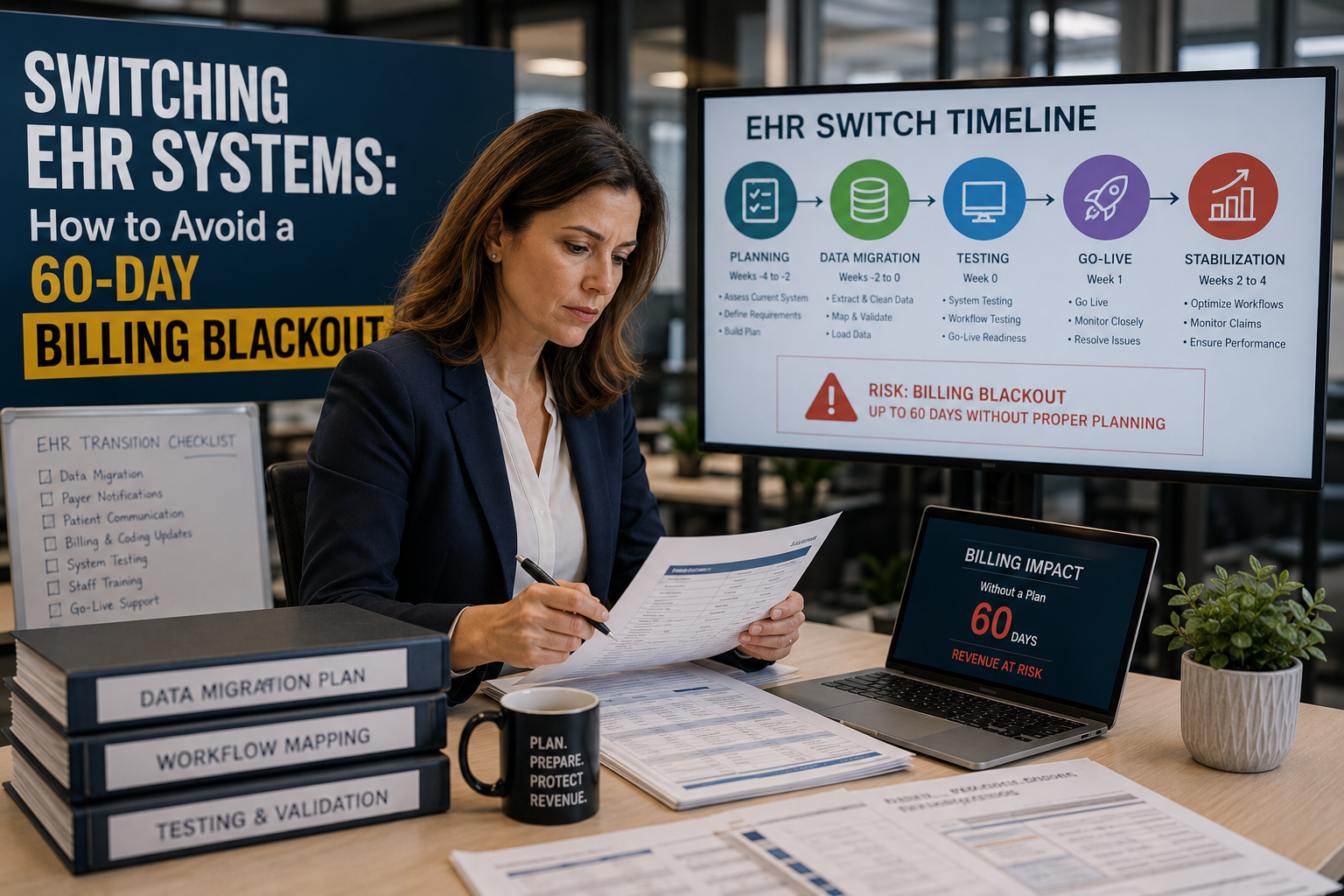
Switching EHR Systems: How to Avoid a 60-Day Billing Blackout
The Qualigenix Editorial Team consists of certified billing and coding experts with over 40 years of experience across 38+ medical specialties. Our content is rigorously researched against CMS, AMA, and payer-specific guidelines to ensure total compliance and accuracy. We apply the same elite standards to our resources as we do our client work, consistently delivering high claim accuracy and significant reductions in AR days.
An EHR switch does not have to cost you two months of cash flow. The blackout comes from three gaps: clearinghouse re-enrollment that starts too late, financial data that migrates after clinical data instead of before it, and no one watching AR closely for the first 30 days post-go-live. Run parallel billing for 30 to 45 days, and the blackout shrinks to a manageable dip.
