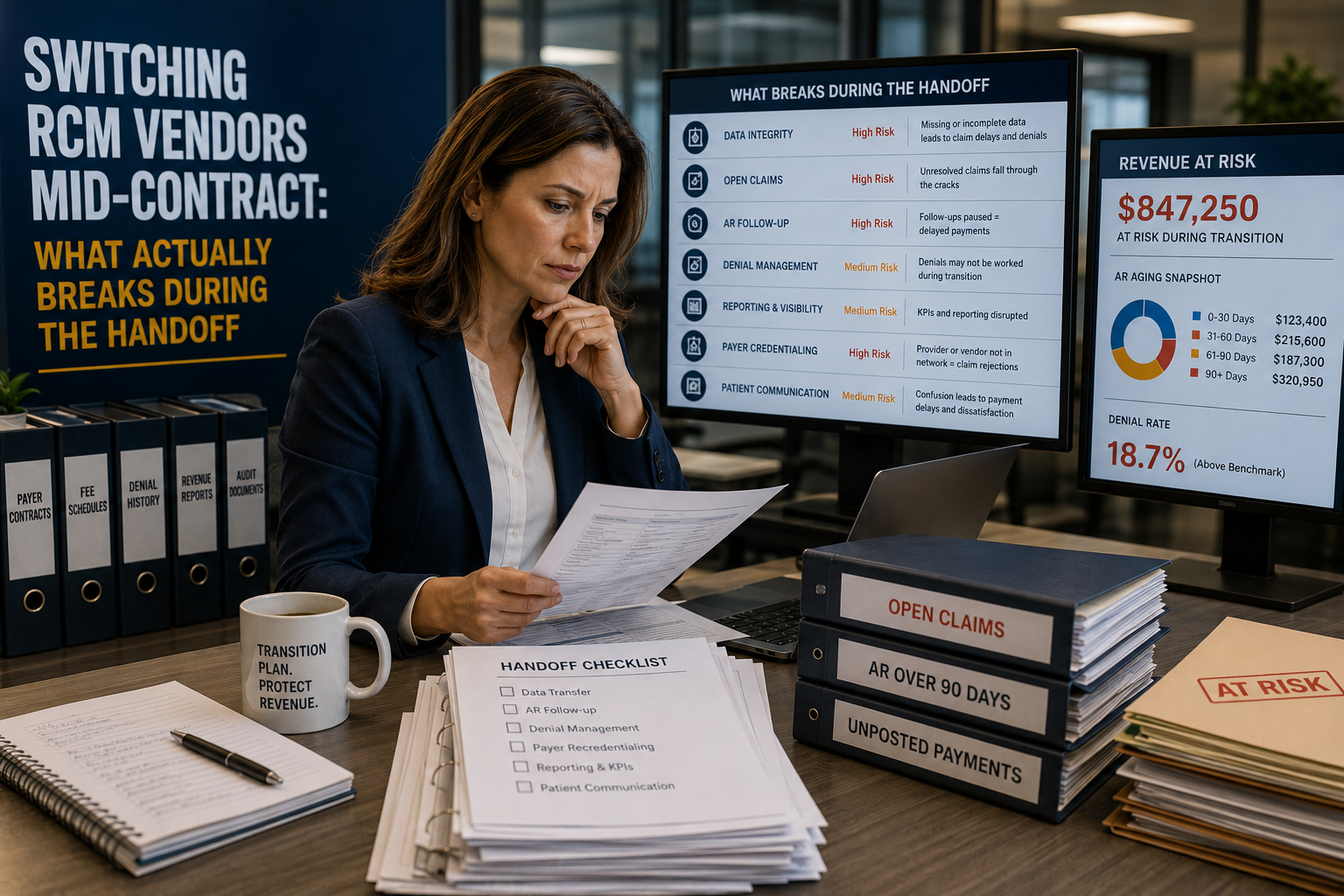
Switching RCM Vendors Mid-Contract: What Actually Breaks During the Handoff
The Qualigenix Editorial Team consists of certified billing and coding experts with over 40 years of experience across 38+ medical specialties. Our content is rigorously researched against CMS, AMA, and payer-specific guidelines to ensure total compliance and accuracy. We apply the same elite standards to our resources as we do our client work, consistently delivering high claim accuracy and significant reductions in AR days.
