Manager Should Track
You can’t fix what you don’t measure. These five numbers give you an accurate picture of your revenue cycle’s health without needing a deep billing background to interpret them.
First-Pass Acceptance Rate: Target 90% or better. Below 90% means your claims are going out with errors. Find out which denial codes are coming back most often and trace them to the stage where the error originates.
Denial Rate: Target under 5% of submitted claims. At 10-15%, you’re in the industry average range but losing significant recoverable revenue. Anything above 15% is a process failure that needs immediate attention.
AR Days: Target under 40 days. This measures how long money sits uncollected after a claim is submitted. The HFMA benchmark is 40 days. Qualigenix clients average 36. If your practice is running at 60+ days, cash flow is being constrained by process delays, not payer timelines.
Clean Claim Rate: Target 98% or better. This is the percentage of claims submitted with no errors. It’s a leading indicator: if your clean claim rate drops, denial rate will follow within 30-45 days.
Net Collection Rate: Target 95% or better. This measures the percentage of collectible revenue actually collected after contractual adjustments. A rate below 95% means you’re leaving money owed to you uncollected.
How Credentialing Connects to RCM
Many practice managers think of credentialing as an HR process, something that happens when a new provider joins and then doesn’t come up again. That’s a gap in how most practices manage the revenue cycle.
If a provider isn’t credentialed and enrolled with a payer, claims submitted under that provider’s NPI will be denied by that payer. Full stop. It doesn’t matter how accurate the coding is or how clean the claim is. If the provider isn’t recognized by the payer, nothing gets paid.
This matters at hire, when a new provider joins your practice and needs to be enrolled with every payer before billing starts. It also matters during re-credentialing, when lapsed credentials trigger the same denial outcome. And it matters with payer contract changes, when credentialing terms are updated and your team may not be notified automatically.
At Qualigenix, our provider credentialing services run in parallel with RCM setup so your providers are enrolled and active before the first claim goes out. Credentialing gaps are one of the most avoidable denial categories, and one of the most expensive when they happen at scale.
How Qualigenix Handles RCM for Your Practice
At Qualigenix, we manage the full revenue cycle for practices across 38+ specialties. Our team handles every stage, from pre-registration and eligibility verification through claims submission, payment posting, and denial management.
We submit claims within 24 hours of the encounter. We verify eligibility before every visit. Every EOB is reconciled against contracted rates so underpayments don’t go unnoticed. Our denial management team works every denial by reason code, not just the high-dollar ones, because the smaller ones add up just as fast.
Most clients see a 30% reduction in AR days within the first few months of onboarding. Our 95% first-pass acceptance rate means fewer resubmissions, less rework, and faster cash flow. And because we onboard in as few as six days, you’re not waiting months to see results.
RCM Checklist for Practice Managers
- Verify insurance eligibility before every patient encounter, including established patients
- Confirm prior authorizations before scheduling procedures that require them
- Run charge capture audit reports weekly to catch unbilled services
- Submit claims within 24-48 hours of the encounter
- Track first-pass acceptance rate monthly (target: 90%+)
- Categorize denials by reason code to identify pattern failures, not just individual errors
- Work every denial before the payer’s appeal deadline, not just high-dollar claims
- Reconcile payer EOBs against your contracted fee schedule to catch underpayments
- Send patient statements within 7 days of posting the insurance payment
- Offer online and mobile payment options to increase patient collection rates
Frequently Asked Questions About RCM in Healthcare
What is RCM in healthcare?
RCM, or revenue cycle management, is the process healthcare practices use to track patient care from registration through final payment. It covers scheduling, insurance verification, coding, claims submission, denial management, and patient collections.
What are the steps in the revenue cycle?
The revenue cycle has eight main steps: pre-registration, insurance eligibility verification, charge capture, medical coding, claims submission, payment posting, denial management, and patient collections. Each stage feeds directly into the next.
Why do practices lose revenue in the billing process?
Most revenue loss comes from coding errors, missed eligibility checks, late submissions, and denials that never get appealed. MGMA data shows 35% of denied claims are never reworked, which becomes permanent revenue loss.
What are the most common causes of claim denials?
The top five denial causes are: coding errors (ICD-10 or CPT mistakes), eligibility failures, missing prior authorizations, duplicate claim submissions, and timely filing violations. Each requires a different correction path.
What is a first-pass acceptance rate?
It measures how many claims a payer accepts on the first submission without corrections. The industry average is around 85%. Qualigenix clients run at 95%, which means fewer resubmissions and faster payment.
What is accounts receivable (AR) in healthcare RCM?
Accounts receivable is the total amount owed to your practice for services not yet paid. AR days tracks how long it takes to collect. The HFMA benchmark is under 40 days. If you’re running at 60+ days, process delays are constraining your cash flow.
How long does the revenue cycle take from service to payment?
The industry average runs 45 to 60 days. Qualigenix clients average 36 days. Faster submission, higher clean claim rates, and proactive denial follow-up all shorten the cycle.
Should a practice handle RCM in-house or outsource it?