Most practices plan an EHR switch around the clinical side. New charting tools, better scheduling, a nicer patient portal. Billing gets a line item and a “we’ll figure it out” attitude. Then the go-live date passes, claims stop moving the way they used to, and six weeks later someone in finance is asking why collections dropped 30%.
That gap has a name in revenue cycle circles: a billing blackout. It is not one big failure. It is three smaller ones happening at once, coding errors from staff still learning the new system, clearinghouse connections that were not tested before go-live, and historical AR data that got lost or mismapped in the migration.
None of that is unavoidable. Practices that treat billing continuity as its own project, separate from the clinical rollout, cut the disruption from months down to days. This guide walks through what actually causes the blackout and the cutover plan that prevents it.
A billing blackout during an EHR switch happens when claim submission, payment posting, and denial follow-up stall at the same time. You avoid it by running parallel billing for 30 to 45 days, re-enrolling with your clearinghouse before go-live instead of after, and migrating financial data ahead of clinical history.
Why an EHR switch turns into a billing blackout
The mechanics are predictable once you have seen them a few times. Your coding staff learns a new charge capture screen, and in the first two to three weeks they miss modifiers or select the wrong diagnosis pointer. Those claims still go out, but they come back denied 20 to 40 days later, right when everyone thought the transition was over.
At the same time, your clearinghouse connection often needs to be rebuilt. A new EHR usually means a new practice management module, which means new EDI credentials and new payer ID mappings. If that setup starts after go-live instead of before it, claims sit in a queue with nowhere to go.
Industry data backs up how common this is. Denial rates industry-wide run 6% to 13%, and 41% of providers now report denial rates above 10%, up from 30% in 2022. A poorly timed EHR switch pushes a practice toward the high end of that range right when cash flow matters most.
Quick answer: How do I know if my practice is at risk of a blackout? If your current denial rate sits above 8%, your clean claim rate is below 93%, or your days in AR already exceed 40, an EHR switch will likely widen those numbers before it improves them. Fix what you can before go-live.
Build a parallel billing bridge before you flip the switch
Parallel billing means your old system stays open for one job only: working the claims that were already in flight when you switched. New charges move through the new EHR from day one. Nobody is trying to run both systems for everything, just splitting the workload so nothing falls through.
This takes a dedicated owner. Whoever manages the legacy AR should not also be learning the new coding workflow at the same time. Split the assignment, even temporarily, or bring in outside support for the bridge period specifically.
Thirty to 45 days is the typical window. Shorter than that and you risk closing out claims that still need follow-up. Longer, and you are paying to maintain two systems without a clear end date. Set the close date when you plan the switch, not after you are already in the middle of it.
The 90-day cutover timeline that keeps claims moving
A practical timeline breaks into three phases: before go-live, the parallel window, and the 30-day monitoring period after cutover closes. Here is the order that protects billing continuity:
- Days -60 to -45: Audit your current denial rate, clean claim rate, and days in AR. This baseline is what you compare against later.
- Days -45 to -14: Start clearinghouse re-enrollment and payer ID mapping. Test electronic remittance advice delivery before go-live, not after.
- Days -14 to 0: Migrate financial and demographic data first. Test claim submission in a sandbox environment if your vendor offers one.
- Go-live to Day 45: Run parallel billing. New claims through the new EHR, legacy AR follow-up on the old system.
- Day 1 to Day 30 post-go-live: Check denial rate, clean claim rate, and AR daily, not weekly. New-system denial patterns usually surface between day 20 and day 40.
- Day 45 to Day 90: Close the legacy system once open claims hit zero or formal write-off, and reconcile total collections against your baseline.
Clearinghouse and payer re-enrollment: the step everyone underestimates
This is where most timelines go wrong. Practices budget a week or two for clearinghouse setup when it typically takes two to six weeks per payer connection, longer for Medicare and Medicaid. Every payer needs its own EDI enrollment confirmed, and remittance files need to route correctly before a single claim goes out clean.
CMS added new pressure to this timeline in 2026. Under CMS-0057-F, impacted payers must now decide standard prior authorization requests within seven calendar days and expedited requests within 72 hours, with a specific reason required for every denial. That is good news for practices once it is running, but it means your prior auth workflow in the new EHR needs to be configured and tested against those windows before go-live, not discovered during it.
Quick answer: How long does clearinghouse re-enrollment actually take? Plan for two to six weeks per major payer connection, with Medicare and Medicaid often at the longer end. Start this the same week you sign your new EHR contract, not the week before go-live.
