Medical Billing and Medical Coding: What’s the Difference?
The Qualigenix Editorial Team comprises certified medical billing professionals, CPC-credentialed coders, prior authorization specialists, and revenue cycle consultants with more than 40 years of combined hands-on experience serving solo physicians, group practices, hospitals, and ASCs across 38+ specialties in the United States. Every guide, article, and resource published on the Qualigenix blog is researched against current CMS guidelines, Federal Register notices, AMA policy updates, and payer-specific billing rules — and reviewed for compliance accuracy before publication. Our content reflects the same standards we apply to our client work: 99% claim accuracy, 95% first-pass acceptance, and a 30% average reduction in AR days.
Every time you walk out of a clinic, a hidden process begins. This process determines how your claim is processed, how fast your provider is paid, and whether you face unexpected bills. Yet few people understand the real difference between medical billing and coding, even though errors in either cost the U.S. healthcare system over $262 billion a year. They even cause nearly 30% of insurance claims to be denied on first submission. And that’s not just paperwork. It affects care access, provider revenue, and patient trust.
This guide breaks down how medical coding and billing work, why both are important for revenue integrity, and how CPT vs ICD-10 codes shape claim submission. You will also learn how clean documentation and accurate workflows prevent costly billing errors.
Medical Coding and Billing: Roles, Skills, and Handshakes
Behind every paid healthcare claim are two teams working in sync: medical coders and medical billers. They’re part of the same revenue cycle but focus on different stages. Coders turn patient care details into standardized codes; billers use those codes to build and process claims. Together, they convert clinical work into cash flow. When they operate in sync, providers see faster reimbursements and fewer claim rejections. When they don’t, denials, billing errors, longer accounts receivable (AR) days, and lower clean claim rates follow.
What Coders Do (ICD-10-CM, CPT, HCPCS)
Medical coders are responsible for transforming clinical documentation into standardized language that insurers understand. They use the International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) to code diagnoses and the Current Procedural Terminology (CPT) and Healthcare Common Procedure Coding System (HCPCS) for procedures and services.
Their tasks go beyond translation:
- Coders check that documentation supports each code,
- They confirm medical necessity, and identify missing details that could cause denials later.
Solid coding supports the entire revenue cycle, as it influences prior authorization decisions, coding audits, and ultimately revenue integrity.
What Billers Do (Claims to Cash)
Medical billers step in after coding is complete. Their role is to convert those codes into claims and ensure payment is collected.
- They build and scrub claims for accuracy before submitting them electronically, often through the standard 837 claim file.
- Once payers respond, billers post payments based on Electronic Remittance Advice (ERA) or Explanation of Benefits (EOB) documents, issue patient statements, and follow up on unpaid claims.
Their vigilance determines how quickly revenue flows and how many claims avoid denial.
The Critical Handoffs
The most sensitive points in the revenue cycle are the transitions from charge capture to coding quality checks, and from coding to final claim edits. If these handoffs fail, small mistakes snowball into rejections, delayed payments, and compliance risks.
Seamless coordination between coding and billing teams ensures cleaner claims, faster adjudication by payers, and stronger overall revenue performance.