Switching RCM vendors before a contract ends feels like the fast fix for a billing team that’s underperforming. It isn’t free. Claims stall in the queue, payer enrollment records lag behind, and clearinghouse connections break more than practices expect. A clean handoff needs a 60 to 90 day overlap window, a documented AR cutoff date, and a vendor willing to hand over raw claim data, not just a summary report.
Practice managers rarely leave an RCM vendor because things are going well. Denial rates climb, calls go unanswered, or a contract renewal reveals fees nobody agreed to. The decision to switch is usually the easy part. What happens in the 60 to 90 days after signing with a new vendor is where most of the damage gets done. Claims stall, payer records lag, and staff spend weeks re-entering data that should have transferred cleanly.
This isn’t a reason to stay with a vendor that’s failing you. It’s a reason to plan the handoff instead of just signing a new contract and hoping the rest sorts itself out.
During an RCM vendor switch, the biggest breaks happen in three places: claims already sitting in the payer queue when the transition starts, payer enrollment and EFT/ERA records tied to the old vendor’s clearinghouse ID, and historical AR data that doesn’t map cleanly into the new system’s fields.
Key Numbers to Know Before You Switch
| Metric | Typical Range | Why It Matters |
|---|---|---|
| Recommended transition overlap window | 60–90 days | Time needed to re-enroll payers and test claims before full cutover |
| Medicare timely filing deadline | 12 months from date of service | Old claims can still be filed late if they’re lost in the handoff |
| Commercial payer timely filing | 90–180 days, payer-dependent | Shorter windows than Medicare, higher risk if AR sits unworked |
| EDI clearinghouse re-enrollment | 2–4 weeks | Needed before the new vendor can submit claims electronically |
| EFT/ERA re-enrollment per payer | 3–6 weeks | Payments can be delayed or misrouted if this isn’t done early |
| Delegated credentialing re-verification | 30–60 days | Applies when the outgoing vendor handled delegated credentialing |
| Post-cutover reconciliation review | 30 days after go-live | Catches claims that fell between the two vendors |
| Qualigenix average onboarding time | 6 days | From signed agreement to active claims processing |
| Qualigenix claim accuracy rate | 99% | Reduces rework during the highest-risk transition window |
| Qualigenix first-pass acceptance rate | 95% | Fewer claims bounce back during the sensitive early months |
| Qualigenix average AR days reduction | 30% | Measured against pre-transition AR aging |
| Qualigenix average collection cycle | 36 days | From claim submission to payment posting |
| Specialties supported | 38+ | Relevant for practices with mixed-specialty billing needs |
Why Practices Switch RCM Vendors Mid-Contract
Most mid-contract switches trace back to one of three problems: denials that never get worked, reporting that doesn’t match what the practice actually collects, or a fee structure that changed after signing. None of these show up on day one. They show up six or nine months in, once the honeymoon period ends and the practice starts pulling its own AR aging reports.
By the time a practice decides to switch, there’s usually a backlog of unworked denials and a stack of claims sitting past 90 days. That backlog doesn’t disappear because a new vendor takes over. It becomes the first thing the new team has to untangle, and untangling someone else’s mess always takes longer than starting clean.
This is why the “what breaks” question matters more than the “who’s better” question. The new vendor might be a clear upgrade. The transition itself is still the riskiest 90 days in the relationship.
Claims Left in Limbo: What Happens to Work-in-Progress AR
Every practice has claims sitting somewhere in the payer pipeline on the day it signs with a new vendor. Some are pending, some are denied and waiting for appeal, some are still within the timely filing window but haven’t been touched in weeks. These claims are the single biggest risk in any transition.
