Home Health Revenue Cycle Management Challenges & Solutions
The Qualigenix Editorial Team comprises certified medical billing professionals, CPC-credentialed coders, prior authorization specialists, and revenue cycle consultants with more than 40 years of combined hands-on experience serving solo physicians, group practices, hospitals, and ASCs across 38+ specialties in the United States. Every guide, article, and resource published on the Qualigenix blog is researched against current CMS guidelines, Federal Register notices, AMA policy updates, and payer-specific billing rules — and reviewed for compliance accuracy before publication. Our content reflects the same standards we apply to our client work: 99% claim accuracy, 95% first-pass acceptance, and a 30% average reduction in AR days.
Home health agencies operate within one of the most volatile financial environments in healthcare. The pressure from Medicare-driven regulations has intensified significantly in recent years. The Patient-Driven Groupings Model (PDGM) completely reshaped how agencies are reimbursed. Scrutiny over clinical documentation has reached unprecedented levels. These factors make home health revenue cycle management a complex puzzle that many providers struggle to solve.
Agencies can no longer rely on volume alone to sustain revenue. Every dollar now depends on precision. A single missing signature or a late assessment can trigger a full denial. This reality forces administrative leaders to rethink their entire approach to billing. The financial health of an agency depends on its ability to adapt. This guide explores the specific hurdles facing home-based care providers today. It also outlines the operational shifts required to secure cash flow in 2026.
What Is Home Health Revenue Cycle Management
Home health revenue cycle management is the entire financial lifecycle of a patient episode. It begins the moment a referral arrives and concludes only when the agency retains the final payment after an audit. This process requires the synchronization of clinical care with financial administration.
Teams must manage intake and authorization. They must also handle OASIS documentation review and final billing. Every step connects to the next. A failure in the intake process inevitably leads to a failure in collections. Successful management ensures that the care provided translates into revenue received. It protects the agency from regulatory penalties and provides the capital needed to maintain high-quality patient care.
How Home Health RCM Differs From Other Specialties?
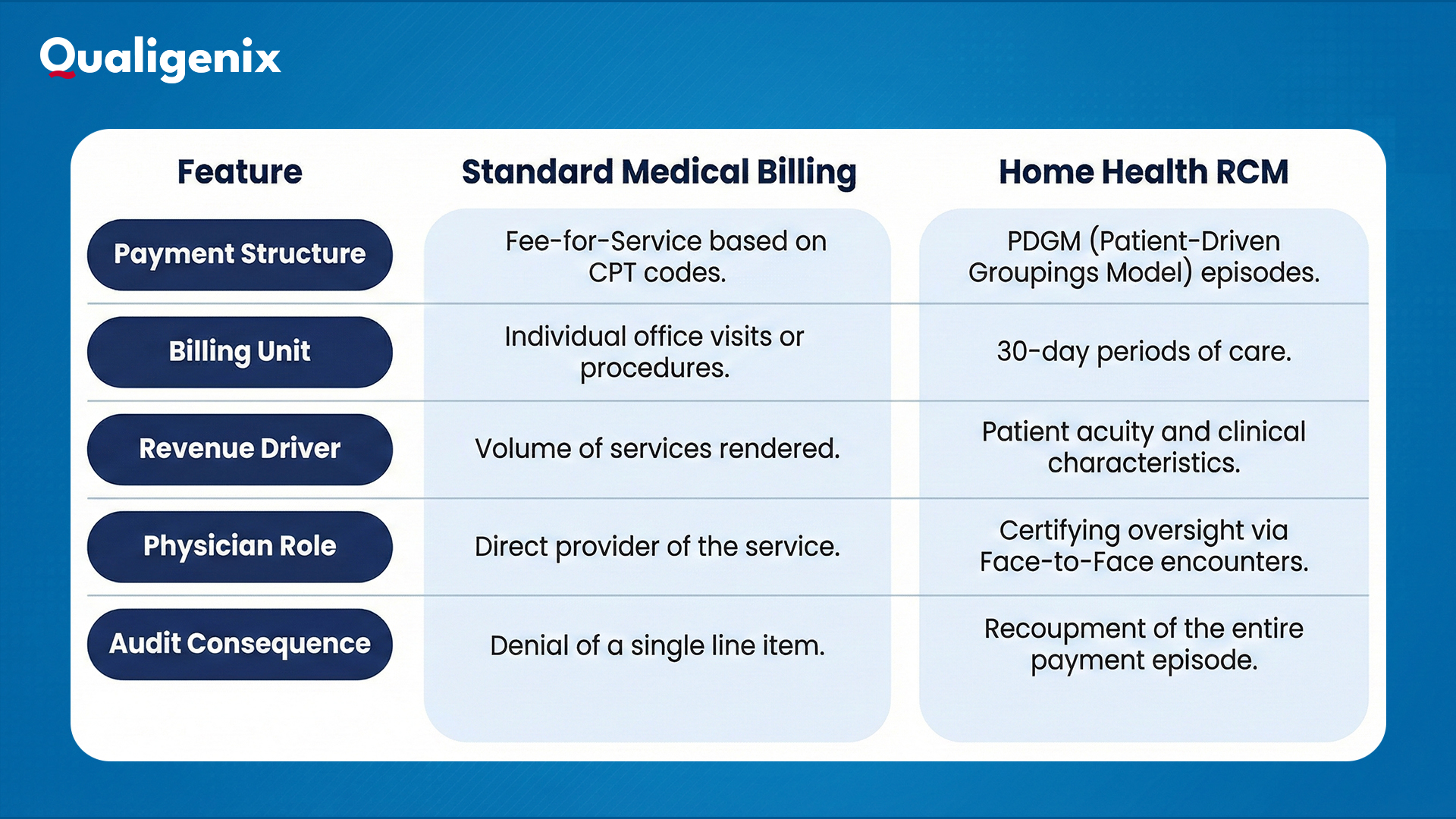
Traditional providers bill for isolated events similar to a retail transaction. Home health agencies must manage financial risk over 30-day episodes where a single documentation error can invalidate an entire month of revenue. The table below outlines these critical operational distinctions.