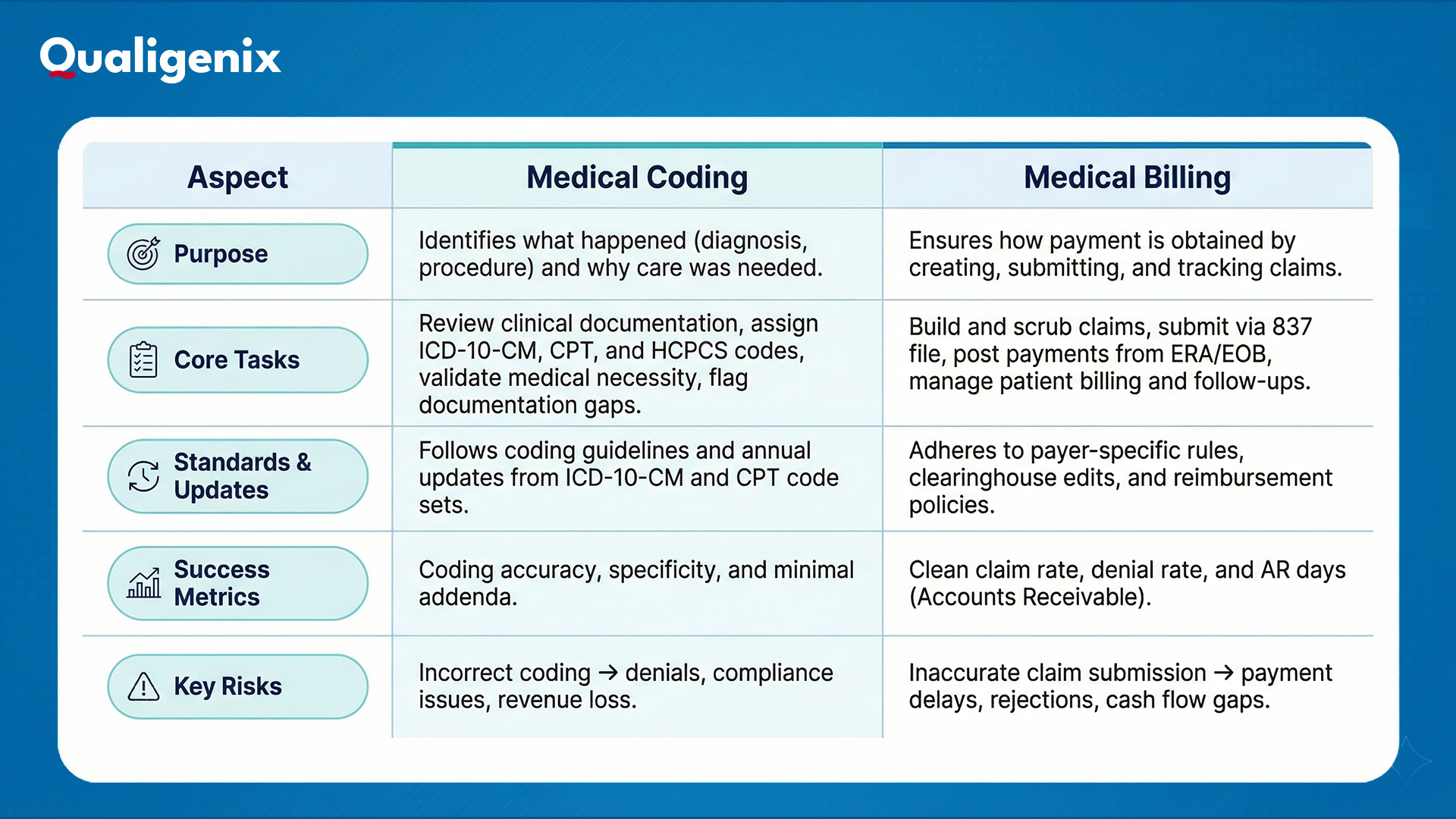
Difference Between Medical Billing and Coding: Side-by-Side
Medical billing and medical coding are deeply connected, but they serve very different functions in the revenue cycle. Coding focuses on translating care into universal codes that explain what was done and why, whereas billing turns those codes into claims and manages how payment is received. Both must stay aligned for claims to be accurate, timely, and compliant.
To make that distinction clearer, here’s how the differences between medical billing and coding compare across key aspects that matter most in everyday workflows:
CPT vs ICD-10: The Code Sets That Must Align
Medical coding is not just about assigning numbers. It tells the patient’s story in a language insurers understand. That story has two parts: what was done and why it was done. CPT and HCPCS codes explain the services performed, whereas ICD-10-CM codes explain the diagnosis or condition behind them. For a claim to get paid, these two sides must align perfectly.
“What” vs “Why”
Think of it like this: if a patient is treated for type 2 diabetes (ICD-10-CM: E11.9) and the provider orders glucose monitoring (CPT: 82947), the “what” (the service) clearly matches the “why” (the condition). But if that same code is paired with a diagnosis like sprained ankle, the mismatch will almost always trigger a denial. This alignment is the first line of defense against preventable revenue loss.
Annual Snapshot
Both code sets update every year. New codes are added, others revised, and some deleted. If your templates and workflows aren’t refreshed regularly, even the best documentation can lead to denials. For example, CPT introduced new remote monitoring codes in 2024, and ICD-10-CM added expanded mental health categories. Missing these updates can cause coding inaccuracies, payer rejections, and compliance issues.