The problem isn’t that this AR gets lost on paper. It’s that nobody owns it in practice. The outgoing vendor assumes the new team will pick it up. The new vendor assumes the outgoing team is still working it under contract. Both assumptions are wrong, and the claims sit untouched until someone notices a drop in collections weeks later.
The fix is a written cutoff date, not a verbal understanding. Every claim dated before the cutoff stays with the outgoing vendor’s AR team until it’s resolved. Everything after belongs to the new vendor. Put this in writing before termination notice goes out, not after.
Data Migration Gaps: Where Patient and Payer Data Get Lost
Most billing vendors will hand over a data export when asked. Fewer will hand over one that’s actually usable. A PDF summary of AR aging is not a data export. A practice needs raw claim history, patient demographics, payer plan details, and ERA/EOB files in a format the new system can import directly.
Field mapping is where most of the pain happens. Payer IDs, provider taxonomy codes, and modifier logic don’t always translate one-to-one between systems. A claim that mapped correctly in the old system can bounce with an edit error in the new one, even though nothing about the underlying claim changed.
Ask for the export early, and test it before the cutoff date arrives. Running a sample batch of claims through the new system while the old vendor is still active gives you time to catch mapping errors before they turn into denied claims.
Credentialing and Payer Enrollment Interruptions
Switching billing vendors doesn’t usually require re-credentialing providers with payers. What it does require is updating EFT and ERA enrollment, since payments and remittance files are routed to the old vendor’s clearinghouse ID. Skip this step and payments keep landing somewhere nobody is checking.
If the outgoing vendor handled delegated credentialing on the practice’s behalf, that relationship needs to be re-verified with each affected payer. This can take 30 to 60 days depending on the payer, and it’s easy to miss if nobody flags it before the switch.
Start EFT and ERA re-enrollment 45 to 60 days before the planned cutover. Payer processing times vary, and some payers are slower than others to update routing on file.
Clearinghouse, EFT, and EHR Integration Breakpoints
The technical side of a handoff breaks in predictable places. The new vendor needs its own clearinghouse connection tested and live before it can submit claims electronically. If the EHR system pushes charges directly to the billing platform, that interface needs to be reconfigured and tested, not assumed to work the same way it did with the old vendor.
Practices that skip parallel testing often find out about integration problems the hard way, when a batch of claims fails to submit during the first live week. By then, staff are already juggling a new system and a stack of claims that need manual resubmission.
Run a test batch through the new vendor’s system before cutover while the old system is still active as a fallback. This catches integration issues while there’s still time to fix them without a claims backlog piling up.
Staff and Communication Breakdown During the Transition
The people problems during a vendor switch are as real as the technical ones. Front-desk staff need to know which insurance verification workflow to use starting on a specific date. Billing staff need training on the new platform before go-live, not during the first week of live claims, when there’s no room to slow down and learn.
Patients feel this too. A billing question that used to get answered same-day can sit for a week if nobody’s clear on who owns patient calls during the overlap period. That’s a trust problem on top of an operational one.
Assign a single point of contact on the practice side who tracks the transition end to end. Without one person owning the timeline, tasks fall through the gap between “the old vendor’s job” and “the new vendor’s job.”
Should you notify patients about an RCM vendor switch? Only if it affects how they pay or who they call with billing questions. A brief notice on statements or at check-in during the transition window prevents confused calls to the front desk.
How to Structure a Clean Handoff
A structured transition follows the same sequence regardless of practice size or specialty:
- Set the AR cutoff date at the start of a billing cycle, not the middle.
- Request a full data export in a usable format, not a summary PDF.
- Start clearinghouse and EFT/ERA re-enrollment 45 to 60 days out.
- Run a parallel test batch of claims before the cutoff date.
- Document in writing which vendor owns denials and appeals on pre-cutoff claims.
- Train front-desk and billing staff before go-live.
- Reconcile AR 30 days after cutover to catch anything that slipped through.
Every step here exists because someone skipped it and paid for it in lost AR. None of them are optional if the goal is a switch that doesn’t show up as a dip on next quarter’s collections report.
