Medical billing KPIs every practice manager should track in 2026
The Qualigenix Editorial Team consists of certified billing and coding experts with over 40 years of experience across 38+ medical specialties. Our content is rigorously researched against CMS, AMA, and payer-specific guidelines to ensure total compliance and accuracy. We apply the same elite standards to our resources as we do our client work, consistently delivering high claim accuracy and significant reductions in AR days.

Most practices track too many metrics and act on too few. The KPIs that actually protect revenue in 2026 are days in AR, first-pass acceptance rate, denial rate, net collection rate, clean claim rate, and AR aging over 90 days. Benchmark each against MGMA specialty data, assign a named owner per metric, and review them on a fixed weekly or monthly schedule.
A practice manager at a multi-provider orthopedic group recently told us that her billing team was generating 47 different reports each month. Nobody read most of them. Meanwhile, their denial rate had crept past 12% over six months without anyone catching it until a payer audit flagged the issue.
This is the KPI trap: tracking everything, acting on nothing. The fix isn’t more data. It’s knowing which six or seven numbers actually tell you whether your revenue cycle is healthy, and checking them on a schedule that gives you time to intervene before problems compound.
This guide covers the medical billing KPIs that matter most in 2026, what good benchmarks look like, and what to do when a number goes sideways.
The medical billing KPIs every practice manager should track in 2026 are: days in AR (target: 30 to 40 days), first-pass acceptance rate (target: 95%+), denial rate (target: below 5%), net collection rate (target: 95%+), clean claim rate (target: 95%+), and AR aging over 90 days (target: below 15% of total AR). These six metrics give a complete picture of billing cycle health and are directly tied to cash flow outcomes.
Key medical billing benchmark statistics for 2026
| KPI | Industry benchmark | Warning threshold | Source |
|---|---|---|---|
| Days in AR | 30 to 40 days | Above 50 days | MGMA DataDive 2025 |
| First-pass acceptance rate | 95%+ | Below 90% | MGMA DataDive 2025 |
| Denial rate | Below 5% | Above 10% | CMS claims data 2025 |
| Net collection rate | 95%+ | Below 90% | MGMA DataDive 2025 |
| Clean claim rate | 95%+ | Below 90% | MGMA DataDive 2025 |
| AR over 90 days | Below 15% of total AR | Above 25% of total AR | MGMA DataDive 2025 |
| Cost to collect | Below 4% of net revenue | Above 7% | MGMA DataDive 2025 |
| Claim submission lag | Within 24 to 48 hours of service | More than 72 hours | Industry standard |
| Patient collection rate | Above 70% at point of service | Below 50% | MGMA DataDive 2025 |
| Qualigenix claim accuracy | 99% | N/A | Qualigenix internal data |
| Qualigenix avg. collection cycle | 36 days | N/A | Qualigenix internal data |
| Qualigenix AR days reduction | 30% reduction on avg | N/A | Qualigenix internal data |
Days in AR: the metric that tells you everything at once
Days in accounts receivable tells you how long, on average, it takes to collect payment from the time a claim is submitted. It’s the single number that reflects the overall speed and health of your revenue cycle.
The MGMA DataDive 2025 benchmark for physician practices is 35 days. Practices running above 50 days are losing cash flow and almost always have at least one of the following problems: claims submitted too slowly, payer follow-up happening too infrequently, or a denial backlog that nobody is working down systematically.
When you pull your days in AR number, also look at what’s inside it. A high average can hide a concentrated problem. One payer with slow adjudication or one billing coder who missed a modifier consistently can drag the whole number up while the rest of your AR looks fine. Break days in AR down by payer and by provider. That breakout tells you exactly where to intervene.
How to calculate it
Divide your total outstanding AR by your average daily charges. If your practice collects $500,000 per month and your outstanding AR is $583,000, your days in AR is about 35 days. Most practice management systems calculate this automatically, but pulling it manually once a quarter is a useful sanity check.
Why does days in AR creep up slowly? Because no single claim breaks the budget. It’s the pattern — slow submission, inconsistent follow-up, appeals that sit untouched for two weeks — that compounds. By the time the number is visibly bad, months of revenue have been delayed. Review it weekly, not quarterly.
First-pass acceptance rate: your coding quality signal
First-pass acceptance rate is the percentage of claims payers accept and process on the initial submission without any corrections. The benchmark is 95% or higher. A rate below 90% means your practice is resubmitting one in ten claims, which doubles the administrative cost of billing those encounters and delays cash by weeks.