Workflow Guardrails
Strong workflows prevent misalignment before it happens. Combining built-in code edits with payer-specific policy checks reduces errors at the source. Just as important is the coder–biller communication loop: if a coder flags documentation that doesn’t support a service, the biller must know before claim submission. That back-and-forth keeps mismatches and the denials they cause out of your revenue cycle.
Workflow Map: From Encounter to ERA/EOB
Medical billing and coding don’t happen in isolation. They’re part of a larger revenue cycle that starts the moment a patient schedules an appointment and ends when payment is fully posted. Here’s how this whole billing workflow works:
Front End
The revenue cycle begins before care is delivered. Front-end tasks include patient registration, verifying insurance eligibility, obtaining prior authorization for services, and capturing accurate charges during the encounter. A missed authorization or incorrect insurance detail here can derail claims before coding even starts.
Mid-Cycle
Once the visit is complete, the mid-cycle phase kicks in. This is where coding happens, such as translating the encounter into ICD-10-CM and CPT/HCPCS codes. Coders may issue documentation queries if details are unclear or incomplete. The claim then runs through scrubber edits to catch common errors before submission to the payer. Clean work here increases the chance of first-pass payment and improves the clean claim rate.
Back End
After submission, the claim enters payer adjudication, where the insurer reviews, approves, denies, or requests more information. Payments and adjustments are communicated through ERA or EOB, and billers post payments, send patient statements, and follow up on outstanding balances. Tracking metrics like clean claim rate and AR days here shows how healthy your revenue cycle truly is, and where you might need to tighten workflows.
Mistakes That Blur the Lines (and How to Avoid Them)
Even the best teams can slip up when coding and billing workflows aren’t tightly connected. Most denials don’t happen because people don’t care. They happen because small gaps usually lead to major problems. Below are three common trouble spots and how you can fix them before they cost time and revenue:
-
Documentation Gaps → Coding Shortcuts
When provider notes are incomplete or too vague, coders are left guessing. That often leads to broad or incorrect codes, which trigger denials or compliance risks later.
How to Fix It:
- Use query templates to quickly ask providers for missing details.
- Create specialty-specific checklists so coders know exactly what information is needed before assigning a code.
- Encourage providers to document the “what” and “why” clearly during or right after the encounter.
-
Code-Set Mismatch (CPT vs ICD-10)
If the procedure codes (CPT/HCPCS) don’t align with the diagnosis codes (ICD-10-CM), the claim will almost always be denied. It’s one of the easiest mistakes to avoid, and one of the most common.
How to Fix It:
- Double-check that each service (“what”) is supported by a matching diagnosis (“why”).
- Use pre-submit edits in your billing software to catch mismatches before claims go out.
- Provide regular coder training on new codes and pairing logic.
-
“Throw-Over-the-Wall” Handoffs
When coders finish their work and simply pass it along without explanation, and billers submit claims without offering feedback, communication gaps allow errors to slip through.
How to Fix It:
- Hold short weekly huddles where coders and billers review common errors and recent denials together.
- Share denial analytics so both teams see the same data and trends.
- Build a feedback loop: coders explain complex coding decisions, and billers share payer responses.
How Qualigenix Helps Align Medical Billing and Coding in Practice
Even with strong teams, keeping coding accuracy and billing efficiency in sync can be tough. Qualigenix was built to bridge that gap. We are aligning clinical detail with payment reality so every claim moves smoothly from documentation to dollars.
Why Qualigenix
Qualigenix helps healthcare organizations connect coding precision with billing throughput by embedding payer-specific edits directly into workflows and coaching teams on stronger documentation practices. The result is fewer denials, cleaner claims, and a more predictable revenue stream.
What You Get
Our approach combines audit, automation, and analytics. You get a code-to-claim audit that uncovers missed revenue, a scrubber rule pack tuned to your payers, measurable clean-claim uplift, and a unified KPI dashboard tracking clean claim rate, denial rate, and AR days in real time.
How We Deliver
We roll out improvements in clear, manageable phases, a 30-60-90 day plan that starts with quick wins and builds toward long-term gains. Our EHR-agnostic connectors integrate easily with your existing systems, and monthly executive readouts keep leadership aligned on progress and performance.
Sync Billing and Coding to Strengthen Your Revenue!
There are some differences between medical billing and coding, but revenue depends on how well they work together. Keep code sets updated, standardize coder–biller handoffs, and track KPIs like clean claim rate, denial rate, and AR days. When both functions operate as one system, claims flow smoothly, payments arrive faster, and revenue integrity stays strong.