Unmanaged Switch vs. Structured Transition
| Task | Unmanaged Switch | Structured Transition |
|---|---|---|
| AR ownership | Assumed, undocumented | Written cutoff date, assigned owner |
| Data export | Summary report only | Full raw export, tested before cutoff |
| Clearinghouse setup | Started after go-live | Started 45–60 days before cutover |
| Staff training | During first live week | Completed before go-live |
| Reconciliation | Only when a problem surfaces | Scheduled 30-day review, built in |
Is a 60 to 90 day overlap always necessary? For most practices, yes. Smaller practices with lower claim volume can sometimes compress this to 45 days, but skipping the overlap entirely almost always shows up as a temporary drop in collections.
How Qualigenix Handles the Handoff
At Qualigenix, we’ve built our onboarding process around the exact failure points above, because we’ve taken over mid-contract for practices more times than we can count. Every transition starts with a written AR cutoff date and a full data audit, not a verbal handshake. Our medical billing services team runs clearinghouse and EFT/ERA re-enrollment in parallel with your current vendor’s remaining contract term, so nothing sits in a gap.
Our credentialing team handles delegated credentialing re-verification where it applies, and our denial management team takes ownership of pre-cutoff AR the moment the transition plan is signed. Average onboarding runs 6 days from signed agreement to active claims processing, with a 30-day reconciliation review built into every transition plan.
What practice managers say about working with Qualigenix
“We switched mid-contract because our old vendor stopped working denials. Qualigenix ran the transition and our days in AR went from 61 to 33 in the first quarter.”
Melissa Grant
Practice Administrator, Family Medicine, Ohio
“We had a hard cutoff date on our EFT re-enrollment and Qualigenix had every payer connection tested two weeks before go-live. Zero claims got lost in the handoff.”
Daniel Ruiz
Practice Manager, Orthopedics, Texas
“Our old vendor’s data export was a mess. Qualigenix rebuilt our claim history and onboarded us in 6 days without a gap in AR follow-up.”
Priya Nair
Billing Director, Multi-Specialty Group, California
“First pass acceptance jumped to 95% within the first two months after Qualigenix took over our billing mid-contract. The transition plan covered things our old vendor never mentioned.”
Thomas Reilly
Practice Owner, Internal Medicine, Georgia
10-Point Handoff Checklist
- ☐ AR cutoff date set at the start of a billing cycle
- ☐ Full raw data export requested and confirmed in writing
- ☐ Data export tested against the new system before cutoff
- ☐ Clearinghouse re-enrollment started 45–60 days before cutover
- ☐ EFT/ERA re-enrollment submitted to every affected payer
- ☐ Delegated credentialing re-verified where applicable
- ☐ EHR interface tested with a parallel claims batch
- ☐ Pre-cutoff AR ownership documented in writing
- ☐ Staff training completed before go-live
- ☐ 30-day post-cutover reconciliation scheduled
Frequently Asked Questions
How long does an RCM vendor transition usually take?
A structured transition runs 60 to 90 days from notice of termination to full cutover. Skipping the overlap window to switch in a single weekend almost always costs a practice lost claims or payer data.
What happens to claims already in process when you switch vendors?
They stay with the original vendor’s clearinghouse ID until they resolve. The outgoing vendor should keep working denials on this AR through the agreed cutoff date, while the new vendor takes everything dated after.
Do you need to re-credential with payers when you switch RCM vendors?
Full re-credentialing usually isn’t required, but EFT and ERA enrollment tied to the old clearinghouse ID does need updating with each payer, which can take three to six weeks.
Who owns patient and claims data during a vendor switch?
The practice owns its patient and claims data at all times. Confirm the export format and delivery deadline with the outgoing vendor in writing before giving termination notice.
What is the biggest risk of switching RCM vendors mid-contract?
A coverage gap in AR follow-up, where claims sit stuck between two vendors that neither one is actively working. This is what drives the visible spike in days in AR that shows up two to three months after a switch.