Key Challenges in Home Health Revenue Cycle Management
Revenue leakage in home health rarely stems from a single cause. It usually results from a series of operational disconnects. Most denials originate from errors made weeks before the bill is even generated. Here are the common challenges you must understand to take the first step toward fixing them:
Incomplete or Late OASIS Documentation
The Outcome and Assessment Information Set (OASIS) serves as the foundation for reimbursement. It determines the clinical severity of the patient and establishes the functional impairment level. Therefore, OASIS documentation must be accurate and timely.
Many agencies struggle with the strict five-day window for completion. Clinicians focused on patient care may delay their charting. This delay halts the entire revenue cycle. You cannot generate a claim without a completed assessment. Inaccurate scoring is equally dangerous. Downcoding a patient’s condition also results in significant revenue loss. Upcoding can trigger a fraud investigation. The balance requires constant vigilance.
PDGM Case Mix and Visit Utilization Errors
The PDGM payment model ties reimbursement to specific clinical characteristics. It groups 30-day periods into payment categories. These categories depend on admission source and timing. They also depend on clinical grouping and comorbidity adjustment.
Errors in any of these variables lead to incorrect payment. Visit utilization errors also plague agencies. The Low Utilization Payment Adjustment (LUPA) threshold is a critical metric. If an agency provides fewer visits than the threshold, reimbursement drops dramatically. Providers often miss this target due to poor scheduling. They might also miss it because of unexpected patient refusals. Managing this case mix requires data-driven oversight.
Authorization and Certification Delays
Agencies cannot bill for services that were not approved. Authorization delays are a primary cause of write-offs. Managed care payers often have slow approval processes. An agency might start care assuming coverage exists. They later find out the authorization was denied.
Medicare requires a signed Plan of Care (POC). This document must cover the entire certification period. Delays in obtaining physician signatures are common. The billing team cannot drop the final claim until the doctor signs. This administrative bottleneck creates a massive backlog. It forces the agency to float the cost of care for months.
Physician Orders and Face to Face Encounter Gaps
Regulatory compliance regarding physician involvement is strict. Physician orders management creates a constant logistical burden. Every change in the care plan requires a new order. Verbal orders must be signed promptly.
The face to face encounter requirements are particularly challenging. Medicare mandates that a certifying physician must see the patient. This encounter must happen within 90 days before or 30 days after the start of care. The documentation must explicitly state why home health is necessary. It must also confirm the patient is homebound. Missing this specific document results in an automatic denial. The entire episode becomes non-billable.
High Medicare Audit and Compliance Risk
Home health agencies operate under a microscope. Compliance risk home health is higher than in almost any other sector. The Review Choice Demonstration (RCD) adds pressure in many states. Targeted Probe and Educate (TPE) audits are also common.
Auditors look for technical errors. They search for lack of medical necessity. They scrutinize therapy utilization. A failed audit leads to payment recoupment. It can also lead to exclusion from the Medicare program. This high-stakes environment demands perfection. Agencies cannot afford “good enough” documentation. They need audit-proof records.
How These Challenges Impact Cash Flow and Operations
Operational inefficiencies have tangible financial consequences. The inability to navigate these challenges destabilizes the business. It creates a cycle of scarcity that affects every department.
Growing Days in AR
Inefficient processes lead to a backlog of unpaid claims. Home health AR management becomes a crisis when balances age beyond 90 days. Cash flow slows down. The agency struggles to meet payroll obligations.
Documentation holds are the most common culprit. A claim sits in the “ready to bill” queue for weeks. It waits for a signature or an OASIS correction. These delays inflate the Days Sales Outstanding (DSO). The longer a balance sits, the harder it becomes to collect. Payers have timely filing limits. Missing these deadlines means losing the revenue forever.