Ready to turn coding accuracy and billing efficiency into real financial performance? Partner with Qualigenix to align both ends of your revenue cycle, and watch your claims get paid faster.
FAQs
1. Is coding or billing done first?
Coding is done first. After the provider documents the encounter, coders assign ICD-10-CM, CPT, and HCPCS codes for diagnoses and services. Billers then use those codes to create the claim, submit it to the payer, and manage payment follow-up.
2. Can one person do both coding and billing?
Yes, especially in small practices. One person can manage both coding and billing if workflows are clearly structured. Detailed checklists, routine internal audits, and denial reports help catch missed edits and maintain accuracy across both functions.
3. What yearly updates should coding and billing teams watch?
CPT code updates are released every January, and ICD-10-CM updates take effect each October. Teams should also track payer policy changes and clearinghouse edit updates throughout the year to avoid rejections and compliance issues.
4. What KPIs show that the coder–biller handoff is healthy?
Strong handoffs are reflected by a high clean claim rate, low initial denial rate, and reduced AR days. Coding audit accuracy is another key signal, showing that documentation and code selection align correctly before claims are submitted.
5. How do CPT and ICD-10 codes work together?
CPT codes describe what service or procedure was performed, and ICD-10-CM codes explain why it was medically necessary. Both must align correctly. Mismatched codes often lead to denials, delayed payments, and revenue leakage.
What’s Next
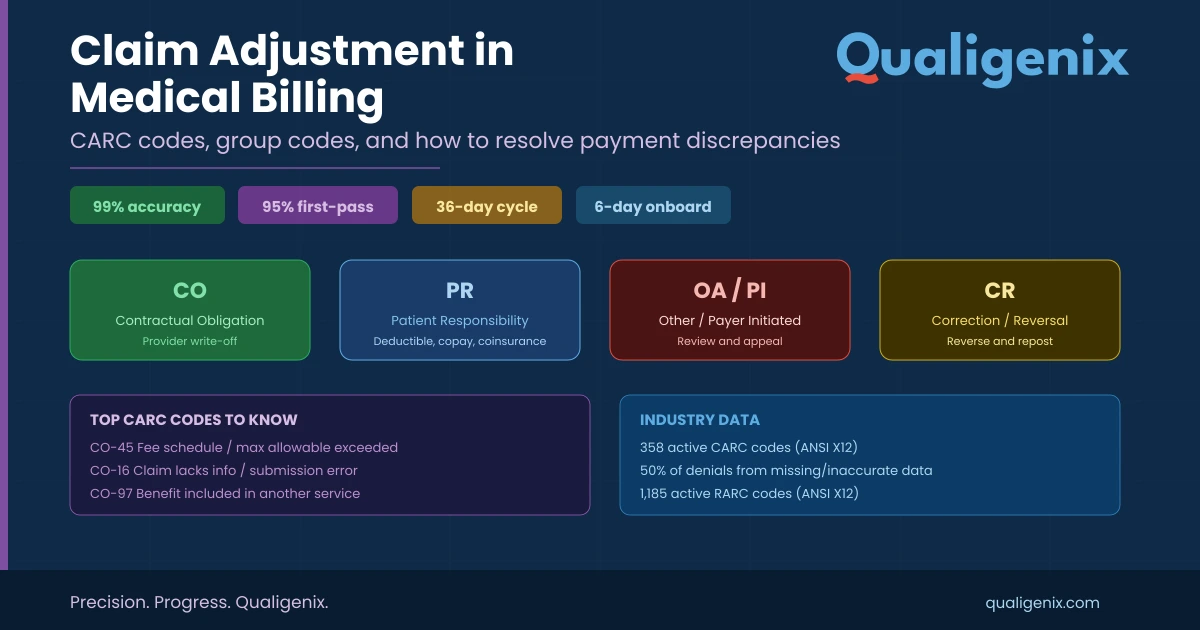
Claim Adjustment in Medical Billing: CARC Codes, Group Codes, and How to Resolve Payment Discrepancies
A claim adjustment occurs when a payer changes the reimbursement amount from what was originally billed. Every adjustment is...
Medical Necessity Documentation Mistakes to Avoid
A claim can look perfect in your billing system, then fall apart the moment a payer asks for records....
Denial Management in Medical Billing: 7 Common Causes
A patient visits your clinic, receives care, and leaves reassured. The service is documented, the claim is submitted, and...