Data migration checkpoints that protect your AR
Migrate in this order: active insurance information, guarantor and demographic records, open claim status, then clinical history. A missing insurance ID or an unmapped payer field will stop a claim before it ever reaches a payer, and that error is invisible until the claim rejects.
Build a checkpoint audit after each migration phase. Pull a sample of 50 to 100 patient accounts and manually verify insurance data, guarantor fields, and open balances matched between old and new systems. Catching a mapping error in a sample of 100 costs an afternoon. Catching it after 3,000 claims have gone out costs a quarter.
Not every record needs to move on day one. Historical clinical notes from years back can often wait for a phased migration. Financial data connected to open or recent claims cannot wait. Prioritize accordingly.
In-house cutover vs. a managed parallel billing bridge
Some practices run the entire transition with existing staff. It can work for a small, low-complexity switch. For most practices, especially multi-location groups, the math favors bringing in dedicated support for the bridge period.
| Factor | In-House Cutover | Managed Parallel Billing |
|---|---|---|
| Staff bandwidth | Same team learns new EHR and works legacy AR at once | Dedicated team works the bridge while staff focuses on clinical rollout |
| Clearinghouse setup | Often starts after go-live, once problems appear | Starts 45 to 60 days before go-live |
| AR monitoring cadence | Weekly, if consistent | Daily through the first 30 days post-go-live |
| Typical AR impact | Days in AR often climb past 45 to 50 for six to eight weeks | Days in AR typically held under 35 through the transition |
What this costs you if you get it wrong
Denial rework is not cheap even outside a transition. Premier estimates U.S. hospitals spend about $19.7 billion a year overturning denials, at roughly $57 per reworked claim. MDaudit’s 2026 data shows denied inpatient dollar amounts climbing 12% year over year and denied outpatient amounts up 14%. An EHR switch without a plan tends to push a practice toward those higher numbers right when it can least afford the hit.
Quick answer: Is it ever worth switching EHR systems mid-year? Yes, if your current system is actively costing you revenue through denials or workflow breakdowns, the ongoing cost can outweigh the disruption of imperfect timing. Compare the two costs directly instead of defaulting to “wait until January.”
Key Statistics: EHR Migration and Denial Benchmarks (2026)
| Metric | Value | Source |
|---|---|---|
| Industry-wide claim denial rate range | 6% to 13% | EHR Source, 2026 |
| Providers reporting denial rates above 10% | 41%, up from 30% in 2022 | Experian Health, State of Claims 2025 |
| Average initial denial rate, 2024 | 11.8% | Experian Health / MDaudit |
| Denials considered preventable | 90% | EHR Source, 2026 |
| Denied claims never resubmitted | 65% | EHR Source, 2026 |
| Clean claim rate, top-performing practices | 97% to 98% | EHR Source, 2026 |
| Clean claim rate flag threshold | Below 90% | EHR Source, 2026 |
| Days in AR benchmark, integrated systems | Under 35 days | EHR Source, 2026 |
| Days in AR risk threshold | Above 40 days | EHR Source, 2026 |
| U.S. hospital spend fighting denials annually | $19.7 billion | Premier Inc., 2026 |
| Average cost to rework one denied claim | $57 | Premier Inc., 2026 |
| YoY increase in denied inpatient dollar amounts | +12% | MDaudit, 2026 |
| YoY increase in denied outpatient dollar amounts | +14% | MDaudit, 2026 |
| CMS standard prior authorization decision window | 7 calendar days | CMS-0057-F, effective Jan. 1, 2026 |
| CMS expedited prior authorization decision window | 72 hours | CMS-0057-F, effective Jan. 1, 2026 |
| Healthcare organizations using AI in RCM | 63% | RCM Insider, June 2026 |
| Providers reporting more prior auth requirements YoY | 89% | 2024 MGMA survey |
| Medical necessity denial growth, YoY | +18% | 2026 CAQH Index |
How Qualigenix supports practices through an EHR switch
At Qualigenix, we build the parallel billing bridge as its own workstream, separate from your clinical go-live plan. We handle clearinghouse re-enrollment and payer ID mapping before your cutover date, not after. Our team tracks denial rate, clean claim rate, and AR daily through the first 30 days post-go-live, because that is the window where new-system problems surface.
We work across 38+ specialties and 275+ practices, which means we have seen the coding gaps that specific EHR platforms tend to expose before they show up in your denial reports. If you are planning a switch, or already in the middle of one and watching AR climb, our medical billing services team can build the bridge plan around your timeline. If credentialing and payer enrollment also need attention during the transition, our credentialing services team handles that in parallel.