The most common culprits behind a low first-pass rate are eligibility verification failures, missing or incorrect prior authorization documentation, modifier errors, and diagnosis-to-procedure mismatches. Each of these is fixable, but only if you know which one is driving the problem.
The right response to a first-pass rate below 95% is a denial root cause analysis, not a general push to “code more carefully.” Pull the denial codes from the last 60 days, sort by volume, and identify the top three. Fix the process behind each one. That’s the only approach that moves the number.
At Qualigenix, we achieve a 95% first-pass acceptance rate across our client practices by combining upfront eligibility verification with real-time claim scrubbing before submission. The goal is to catch errors before a payer ever sees the claim, not after.
Denial rate: the number most practices underestimate
Denial rate is the percentage of submitted claims that payers reject. The industry average sits between 5% and 10%, but best-performing practices keep it below 5%. A denial rate above 10% is a revenue cycle emergency that needs immediate attention.
What makes denial rate particularly deceptive is that many practices never see the true number. If your billing system only reports on worked denials, you’re missing the ones that aged out, were written off, or were never appealed. Your real denial rate may be higher than your reports show.
Denial management in 2026 requires two separate workflows: one for working current denials within the timely filing window, and one for identifying the upstream process failures that created the denials in the first place. Working denials without fixing root causes is just expensive triage.
Net collection rate: the closest thing to a report card
Net collection rate measures the percentage of collectible revenue your practice actually receives. The calculation removes contractual adjustments (the amounts you’ve agreed to write off under payer contracts) and looks only at what you could have collected. A rate below 95% means money you were entitled to collect didn’t come in.
The gap between gross and net collection rate is often where practices lose the most revenue without realizing it. Timely filing lapses, missed appeals deadlines, and balances left in patient responsibility buckets without follow-up are the primary drivers. Each one shows up in the net collection rate before it shows up anywhere else.
Review net collection rate monthly, broken down by payer. If one payer is pulling your overall rate down, the problem is specific to their adjudication patterns, your contract with them, or your follow-up process for that payer’s claims. All three are fixable once you know which one it is.
AR aging: the early warning system you can’t ignore
AR aging categorizes your outstanding balances by how long they’ve been unpaid, typically in 30-day buckets: 0 to 30, 31 to 60, 61 to 90, and over 90 days. MGMA recommends keeping AR over 90 days below 15% of your total outstanding AR. When it climbs above 25%, collection becomes significantly harder and write-off decisions start appearing on the agenda.
Balances that age into the 91 to 120-day bucket have usually failed at least two follow-up cycles. They’re not going to resolve themselves. These require direct payer calls, appeal filings, or escalation to secondary billing. Ignoring them doesn’t make them collectible later — it makes them write-offs earlier.
One useful habit: every week, pull the claims that crossed the 90-day threshold in the last seven days. That’s your active intervention list. Assign it to a specific team member with a deadline. Accounts that get personal attention within the first week of hitting 90 days recover at a significantly higher rate than those that sit in a general aging report for another month.
Balances over 120 days are the ones that test your write-off policy. Before writing anything off, confirm that the claim was appealed at least once, that timely filing hasn’t expired, and that the balance isn’t actually a patient responsibility item sitting in the wrong bucket. Many “bad debt” write-offs are recoverable claims that got misfiled.
Clean claim rate and cost to collect: the operational efficiency pair
Clean claim rate and cost to collect work together to tell you how efficiently your billing operation runs. A clean claim rate above 95% means your team is submitting error-free claims consistently. Cost to collect below 4% of net revenue means you’re not spending more to collect a dollar than that dollar is worth.
A low clean claim rate almost always inflates cost to collect. Every claim that gets rejected and resubmitted adds staff time, delays payment, and increases the chance the claim ages past timely filing. The relationship is direct: fix clean claim rate, and cost to collect follows.
For practices evaluating whether to outsource billing, cost to collect is the most useful comparison metric. In-house billing departments often run at 6% to 8% of net revenue when you factor in salaries, software, training, and overhead. A well-run RCM partner should deliver cost to collect in the 3% to 5% range with better clean claim and denial metrics.
How Qualigenix approaches KPI management for client practices
We work with 275+ practices across 38+ specialties, and the most common gap we see isn’t a lack of data — it’s a lack of accountability structure around the data. Practices have KPI reports. They don’t have weekly review cadences, named metric owners, or documented escalation paths when a number goes outside target range.