Can you switch RCM vendors before your contract term ends?
Most RCM contracts allow early termination with 30 to 90 days written notice, though some carry a fee. Review the termination clause and data ownership language before signing with a new vendor.
What should be in an RCM vendor transition checklist?
Data export format, an AR cutoff date, clearinghouse and EFT/ERA re-enrollment, EHR interface testing, staff training, denial and appeal handoff, and a 30-day post-cutover reconciliation review.
Related Resources
- Medical Billing Services
- Provider Credentialing Services
- Denial Management and Appeals
- Book a Free Consultation
Planning a Mid-Contract Switch?
Get a transition plan built around your cutoff date, not a generic checklist. We’ll map your AR, payer connections, and data export before you give notice.
Our team delivers 99% claim accuracy, a 95% first-pass acceptance rate, an average 36-day collection cycle, and a 30% reduction in AR days. We onboard in as few as 6 days.
Precision. Progress. Qualigenix.
What’s Next

Medical Coding Errors That Cost Practices the Most (And How to Catch Them Before They Submit)
Medical Coding Errors That Cost Practices the Most (And How to Catch Them Before They Submit) Written by the...
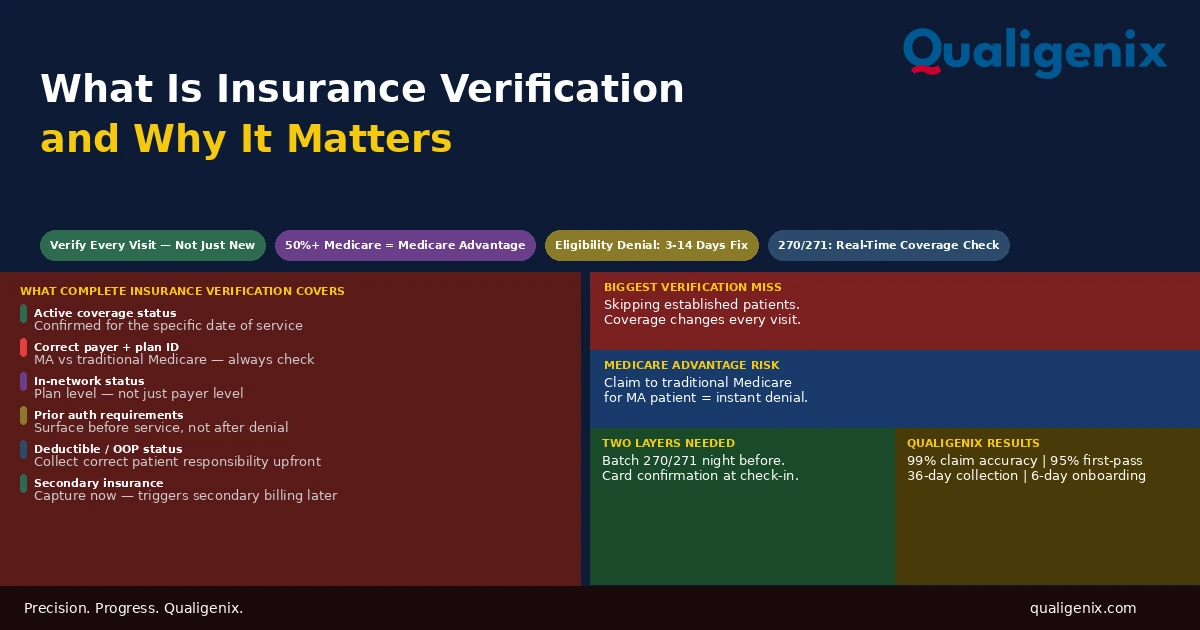
What Is Insurance Verification and Why It Matters
Insurance verification is the front-end process that determines whether a claim will be paid before the patient ever enters...

Insurance Denial Appeals: What Practices Miss
Most insurance denial appeals that fail don’t fail because the clinical case was weak. They fail because the...