What practice managers say about working with Qualigenix
“We switched from an old server-based system to a cloud EHR and braced for a rough quarter. Qualigenix ran parallel billing for six weeks and our days in AR never moved past 33. No blackout, no scramble.”
Denise Callahan
Practice Administrator, Family Medicine, Ohio
“Our clearinghouse re-enrollment alone would have taken our staff a month to sort out. Qualigenix had it mapped and tested two weeks before go-live, so our clean claim rate held at 96% through the whole cutover.”
Marcus Webb
Director of Operations, Orthopedics, Texas
“Across our four locations, the EHR migration exposed a coding gap we did not know we had. Qualigenix caught it in the first ten days post-go-live and our denial rate stayed under 6% instead of spiking like it did at a sister practice that switched without support.”
Priya Nair
Multi-Site Billing Manager, Dental Service Organization, Georgia
“I switched EHR systems once before without help and lost almost two months of clean cash flow. This time Qualigenix built the parallel billing bridge and our collections for the transition quarter came in only 4% below baseline instead of the 30% drop we saw last time.”
Aaron Kessler
Practice Owner, Behavioral Health, North Carolina
10-point checklist before your EHR go-live date
- ☐ Baseline denial rate, clean claim rate, and days in AR documented
- ☐ Clearinghouse re-enrollment started 45 to 60 days before go-live
- ☐ Payer ID mapping tested for every active payer connection
- ☐ Electronic remittance advice delivery confirmed in the new system
- ☐ Financial and demographic data migrated and spot-checked before clinical history
- ☐ Parallel billing owner assigned, separate from clinical rollout staff
- ☐ Close date set for the parallel billing window
- ☐ Daily AR monitoring plan in place for the first 30 days post-go-live
- ☐ Prior authorization workflow configured against CMS-0057-F timelines
- ☐ Reconciliation date set to compare post-switch collections against baseline
Frequently Asked Questions
How long does a billing blackout last during an EHR switch?
Most unmanaged transitions see 30 to 60 days of disrupted billing. A parallel billing plan started 30 to 45 days before go-live typically cuts that window to under two weeks.
What is parallel billing during an EHR migration?
It means running claim follow-up for in-flight claims on your old system while new claims move through the new EHR. It keeps existing AR from stalling while staff learns the new workflow.
Do I need to re-enroll with my clearinghouse when I switch EHR systems?
Yes, in nearly every case. A new EHR usually means new EDI credentials and payer ID mapping, which can take two to six weeks and should start before go-live.
What data should migrate first to protect billing?
Financial and demographic data before clinical history. Active insurance information, guarantor records, and open claim status matter most in the first 30 days.
How much revenue does a practice lose during a bad EHR transition?
It depends on payer mix and starting denial rate, but practices already above an 8% denial rate before the switch tend to see the sharpest drop. The new system exposes coding gaps the old one absorbed silently.
Should I switch EHR systems mid-year or wait?
A natural breakpoint lowers risk, but it is not always the right call. If your current system is actively costing you revenue, weigh that cost directly against the transition risk instead of defaulting to “wait.”
Can outsourcing billing during an EHR switch prevent a blackout?
Yes. A dedicated RCM partner can run the parallel billing bridge and manage re-enrollment without pulling staff away from the clinical rollout. Qualigenix builds this into every EHR transition engagement.
What is the biggest mistake practices make when switching EHR systems?
Treating go-live as the finish line instead of the start of a 30-day monitoring period. Denial patterns from a new system usually surface 20 to 40 days after cutover, so that window needs daily attention, not a monthly report.
Related Resources
- Qualigenix Medical Billing Services
- Qualigenix Credentialing and Payer Enrollment
- Denial Management Services
- More Revenue Cycle Insights on the Qualigenix Blog
Planning an EHR Switch? Protect Your Cash Flow First
Qualigenix builds the parallel billing bridge before your go-live date, not after the problems start.
Our team delivers 99% claim accuracy, a 95% first-pass acceptance rate, an average 36-day collection cycle, and a 30% reduction in AR days. We onboard in as few as 6 days.
Precision. Progress. Qualigenix.
What’s Next

Running billing across multiple DSO locations: centralize or keep it site-by-site?
Full centralization wins on cost and denial rate once a DSO passes about 10 to 12 locations. Below...
Behavioral health billing: why session caps and auth renewals break more claims than coding errors
Session caps and late authorization renewals deny more behavioral health claims than CPT or modifier mistakes. Once a patient...

Home Health Billing Under PDGM: Where 30-Day Periods Quietly Cost You Revenue
PDGM pays home health agencies by the 30-day period, and every period gets scored independently on admission source,...