Outsourcing typically lowers costs and improves collection rates. 73% of practices that outsource report better collections within the first year. The gains come from specialization, scale, and consistent payer knowledge that most in-house teams can’t match.
How does credentialing affect the revenue cycle?
If a provider isn’t credentialed with a payer, every claim submitted under that provider will be denied by that payer. Credentialing gaps are one of the most avoidable and most expensive RCM failures. Completing enrollment before billing starts eliminates this denial category entirely.
What RCM metrics should a practice manager track?
The five key metrics are: first-pass acceptance rate (target 90%+), denial rate (target under 5%), AR days (target under 40), clean claim rate (target 98%+), and net collection rate (target 95%+). These five numbers give a complete picture of revenue cycle health.
What is the difference between a rejection and a denial?
A rejection means the claim didn’t enter the payer’s system due to a data error. A denial means the payer received and reviewed the claim but decided not to pay. Rejections are fixed at submission. Denials require a correction and formal appeal within the payer’s deadline.
How does RCM affect patient experience?
A well-run revenue cycle means fewer billing errors, accurate cost estimates before visits, and clear statements after insurance pays. Fewer billing disputes and easier payment options improve patient satisfaction scores and reduce no-return rates after billing problems.
Related Resources
- Medical Billing Services
- Denial Management and Claims Appeals
- Payment Posting and Reconciliation Services
- Provider Credentialing Services
- Blog: What Is Payment Posting in Medical Billing?
- Blog: Healthcare Credentialing in 2026
- CMS: Provider Enrollment and Certification
- HFMA: Revenue Cycle Benchmarks
Ready to Fix Your Revenue Cycle?
Most practices don’t know how much revenue they’re leaving on the table until they see the numbers. We’ll show you exactly where your cycle is leaking and how quickly we can fix it.
Qualigenix delivers 99% claim accuracy, a 95% first-pass acceptance rate, an average 36-day collection cycle, and a 30% reduction in AR days. We onboard in as few as 6 days.
Precision. Progress. Qualigenix.
What’s Next
Medical Coding Errors That Cost Practices the Most (And How to Catch Them Before They Submit)
Medical Coding Errors That Cost Practices the Most (And How to Catch Them Before They Submit) Written by the...
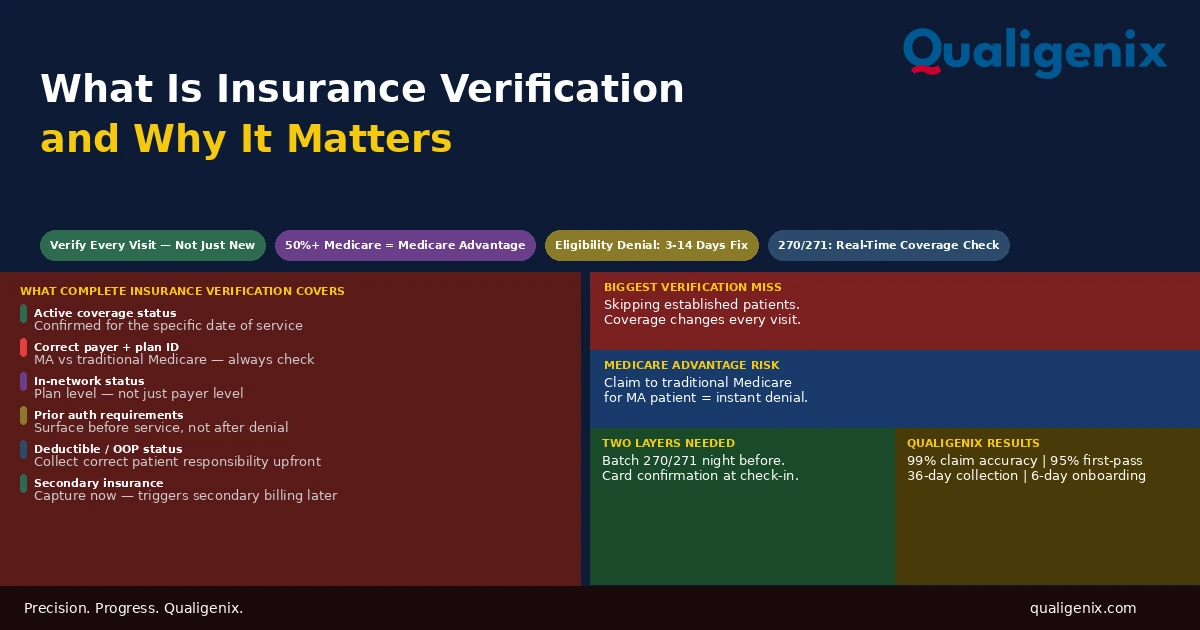
What Is Insurance Verification and Why It Matters
Insurance verification is the front-end process that determines whether a claim will be paid before the patient ever enters...

Insurance Denial Appeals: What Practices Miss
Most insurance denial appeals that fail don’t fail because the clinical case was weak. They fail because the...