Our revenue cycle management approach assigns every client a dedicated account lead who owns weekly KPI reviews. Days in AR and denial rate get reviewed every week. First-pass rate, net collection rate, and AR aging get a full monthly review with written commentary and action steps. If a metric moves more than 5% in the wrong direction between reviews, the client gets a same-week flag, not a monthly report.
Our medical billing services deliver a 99% claim accuracy rate, a 95% first-pass acceptance rate, a 36-day average collection cycle, and a 30% reduction in AR days across client practices.
What practice managers say about working with Qualigenix
“Our days in AR dropped from 58 to 34 in the first three months. We’d been chasing that number for two years with our previous biller. Qualigenix fixed the denial workflow in week one.”
Sarah M.
Practice Manager, Internal Medicine Group, Texas
“I finally have a denial rate I’m not embarrassed to show the physicians. We went from 13% down to 4.2% in under 90 days. The weekly KPI reports alone are worth it.”
James R.
Administrator, Multi-Specialty Clinic, Minnesota
“We were writing off balances over 90 days as a habit. Qualigenix showed us that 30% of what we were writing off was still collectible. That money is now coming in.”
Dr. Priya K.
Owner, Family Practice, Illinois
“Our net collection rate was sitting at 88%. Six months with Qualigenix and it’s at 96.4%. They found the payer contracts that were underpaying us and pushed back on adjustments we’d been accepting for years.”
Maria T.
COO, Orthopedic Practice Group, Florida
Your 10-item KPI accountability checklist
Days in AR is under 40 days and reviewed weekly
First-pass acceptance rate is at or above 95% this month
Denial rate is below 5% and trending flat or downward
Net collection rate is at or above 95% for the last 90 days
AR over 90 days is below 15% of total AR
Clean claim rate is at or above 95%
Cost to collect is below 4% of net revenue
Each KPI has a named owner on the billing team
A denial root cause log is updated monthly
Claims crossing the 90-day threshold are flagged weekly for direct intervention
Frequently asked questions about medical billing KPIs
What is a good first-pass acceptance rate for medical billing?
A first-pass acceptance rate above 95% is the MGMA benchmark. Qualigenix achieves 95% across client practices through upfront eligibility verification and pre-submission claim scrubbing. Anything below 90% signals a systematic coding or eligibility problem that needs root cause analysis, not just resubmission.
What should days in AR be for a medical practice?
Most benchmarks place the target at 30 to 40 days. MGMA data shows the median for physician practices is around 35 days. Practices running above 50 days are losing cash flow and should audit their billing workflows, submission lag, and follow-up cadences by payer.
What is the average medical billing denial rate?
The national average sits between 5% and 10%. Best-performing practices stay below 5%. A rate above 10% points to eligibility verification failures, coding errors, or missing authorization documentation and should trigger an immediate root cause review.
What is net collection rate and why does it matter?
Net collection rate measures the percentage of collectible revenue your practice actually collects after contractual adjustments. A rate below 95% means money you were entitled to receive didn’t come in. Timely filing lapses and unworked patient balances are the most common causes.
How often should practice managers review billing KPIs?
Days in AR and denial rate should be reviewed weekly. First-pass rate and net collection rate should be reviewed monthly. Reviewing too infrequently means problems compound for weeks before anyone catches them. Build the review into a fixed meeting, not an ad hoc pull.
What causes high days in AR?
High days in AR usually traces back to slow claim submission, poor denial follow-up, inadequate payer contract management, or patient balance collections that aren’t happening at point of service. Break the number down by payer and provider to identify which bucket is the primary driver.
Should practices track AR over 90 days separately?
Yes. AR over 90 days is one of the most useful sub-metrics in revenue cycle management. MGMA recommends keeping it below 15% of total AR. Balances that age past 120 days become significantly harder to collect and often require write-off decisions that wouldn’t be necessary with earlier intervention.
What is clean claim rate and how is it different from first-pass acceptance rate?
Clean claim rate measures the percentage of claims submitted with zero errors. First-pass acceptance rate measures the percentage of those claims a payer then accepts and processes. A clean claim rate problem is upstream — it’s in your billing team’s submission process. A first-pass rate problem can also involve payer adjudication behavior. Track both separately.