Increased Write Offs and Take Backs
Home health claim denials that are not worked promptly turn into write-offs. Agencies often lack the staff to appeal every rejection. They choose to abandon smaller balances. These small losses add up to significant sums over a year.
Take-backs are even more damaging. An agency receives payment. An audit later finds an error. The payer retracts the funds. This creates a negative balance on the ledger. It distorts financial reporting. It also creates sudden cash shortages. Preventing these reversals requires front-end accuracy.
Solutions to Strengthen Home Health RCM
Agencies can overcome these hurdles with the right strategies. Success requires a shift from reactive correction to proactive prevention. Operational discipline is the key to stability.
Documentation Alignment at Point of Care
Accuracy must happen in the patient’s home. Agencies should invest in training for field clinicians. Nurses and therapists must understand how their notes impact billing. Real-time documentation checks are essential.
Electronic Health Record (EHR) systems should prompt clinicians for missing data. They should flag inconsistencies before the visit ends. This “point of care” validation reduces the need for downstream corrections. It ensures that the OASIS documentation reflects the true clinical picture. It also speeds up the timeline for claim submission.
Authorization and Certification Tracking
Structured workflows prevent authorization gaps. Intake teams should verify insurance eligibility immediately. They must obtain initial authorization before the first visit.
Technology can automate this tracking. Alerts should notify staff when an authorization is expiring. They should also trigger warnings when visit counts approach the approved limit. Dedicated staff should focus solely on physician orders management. They must relentlessly pursue signatures. They should educate referral sources on the importance of timely paperwork.
PDGM Coding Accuracy and Review
Correct coding is the linchpin of fair reimbursement. Agencies should utilize certified coding specialists. These experts understand the nuances of the PDGM payment model. They ensure that the primary diagnosis matches the reason for home health.
A pre-billing review process is critical. This review checks the HIPPS code against the clinical documentation. It verifies that the visit pattern meets the LUPA threshold and confirms that comorbidity adjustments are captured. This layer of quality assurance prevents costly visit utilization errors and maximizes the revenue entitlement for each episode.
Proactive Denial Management
Agencies must attack denials immediately. A dedicated team should monitor the remittance advice daily. They should identify trends in home health claim denials. Understanding the root cause allows for systemic fixes.
Appeals should be data-driven. The team must gather the necessary medical records to prove necessity. They must submit these appeals within the payer’s timeline. Prevention is the ultimate goal. Analyzing denial data reveals weakness in the intake or coding process. Fixing these upstream issues stops the bleeding.
How Qualigenix Helps With Home Health Revenue Cycle Management

We understand that home health is not just about billing. It is about the continuity of care and commerce. Qualigenix supports agencies by acting as a specialized extension of your financial team. We navigate the regulatory maze so you can focus on your patients.
- Our experts handle rigorous OASIS documentation validation to ensure clinical accuracy.
- We manage the complexities of the PDGM payment model to secure appropriate reimbursement.
- We deploy dedicated staff to track authorization delays and relentlessly pursue physician orders management.
- Our home health AR management strategy involves aggressive follow-up on every unpaid dollar. We identify visit utilization errors before they become write-offs.
- We build compliance risk home health protocols into every workflow we touch.
This approach reduces your audit exposure and accelerates your cash flow. It gives you the peace of mind that your revenue cycle is secure.
Conclusion
Home health revenue cycle management demands precision. It requires discipline. It necessitates a deep understanding of specialty-specific rules. The challenges of Medicare home health billing and face to face encounter requirements will not disappear. They will likely become more stringent.
Providers that tolerate documentation gaps will struggle. Those that build robust, data-driven workflows will thrive. Strengthening your revenue cycle is the best way to protect your mission. It ensures that you have the resources to care for the vulnerable patients who depend on you. Your focus belongs in the home. Our focus ensures you get paid for the vital work you do there.
FAQs
1. What makes home health revenue cycle management difficult?
It combines strict Medicare regulations, time-sensitive OASIS documentation, and the complex PDGM payment model. A single signature gap or late assessment can stall your entire cash flow.
2. How does PDGM affect home health billing?
PDGM shifts reimbursement from volume to value, grouping 30-day episodes based on clinical characteristics. It demands precise coding and careful visit management to avoid low-utilization payment adjustments.
3. Why are home health claims denied so often?
Most denials stem from technical errors like missing Face-to-Face encounter notes, unsigned Orders, or unauthorized services. These documentation gaps trigger automatic rejections from strict payers.
4. How can agencies reduce AR in home health billing?
You must prioritize front-end accuracy, ensuring OASIS and authorizations are perfect before billing. Combine this with aggressive, consistent follow-up on every unpaid claim to prevent aging.
5. Is home health RCM different from hospital billing?
Yes. Hospitals bill for specific procedures, while home health bills for 30-day episodes of care. This requires managing long-term documentation compliance rather than just transactional coding.
6. Can home health RCM be outsourced?
Absolutely. Outsourcing to specialized partners provides access to experts who navigate PDGM nuances and regulatory shifts, allowing your clinical team to focus entirely on patient care.