Related resources
- Qualigenix Medical Billing Services — how we manage claims end-to-end
- Denial Management Services — denial tracking, root cause analysis, and appeals
- Revenue Cycle Management — full-cycle RCM for practices across 38+ specialties
- MGMA DataDive — industry benchmark source for specialty-specific KPI targets
- CMS.gov — Medicare claims and billing guidance
Your billing KPIs should be moving in the right direction every month
If your days in AR is climbing, your denial rate is above 5%, or your net collection rate has slipped below 95%, those numbers won’t fix themselves. The practices that protect revenue in 2026 are the ones with a consistent review cadence, named metric owners, and a billing partner who flags problems before they show up in the next month’s report.
Qualigenix delivers 99% claim accuracy, a 95% first-pass acceptance rate, an average 36-day collection cycle, and a 30% reduction in AR days. We onboard new clients in as few as 6 days.
What’s Next

Denial Management in 2026: The Top 10 Codes and the Appeal Playbook for Each
Denials cluster around a small set of codes, and each one has a different correct response. Some need a...
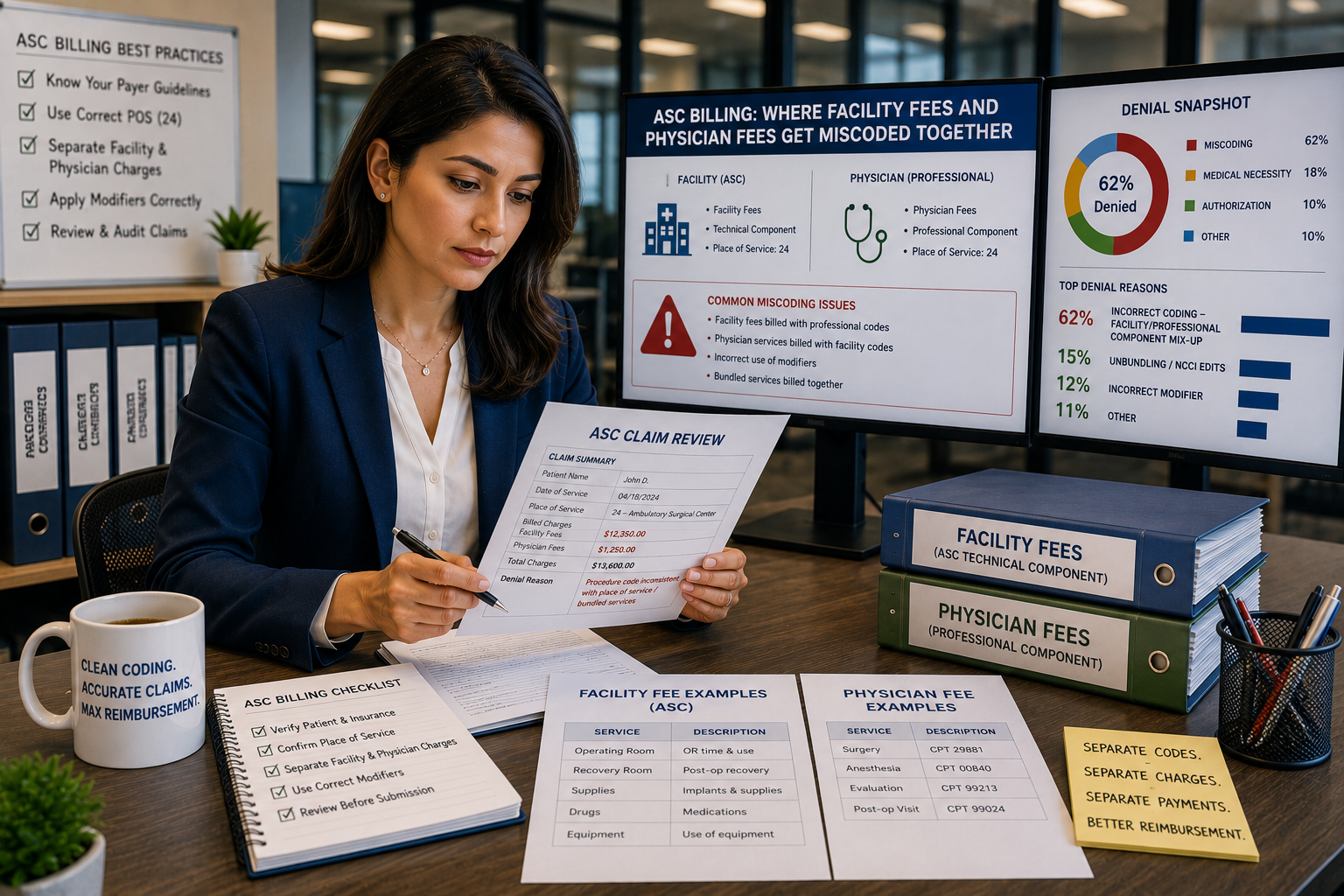
ASC Billing: Where Facility Fees and Physician Fees Get Miscoded Together
ASC facility and physician claims both go out on a CMS-1500 form with the same CPT code and place...
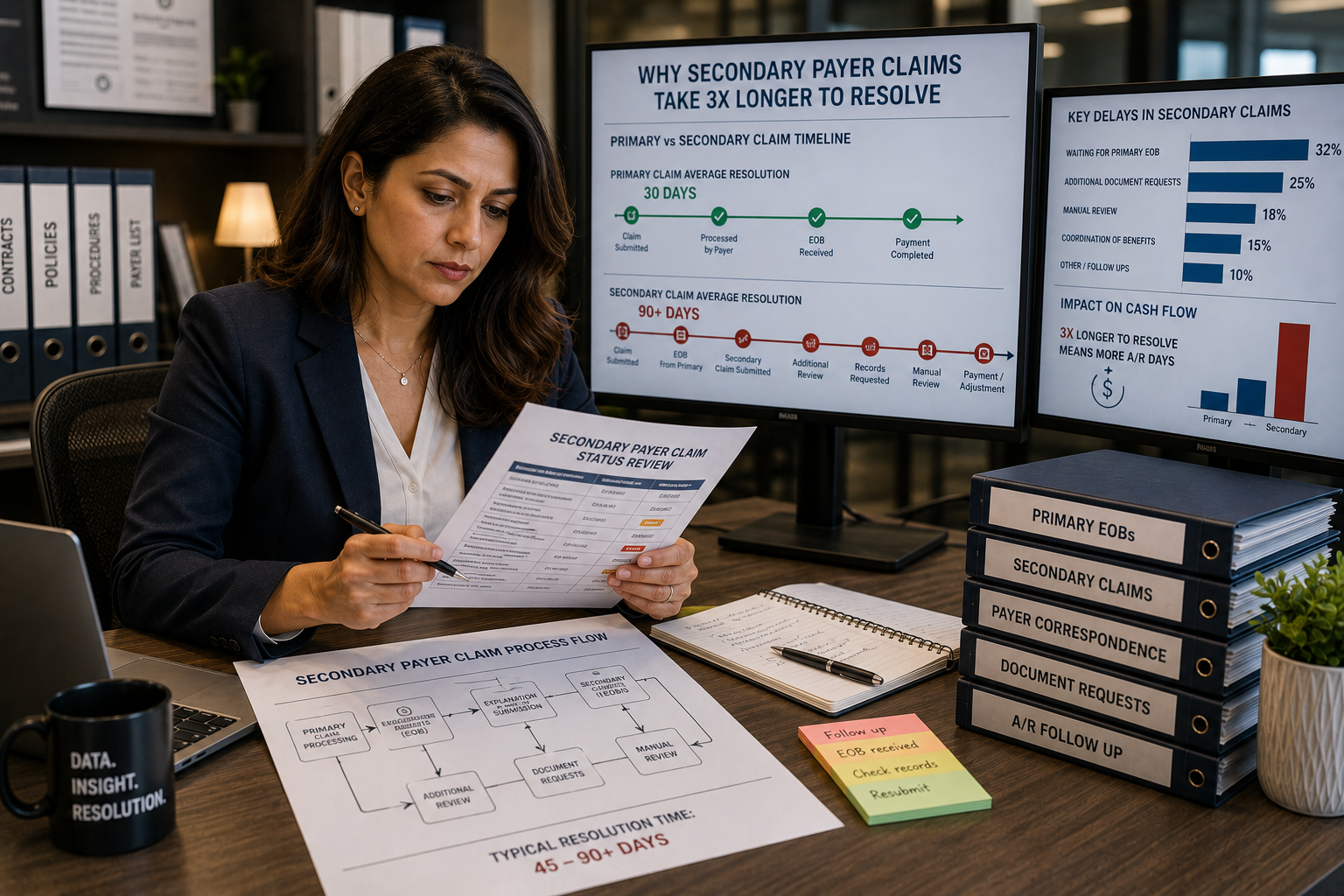
Coordination of benefits errors: why secondary payer claims take 3x longer to resolve
Secondary payer claims stall because coordination of benefits errors, wrong payer order, outdated COB records, and missing primary...